|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2014 | Volume
: 2
| Issue : 1 | Page : 2-6 |
|
Igbos are predominantly microsemes: A radiologic study of the orbital rims of South-Eastern Nigerians
Vitalis Chukwuma Ezeuko1, Ferdinand Akpokpomese Om'Iniabohs1, Okwudili Onochie Udemezue2
1 Department of Anatomy, School of Basic Medical Sciences, College of Medical Sciences, University of Benin, Benin, Edo, Nigeria
2 Department of Anatomy, College of Medicine, Nnamdi Azikiwe University, Nnewi Campus, Nnewi, Nigeria
| Date of Web Publication | 27-Oct-2014 |
Correspondence Address:
Vitalis Chukwuma Ezeuko
Department of Anatomy, School of Basic Medical Sciences, College of Medical Sciences, University of Benin, Ugbowo, Benin, Edo
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2315-7992.143397

Introduction: Orbital index could be defined as the percentage ratio of the orbital height to the orbital width. Aim: The purpose of the present study is to investigate the prevalent orbital class among the Igbo Ethnic group. Materials and Methods: A total number of 350 radiographic films of subjects aged between less than 1 year and 79 years were collected, comprising 217 males and 133 females, from the National Orthopaedic Hospital, Enugu, Nigeria from which orbital index was calculated. The orbits were classified accordingly based on the orbital index into microseme, mesoseme or megaseme. The frequency of each orbital class was presented in percentage. Result: The results showed that the prevalent orbital class among the Igbo Ethnic group is microseme. Conclusion and Recommendation: However, whereas microseme was found to be predominant, the other orbital classes were also found within the same population. It is recommended that further studies should be carried out in other populations to find out the incidence of different orbital classes instead of concluding that an entire population has a particular orbital class based on the mean. Keywords: Igbo ethnic group, megaseme, mesoseme, microseme, orbital index
How to cite this article:
Ezeuko VC, Om'Iniabohs FA, Udemezue OO. Igbos are predominantly microsemes: A radiologic study of the orbital rims of South-Eastern Nigerians. Ann Bioanthropol 2014;2:2-6 |
How to cite this URL:
Ezeuko VC, Om'Iniabohs FA, Udemezue OO. Igbos are predominantly microsemes: A radiologic study of the orbital rims of South-Eastern Nigerians. Ann Bioanthropol [serial online] 2014 [cited 2018 Sep 6];2:2-6. Available from: http://www.bioanthrojournal.org/text.asp?2014/2/1/2/143397 |
| Introduction | |  |
The two orbital cavities are situated on either side of the sagittal plane of the skull between the cranium and the skeleton of the face. Thus situated, they encroach about equally on these two regions. [1] Each orbital cavity essentially is intended as a socket for the eyeball but it also contains associated muscles, vessels, nerves, lacrimal apparatus, fascial strata and soft pad of fat. In a nutshell, it lodges the visual apparatus. [2] Due to the fact that it is made up of many bones and that it has fissures, foramina and canals, the orbit is said to have a very complex structure. However, the orbit is roughly pyramidal in shape with the apex located posteriorly forming the optic canal and the base located anteriorly forming the orbital margin.
The orbital margin has the form of a quadrilateral with rounded corners. It is usually in the form of a spiral; the inferior orbital margin is continuous with the anterior lacrimal crest, while the superior is continued down into the posterior lacrimal crest. The lacrimal fossa thus lies in the orbital margin.
Ezeuko et al., [3] Ferrario et al., [4] Bentley et al., [5] and Denis et al., [6] proposed that there could be a correlation between orbital width and height. This correlation could be investigated further by determining the orbital index.
Orbital index could be defined as the percentage ratio of the orbital height to the orbital width Orbital index = (Height of orbit/Width of orbit)*100
According to Patnaik et al., [7] taking the orbital index as the standard, there are three classes of orbit:
- Megaseme (large): The orbital index is >89. This type is characteristic of the yellow races, except the Eskimos. The orbital opening is round.
- Mesoseme (intermediate): Orbital index between 89 and 83. This type is found in the white races (European 87, English 88.4).
