|
 
 |
| CASE REPORT |
|
| Year : 2014 | Volume
: 2
| Issue : 2 | Page : 65-73 |
|
Paramolar complex - The microdental variations: Case series with review of literature
Vela D Desai1, Isha Gaurav2, Sudakshina Das1, MV Sunil Kumar3
1 Department of Oral Medicine and Radiology, Jaipur Dental College, Jaipur, Rajasthan, India
2 Department of Oral Medicine and Radiology, Government Dental College, Jaipur, Rajasthan, India
3 Department of Prosthodontics, Jaipur Dental College, Jaipur, Rajasthan, India
| Date of Web Publication | 23-Mar-2015 |
Correspondence Address:
Vela D Desai
Department of Oral Medicine and Radiology, Jaipur Dental College, B-4O6, Trimurthy Apartment, Opposite BSNL Telecom Colony, Malviya Nagar, Jaipur - 302 017, Rajasthan
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2315-7992.153820

Variations of teeth have always been of enduring interest to clinical practitioners, academicians, and laboratory scientists. Apart from requiring thorough diagnoses and due considerations during treatment planning and procedures, such variations are of great interest to the dental anthropologist in tracing population movements and forensic viewpoints. The present series of case reports describes a rare developmental feature termed "paramolar tubercle," encountered in otherwise normal young adults. Mentioned in the literature in a few case reports, not much is known about this entity. Thus, the purpose of our case report is to increase awareness and stimulate discussion of these structures and their importance. In addition, paramolar tubercles are clinically relevant, as they influence treatment modalities in different dental disciplines and, further, may affect the prognosis of treatment. This case report also includes cone-beam computed tomography (CBCT) imaging taken for one patient to evaluate the utility of such an imaging modality in knowing the precise structure and nature of these anomalies. Keywords: Anthropology, developmental, paramolar tubercle, parastyle, protostylid
How to cite this article:
Desai VD, Gaurav I, Das S, Sunil Kumar M V. Paramolar complex - The microdental variations: Case series with review of literature. Ann Bioanthropol 2014;2:65-73 |
| Introduction | |  |
Human teeth of both dentitions may show variations and changes in morphological structures. No two teeth are alike. The day-to-day variation of teeth that we see is the norm. However, odd, peculiar, or strange groups of teeth are called anomalies. They are the more extreme variations from the norm. Thus, teeth play an important role in any anthropological study due to their preservability, observability, variability, and heritability. Teeth also present geographic variability. [1] Dental anthropologic structures include metric and nonmetric traits. Among these, the nonmetric dental traits (NDTs) are easily observed and documented, and are of value because they possess high taxonomic value and have been used to estimate biological relationships among diverse populations. [2] The dental morphology constitutes distinct features or traits of the crowns and roots that are present or absent and, when present, exhibit variable degrees of expression. Such changes may be found on the crown either in the form of anomalous cusps or as an increased number of roots, which in some instances is associated with an anomalous cusp. The most commonly reported extra/accessory cusps are the cusp of Carabelli, found in the molar, Talon's cusp in the incisor, and Leong's tubercle in the premolar, with frequencies of occurrence varying 1-7.7% for Talon's cusp, 52-68% for the Carabelli cusp, and 8% for Leong's tubercle, respectively. [2],[3]
The case report here presents a unique case series of certain forms of accessory cusps more uncommon than those mentioned before. These microdevelopmental dental morphological alterations may even challenge the prognosis of a treatment. Although the literature suggests that these structures are more common in North Indian populations, [4] so far most of the case reports are from South Indian populations, and only a few case series have been reported. According to the literature reviewed, this case report is the first of its kind to illustrate such a large number of case series among the North Indian population, presenting 15 different cases collected randomly within a period of 6 months from a pool of about 12,657 patients from September 2013 to March 2014, from the Department of Oral Medicine, Diagnosis and Radiology, Jaipur Dental College, Rajasthan.