- Microseme (small): Orbital index <83. This type is characteristic of the black races. The orbital opening is rectangular.
Previous studies had classified populations based on the mean of their orbital index [8],[9] but not on the frequencies of the different types of orbital index. These, however, have a way of concealing the fact that whereas a types of orbital index could be more frequent in a population, other types of orbital index could also be found. The purpose of the present study is to investigate the prevalent orbital class among the Igbo Ethnic group.
The knowledge that would be gathered from the result will help in skull classification in forensic medicine. It will also assist anthropologists in skull identification and in the study of evolutionary trend and racial differences.
| Materials and Methods | | |
The study was carried out retrospectively in the National Orthopedic Hospital Enugu using Plain X-rays of the Water's (frontal) view of the skull [Figure 1] that were taken between 2000 and 2006.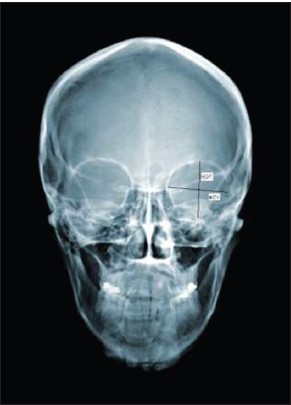 | Figure 1: Plain film showing the orbital margin and measurement of orbital width and height[3]
Click here to view |
A total number of 350 radiographic films (Water's view) of patients aged between less than 1 year and 79 years were collected, comprising 217 males and 133 females, from the National Orthopaedic Hospital, Enugu, Nigeria from which a total of 700 orbital margins were measured (350 from each side).
Measurements were only taken on skulls that were evidently healthy or, if pathology was present, from those that did not affect the dimensions of the orbit. Information on the age and gender were also gathered from the hospital cards. All cases of raised intracranial or intraorbital pressures as reported by the radiologists were discarded. The films that were selected for the study were strictly those of the Igbos based on the information given by the subjects and filled in their cards. Non-Igbos population was not included in the study.
In addition to the radiographs employed in this research, other materials that were helpful in my measurements include: an X-ray illuminator, a metre rule calibrated in millimetres and a pair of dividers.
The orbital height was measured from the frontal film as the maximal distance between the superior and inferior orbital margins. The orbital width was also measured from the same frontal film as the maximal distance between the medial and lateral orbital margins [Figure 1].
The orbital indices were calculated from the data gathered using the formula:
Orbital index = [Height of orbit/Width of orbit]*100
The orbits were classified accordingly based on the orbital index into either microseme, mesoseme or megaseme. The frequency of each orbital class was presented in percentage. The differences in frequencies were compared using Chi-square test and were statistically significant when probability is less than 0.05 (P < 0.05).
| Results | | |
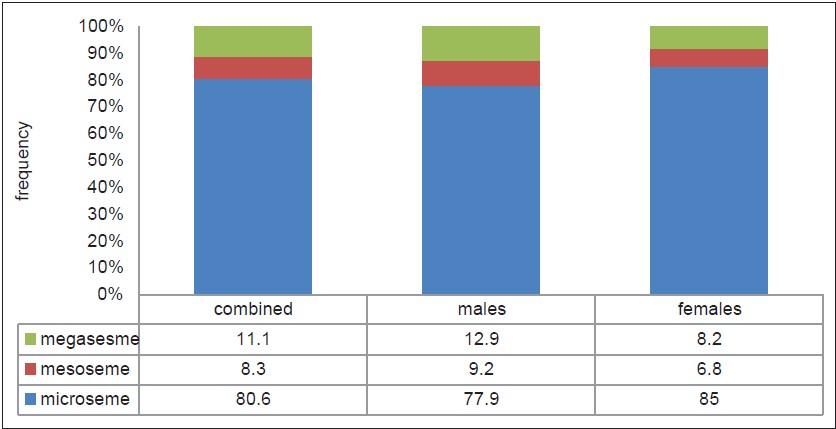
From [Figure 2], out of the 350 subjects used in the study, 80.6% orbits were of microseme class; 8.3% were of mesoseme class; 11.1% were of megaseme class. Out of the 217 male subjects used in the study, 77.9% were of microseme class; 9.2% were of mesoseme class; 12.9% were of megaseme class. Out of the 133 female subjects used in the study, 85% were of microseme class; 6.8% were of mesoseme class; 8.2% were of megaseme class. The frequencies of microsemes were significantly (P < 0.05) higher than non-microsemes in both males and females.
From [Figure 3], out of the 33 subjects aged 0-9 years, 90.9% were of microseme class; 6.1% were of mesoseme class; 3% were of megaseme class. Out of the 41 subjects aged 10-19 years, 89% were of microseme class; 7.3% were of mesoseme class; 3.7% were of megaseme class. Out of the 101 subjects aged 20-29 years, 77.2% were of microseme class; 9.9% were of mesoseme class; 12.9% were of megaseme class. Out of the 67 subjects aged 30-39 years, 76.9% were of microseme class; 6.0% were of mesoseme class; 17.1% were of megaseme class. Out of the 36 subjects aged 40-49 years, 70.3% were of microseme class; 16.2% were of mesoseme class; 13.5% were of megaseme class. Out of the 30 subjects aged 50-59 years, 74.1% were of microseme class; 10.4% were of mesoseme class; 15.5% were of megaseme class. Out of the 25 subjects aged 60-69 years, 96% were of microseme class; 0% were of mesoseme class; 4% were of megaseme class. Out of the 17 subjects aged 70-79 years, 91.2% were of microseme class; 8.8% were of mesoseme class; 0% were of megaseme class. The frequencies of microsemes were significantly (P < 0.05) higher than non-microsemes in all the age groups.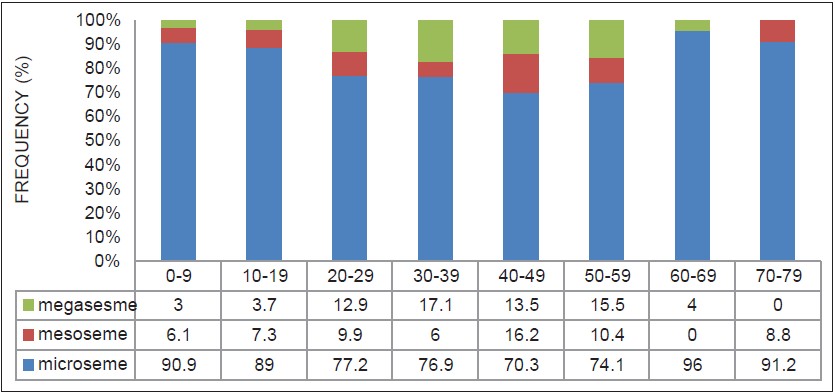 | Figure 3: Bar chart showing frequency of different classes of orbit among different age groups
Click here to view |
From [Figure 4], out of the 13 subjects aged 0-9 years, 88.5% were of microseme class; 11.5% were of mesoseme class; 0% were of megaseme class. Out of the 29 subjects aged 10-19 years, 93% were of microseme class; 3.5% were of mesoseme class; 3.5% were of megaseme class. Out of the 66 subjects aged 20-29 years, 76.5% were of microseme class; 9.9% were of mesoseme class; 13.6% were of megaseme class. Out of the 47 subjects aged 30-39 years, 69.2% were of microseme class; 8.5% were of mesoseme class; 22.3% were of megaseme class. Out of the 24 subjects aged 40-49 years, 70.8% were of microseme class; 12.5% were of mesoseme class; 16.7% were of megaseme class. Out of the 16 subjects aged 50-59 years, 71.9% were of microseme class; 15.6% were of mesoseme class; 12.5% were of megaseme class. Out of the 12 subjects aged 60-69 years, 91.7% were of microseme class; 0% were of mesoseme class; 8.3% were of megaseme class. Out of the 10 subjects aged 70-79 years, 85% were of microseme class; 15% were of mesoseme class; 0% were of megaseme class. The frequencies of microsemes were significantly (P < 0.05) higher than non-microsemes in all the age groups in males.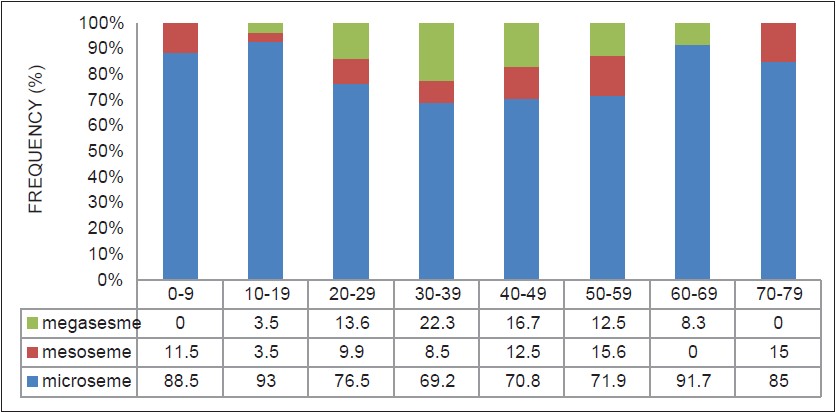 | Figure 4: Bar chart showing frequency of different classes of orbit among different age groups in males