| Case report | | |
Case 1
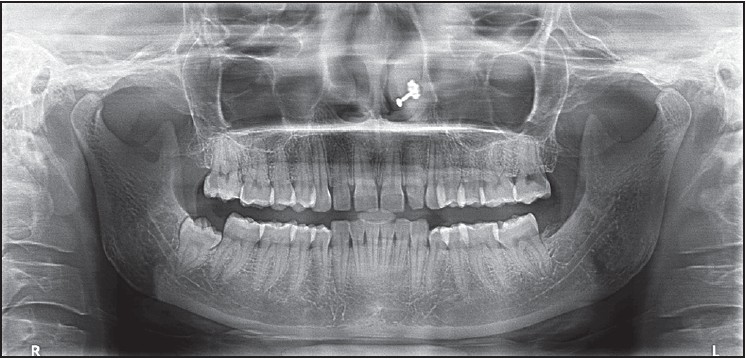
A 22-year-old male patient reported to the outpatient department (OPD) of the Department of Oral Medicine, Diagnosis and Radiology, with the chief complaint of pain in his left upper back teeth for the past 3 months. The patient's familial and medical histories were noncontributory. Extraoral examination revealed no abnormalities. Intraorally, the patient had generalized gingivitis, root stump with 16, bilateral paramolars adjacent to 16 and 26 [Figure 1]a, and caries with 26 and 27. In addition, there was a tubercle seen on the mesiobuccal cusp of 28. The tubercle was cone-shaped, measuring approximately 4 × 3 mm, clearly delineated from the associated tooth by a groove. It had its base at the gingival margin, while the apex was oriented occlusally but well below the occlusal plane. The buccal aspect of the tubercle was smooth, descending straight to the cemento-enamel junction (CEJ). With reference to the available literature, a diagnosis of parastyle was provided for the tubercle. Intraoral periapical (IOPA) radiography of 26, 27, and the paramolar was done for evaluating caries and to visualize the parastyle with 28. IOPA radiography did not provide any information about the extra cusp; thus, cone-beam computed tomography (CBCT) was done in order to understand the exact nature of this structure after obtaining written consent from the patient [Figure 1]b and c. CBCT showed a pulp horn extending into the parastyle, with the parastyle merging with the rest of the tooth in the cervical area. There was no root structure present.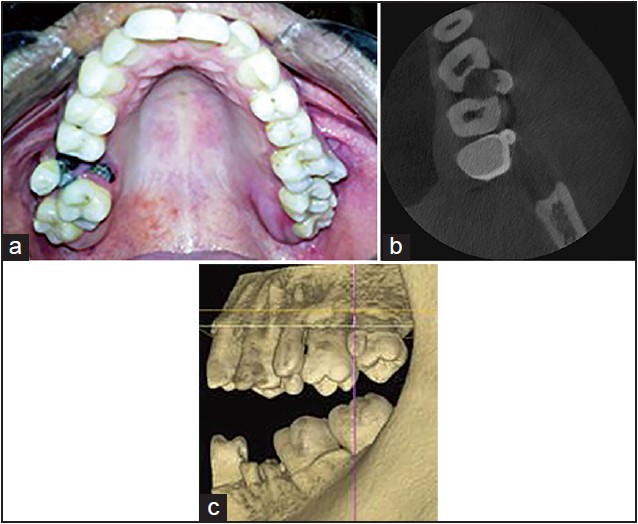 | Figure 1: (a) Bilateral paramolar with respect to 16, 26 (b) CBCT image showing the tubercle on mesiobuccal cusp of 28 (c) CBCT image showing no root structure with respect to the tubercle
Click here to view |
Case 2
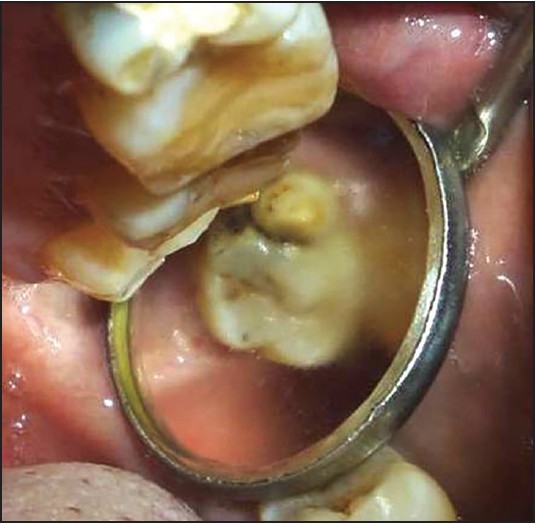
A 20-year-old male patient visited the OPD with the chief complaint of dirty teeth for the past 6 months. His family and medical histories were noncontributory, and extraoral examination revealed no abnormality. On intraoral examination, no soft-tissue abnormalities were observed except gingivitis with mild stains. There was caries with 26, 36, and 37; Missing 18, 28, 38, 47 and 48. Extra cusps could be seen bilaterally on the mesiobuccal cusps of 17 and 27 [Figure 2]. They measured approximately 3 × 3 mm. Each extra cusp was separated from the associated tooth by a groove and was out of occlusion. These structures were given the name "parastyle." Study casts were made to accurately measure the dimensions of the cusps. Radiography revealed a radiopaque V-shaped extension of the cusp up to the CEJ. | Figure 2: Additional cusp on 17 separated from the tooth by a straight groove
Click here to view |
Case 3
A 21-year-old male patient visited the Department for a routine dental checkup with noncontributory family and medical histories. No abnormality was detected on extraoral examination. Upon intraoral examination, a parastyle was found present on the buccal surface of the maxillary right second molar. The free cusp apex did not reach the occlusal plane and thus was out of function. On the buccal view, it constituted a conical shape, which measured about 5 mm cervicoocclusally and 3 mm mesiodistally. The triangular prominence had its base at the gingival margin and its apex oriented occlusally.
Case 4
A 29-year-old female patient visited the Department of Oral Medicine, Diagnosis and Radiology with a complaint of bleeding gums in the lower anterior region for the past 3 months. Family and medical histories were noncontributory, with no extraoral abnormalities. Clinically, intraoral examination revealed no soft-tissue changes except moderate gingivitis. A parastyle was present on the buccal surface of the maxillary right second molar. It had a slightly bluish hue, unlike the rest of the tooth. The buccal view showed a conical structure measuring about 5 mm cervicoocclusally and 3 mm mesiodistally that had its apex well above the occlusal plane.
Case 5
A 28-year-old female patient visited the dental OPD complaining of bleeding gums in the lower anterior region for the past 5-6 months. Family and medical histories were noncontributory. Extraoral examination revealed no abnormalities. Intraoral examination revealed no soft-tissue abnormalities except mild gingivitis with the presence of a moderate degree of stains and calculus. A parastyle was present on the mesiobuccal surface of the maxillary right second molar. It was conical, measuring about 5 mm cervicoocclusally and 5 mm mesiodistally, slightly above the occlusal plane. Radiography revealed a V-shaped radio opacity on the mesiobuccal cusp of second molar also with a fully formed root [Figure 3].
Case 6
A 17-year-old boy had the complaint of proclination of anterior teeth and hence wanted orthodontic treatment. No relevant medical and dental histories were presented. Intraoral examination revealed Angle's class 1 molar relationship. The maxillary right second permanent molar (17) had a parastyle on the mesiobuccal cusp measuring about 4.5 mm cervicoocclusally and 4 mm mesiodistally. Radiography revealed pulp stones in the pulp chamber of 17.
Case 7
A 30-year-old female patient visited the dental OPD with a complaint of decayed tooth in the upper right back teeth region. There were no relevant medical or dental histories. Clinical examination revealed gross caries leading to a chronic periapical abscess with respect to 24, and generalized gingivitis. The maxillary left third permanent molar (28) had a bulky parastyle present on the mesiobuccal cusp measuring about 4.5 mm cervicoocclusally and 5 mm mesiodistally, extending almost up to the occlusal plane [Figure 4]. There was a prominent groove evident between the extra cusp and the rest of the tooth. Fissure caries could be appreciated in the tooth, with discoloration of the adjacent tooth. Radiography of the region confirmed a parastyle, with dental caries developed in relation to the groove.