Click here to view |
From [Figure 5], out of the 20 subjects aged 0-9, 92.5% were of microseme class; 2.5% were of mesoseme class; 5% were of megaseme class. Out of the 12 subjects aged 10-19 years, 79.2% were of microseme class; 16.6% were of mesoseme class; 4.2% were of megaseme class. Out of the 35 subjects aged 20-29 years, 78.6% were of microseme class; 10% were of mesoseme class; 11.4% were of megaseme class. Out of the 20 subjects aged 30-39 years, 95% were of microseme class; 0% were of mesoseme class; 5% were of megaseme class. Out of the 13 subjects aged 40-49 years, 69.2% were of microseme class; 23.1% were of mesoseme class; 7.7% were of megaseme class. Out of the 13 subjects aged 50-59 years, 76.9% were of microseme class; 3.8% were of mesoseme class; 19.2% were of megaseme class. Out of the 13 subjects aged 60-69 years, 100% were of microseme class; 0% were of mesoseme class; 0% were of megaseme class. Out of the 7 subjects aged 70-79 years, 100% were of microseme class; 0% were of mesoseme class; 0% were of megaseme class The frequencies of microsemes were significantly (P < 0.05) higher than non-microsemes in all the age groups in females.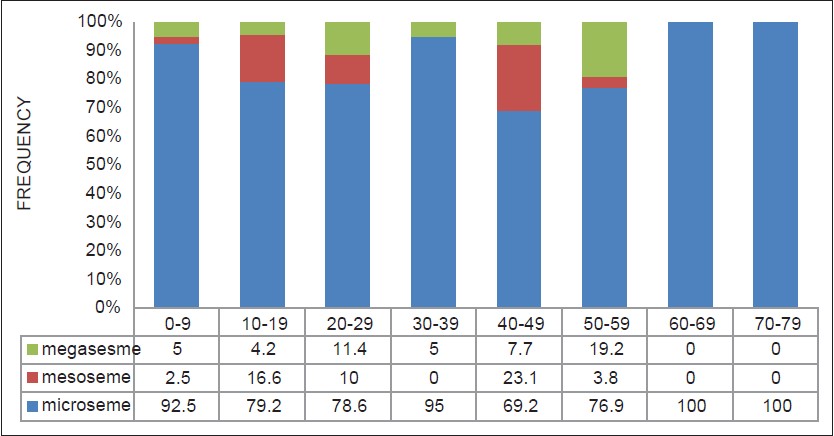 | Figure 5: Bar chart showing frequency of different classes of orbit among different age groups in females
Click here to view |
| Discussion | | |
From the study, the prevalent orbital class among the Igbo Ethnic group is microseme. However, whereas one type of orbital class was found to be predominant, the other orbital classes were also found within the same population. The incidence of microseme was higher in females than in males. This agreed with Patnaik et al.,[7] that microseme was the typical orbital class of the black race. It however was at variance with an earlier work by Igbigbi and Ebite [9] which showed that adult Malawians were of Megaseme category. This might add some credence to the fact that orbital index varied with ethnicity. Adebisi [8] placed male Hausas/Fulanis in megaseme category and females in microseme category. Igbigbi and Ebite [9] and Adebisi [8] did not, however, state the incidence of the orbital classes in their studies. They classified the orbits based on the mean of the orbital indices.