Case 8
A 26-year-old female patient reported to the Department of Oral Medicine, Diagnosis and Radiology with the chief complaint of pain in the lower right back teeth for the past 5 days. Medical, dental, and family histories were noncontributory. A parastyle present on the mesiobuccal cusp of 17 had its base at the CEJ and its apex approximately 2 mm above the occlusal plane. Radiography revealed a V-shaped radiopacity superimposed on the mesiobuccal cusp of the maxillary second molar.
Case 9
A 48-year-old male visited the dental OPD with the chief complaint of pain in a left lower back tooth for the past 1 year, with no relevant medical and family histories, and there was no abnormality found with extraoral examination. Intraorally, there was generalized attrition and periodontitis with restoration done in 37. An extra cusp was appreciable in 28, not in occlusal contact. A radiopacity merging at the cervical region was seen in the radiograph.
Case 10
A 25-year-old male patient reported to the Department of Oral Medicine, Diagnosis and Radiology with the chief complaint of dirty teeth and bleeding gums for the past 6 months. The patient's familial and medical histories were noncontributory. On clinical examination, there was gingivitis with a moderate amount of plaque and calculus.
A triangular cusplike projection was seen on the mesiobuccal aspect of 38, measuring approximately about 3 × 4 mm size, with color similar to the associated tooth, projecting from the cervical line toward the occlusal surface (2 mm below the occlusal surface). According to the explanation given by Dahlberg, a diagnosis of protostylid was given for the extra cusp. Radiovisiography (RVG) revealed the same with curved mesial roots.
Case 11
A 36-year-old male complaining of sensitivity to hot and cold fluids for the past 5-6 months visited the dental OPD. He had noncontributory medical and family histories. Extraoral examination revealed no abnormalities; there was generalized attrition intraorally. The occlusion view of the teeth presented an extra cusp over the distolingual surface of the mandibular right third molar. It constituted a triangular shape that measured about 5 mm cervicoocclusally and 6 mm mesiodistally. The prominence was also evident on IOPA radiography, with its base well below the gingival margin and its apex oriented distoocclusally, extending almost up to the occlusal plane. A diagnosis of protostylid was given for the extra cusp. RVG of the same showed radiopacity of the extra cusp overlapping the distal aspect of the crown, with an extension on the distal root inferiorly presenting as having a rudimentary root [Figure 5].
Case 12
A 36-year-old male patient came with the complaint of bleeding gums for the past 5-6 months and sensitivity to hot and cold fluids in the lower left back teeth region since 4-5 months. There was history of trauma to the maxillary anterior teeth 3-4 years ago and insignificant medical and family histories. This patient had a deleterious oral habit of bidi smoking one packet per day for the past 10-12 years. No abnormality was detected on extraoral examination; generalized periodontitis was found present on intraoral examination. A protostylid showed on the buccal surface of the mandibular right second molar at the cervical one-third of the crown, having a conical shape. It measured about 4 mm cervicoocclusally and 3 mm mesiodistally, and was 7 mm below the occlusal plane. The same was also evident as a triangular radiopacity on the IOPA radiograph. The extra cusp contributed to periodontal destruction in this case and had to be extracted with the patient's consent. During extraction, the cusp was separated from the tooth, as shown in the figure, which comprised enamel, dentin, and pulp, and had a rudimentary root [Figure 6]a and b.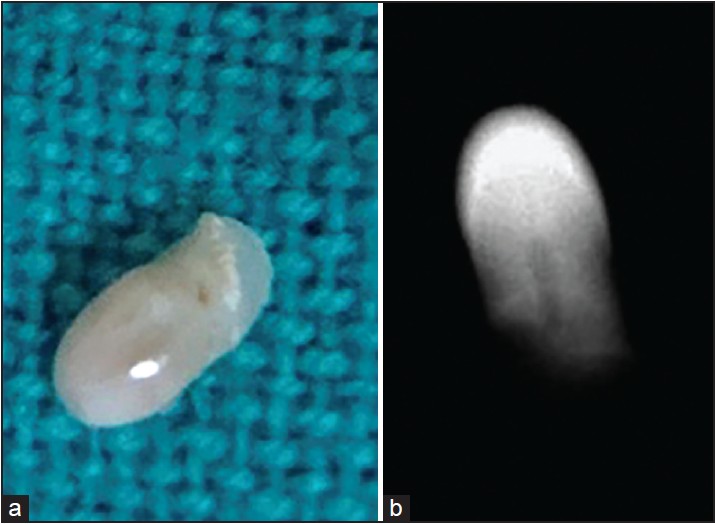 | Figure 6: (a) Specimen of protostylid on 48 after extraction of the tooth (b) Radiograph of specimen of protostylid on 48
Click here to view |
Case 13
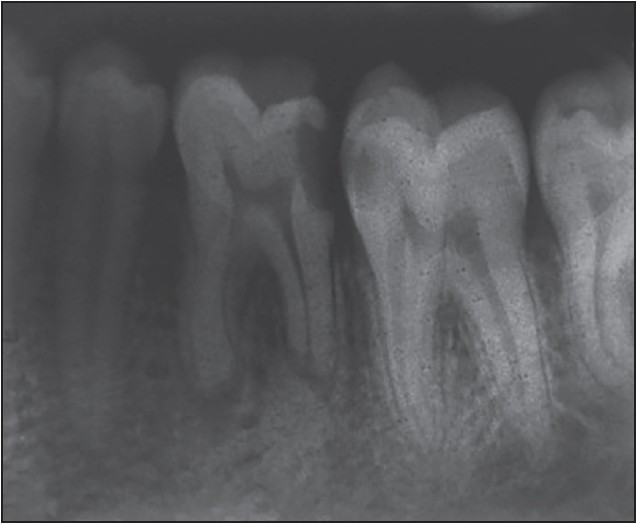
A 35-year-old male patient arrived with the complaint of pain in the left lower back teeth region for the past 4-5 months. Family and dental histories were noncontributory. An extraoral examination revealed no abnormalities. Upon intraoral examination frictional keratosis was found on the left buccal mucosa, attrition of the posterior teeth, a moderate amount of plaque and calculus, carious exposure with 36, caries with 37, and pericoronitis with 38. A protostylid was present on the mesiobuccal surface of the left mandibular second molar. On the buccal view, the protostylid showed a rounded appearance, with slight attrition extending from the CEJ up to the occlusal surface, measuring approximately 7 mm mesiodistally and 4 mm cervicoocclusally. IOPA radiography revealed periapical pathology with 36 and caries in 37. The protostylid was seen as a discrete radiopacity that had a completely formed root structure [Figure 7].
Case 14
A 21-year-old female patient visited the OPD of the Department of Oral Medicine, Diagnosis and Radiology with the chief complaint of pain in the right and left posterior teeth, which were revealed to have pericoronitis. Medical, dental, and family histories were noncontributory. The patient presented with a small cusplike projection on the mesiobuccal cusp of the lower right second molar, the base of which was at the CEJ, the cusp extending to half of the crowns length. Radiography revealed only a faint shadow of the cusp on the crown.
Case 15
A 42-year-old male patient with a complaint of pain in his right lower back teeth visited the dental OPD. The general medical and family histories were insignificant, and there was a history of dental treatment in the same tooth. The patient had the deleterious oral habit of cigarette smoking for the past 20 years. Intraorally, there was a white patch on the left buccal mucosa (provisionally diagnosed as leukoplakia), the teeth showed generalized attrition, and 46 was cariously exposed and tender on percussion. A protostylid was present on the mesiobuccal cusp of 47. Due to attrition, there were no cuspal elevations on 47, thus the protostylid had its apex reaching the occlusal plane. IOPA showed periapical radiolucency with a partially filled distal canal in 46, and radiopacity of the protostylid with a well-developed root.