When gender was combined, the highest incidence of microseme occurred in age group 60-69 years (96%). The highest incidence of mesoseme occurred in age group 40-49 years (16.2%). The highest incidence of megaseme occurred in age group 30-39 years (17.1%). The lowest incidence of microseme occurred in age group 40-49 years (70.3%). There is no incidence of mesoseme in age group 60-69 years. Also there is no incidence of megaseme in age group 70-79 years.
In males, the highest incidence of microseme occurred in age group 10-19 years (93%). The highest incidence of mesoseme occurred in age group 50-59 years (15.6%). The highest incidence of megaseme occurred in age group 30-39 years (22.3%). The lowest incidence of microseme occurred in age group 30-39 years (69.2%). There is no incidence of mesoseme in age group of 60-69 years. Also there is no incidence of megaseme in age group of 70-79 years.
In females, the highest incidence of microseme occurred in age groups 60-69 and 70-79 years (100%). In other words, all the subjects in these age groups are all of microseme category. The highest incidence of mesoseme occurred in age group 40-49 years (23.1%). The highest incidence of megaseme occurred in age group 50-59 years (19.2%). The lowest incidence of microseme occurred in age group 40-49 years (69.2%).
Based on the findings of the study, the study concludes that the predominant orbital class among Igbos was microseme. Whereas an orbital class is usually predominant, other orbital classes are usually found within the same population.
It is recommended that further studies should be carried out in other populations to find out the incidence of different orbital classes instead of concluding that an entire population has a particular orbital class based on the mean.
| References | | |
| 1. | Last RJ. The orbit and paranasal sinuses. In: Eugene Wolff's anatomy of the eye and orbit. In: Lewis HK, editor. 6 th ed. London: WB Saunders and Company; 1968. p. 1-29. 
|
| 2. | Soames RW. Skeletal systems In: Grays anatomy: The anatomical basis of medicine and surgery. In: Williams PL, Bannister LH, Berry MM, Collins P, Dyson M, Dussek J, et al., editor. 38 th ed. London: Churchill Livingstone, Elsevier; 1999. p. 555.
|
| 3. | Ezeuko CV, Aligwekwe AU, Udemezue OO, Ejimofor OC. Orbit dimensions and bony interorbital distance in south-east Nigerians: A radiologic study. J Exp Clin Anat 2007;6:47-50.
|
| 4. | Ferrario VF, Sforza C, Colombo A, Schmitz JH, Serrao G. Morphometry of the orbital region: A soft-tissue study from adolescence to mid-adulthood. Plast Reconstr Surg 2001;108:285-93.
|
| 5. | Bentley RP, Sgouros S, Natarajan K, Dover MS, Hockley AD. Normal changes in orbital volume during childhood. J Neurosurg 2002;96:742-6.
|
| 6. | Denis D, Burguière O, Burillon C. A biometric study of the eye, orbit, and face in 205 normal human fetuses. Invest Ophthalmol Vis Sci 1998;39:2232-8.
|
| 7. | Patnaik VV, Bala S, Singla R. Anatomy of the bony orbits- Some applied aspects. J Anat Soc Ind 2001;50:59-67.
|
| 8. | Adebisi SS. Sex Identification from the skull of the Hausa/Fulani in Northern Nigeria. An Afr Med 2003;2:22-6.
|
| 9. | Igbigbi PS, Ebite LE. Orbital index of adult Malawians. Anil Aggrawal's Internet. J Foren Med Toxicol 2010;11. Available from: http://www.anilagarwal.com/ij/vol_011_no_001/papers/paper001.html [Last accessed on 2013 Dec 03].
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5]
|








 Search Pubmed for
Search Pubmed for