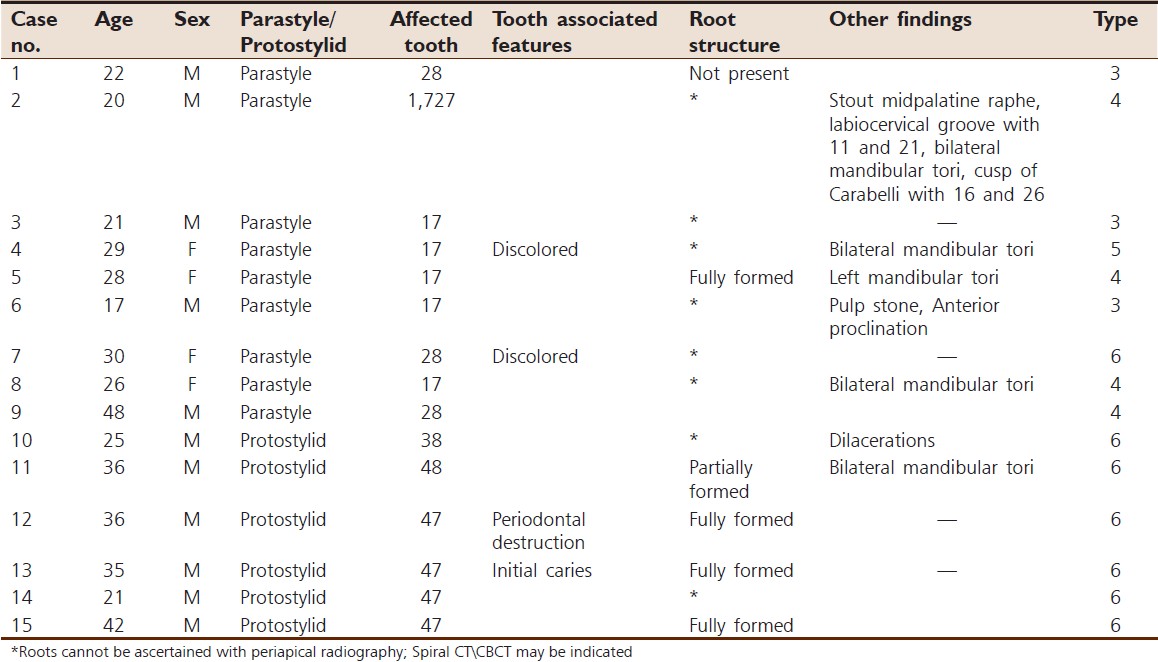
For all the above cases, [Table 1] preventive measures such as oral prophylaxis with instructions for good oral hygiene practice measures and healthy diet were advised. The use of topical fluoride gel was instituted. Other treatments were rendered to the patients as necessitated and kept under follow-up. The presence of caries (case 13), discoloration between the teeth and the extra cusp (cases 4 and 7), and periodontal problems (case 12) mandate the recognition of these structures and their associated problems to enable early intervention and careful follow-up in the future.
| Discussion | | |
The two most prevalent uses of teeth are for studies in phylogeny and ecological adaptation. Teeth are a good and durable source of characteristics for phylogenetic analysis, including the following: The surface features of tooth crowns, most notably cusps and crests; structural details of enamel; and measures of size and shape. These characteristics are discrete and heritable, and show different degrees of expression, that is, different characteristic states. [5]
Dental size and morphology are easily-recorded aspects of phenotypic variations among these characteristics, either by examination of the negative relief in a wax bite impression or by making an alginate impression and plaster cast. [6]
The primary units of teeth that constitute the crowns are called cusps, whereas those of the roots are cones. The majority of pathological variations in shape affect the crown of the tooth, one of which may be in the form of an extra cusp. Among these, the entity that is of interest to the authors is the "paramolar tubercle." A paramolar tubercle is an additional cusp occurring on the buccal surface of a permanent molar. [4],[7]
The term "paramolar tubercle" was first described in the literature by the late Prof. Bolk in 1916. [7] It is defined as any stylar or anomalous cusp, supernumerary inclusion, or eminence occurring on the buccal surfaces of both upper and lower premolars and molars. [7]
The paleontological nomenclature given by Dahlberg in 1945 refers to this structure as the "parastyle" when present in the upper molars and as the "protostylid" when present in the lower molars. [8]
Paramolar tubercles are considered NDTs, which are structural characteristics expressed within certain biological and geographical affiliations. Racial and ethnic background plays an important role in its occurrence. These structures can be considered normal morphological features of the dentition and are not classified as anomalous structures because of their low occurrence; very little information about these structures is cited. The occurrence of paramolar tubercles is reported with varied prevalence in different parts of the world. According to the study by Kustaloghi et al., the occurrence of parastyles is prevalent among Indians. [3],[4],[9]
Clinically, these anomalies present with diverse sizes and shapes, from a mere prominence of the buccal surface to a well-developed lobulated cusp having the appearance of a fused supernumerary tooth. The lobulated tubercle is often associated with a root that is either rudimentary or fully formed, as in a few of the cases presented by the authors. Paramolar tubercles, when present in maxillary molars, tend to unite at the roots, whereas those in the mandibular molars have their own roots, as reported by Bolk. [7],[9],[10]
Parastyle
The prevalence rate of the parastyle is very low in upper first molars (0-0.1%) compared with upper second molars (0.4-2.8%) or with upper third molars (0-4.7%), as quoted in the literature. [4],[7],[11] In the present series, out of nine cases of parastyle, six cases were found on the second molar and three on the third molar.
Clinically, a parastyle may present with varying degrees of expression. The clinical presentation of the parastyle according to plaque [developed by Joseph F Katich and Turner (1974)] [12] is shown in [Table 2].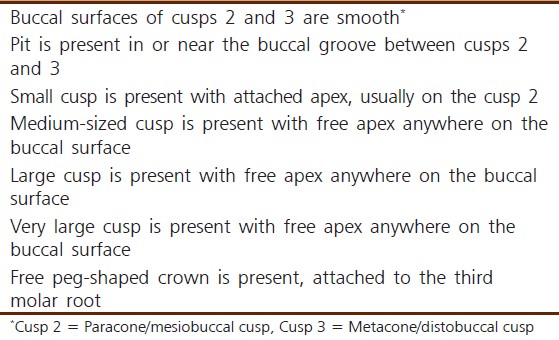 | Table 2: A scale for determination of the degree and expression of parastyle-by Plaque
Click here to view |
The cases discussed by the authors showed varying degrees of expression, ranging 3-6. Sex predilection has not been mentioned previously in the literature, and the authors of this study also did not find any significant difference regarding sex between the five male patients and the four female patients. Eight of the nine patients were in their second and third decades of life, with one in the fourth decade. The prevalence as seen in our series was on the right side, with five cases on the right side, three on the left side, and one bilateral. However, a prevalence study is mandatory in this area.
Protostylid
The Arizona State University Dental Anthropology System (ASUDAS), which was devised for the analysis of modern human teeth, defines the protostylid as a paramolar cusp found on the buccal surface of the protoconid that is normally associated with the buccal groove. [12]
A protostylid was described by Dahlberg (1950) as "an elevation or ridge of enamel on the anterior part of the buccal surface of the lower molars, which ascends from the gingival end of the buccal groove and extends mesio-occlusally." [9]
The protostylid may be seen on both primary and permanent molars but more frequently in primary than in permanent. In the primary dentition, the protostylid is found on the buccal surface of the protoconid of the mandibular second molar. Whenever a protostylid is found on a permanent molar, it has been reportedly present on the primary second molar; however, the reverse situation does not always occur. [4],[8],[13]
The clinical presentation of the protostylid has been classified by Hanihara [14] into six types as described in [Table 3].
The classification of protostylids holds good only for the primary dentition and not for the permanent dentition. In our case series, all cases noted were on permanent teeth, so the exact types of protostylid could not be ascertained. However, if we classify our cases using the same classification, all of them belong to type 6.
Out of the six cases of protostylid presented, four were present on the second molar and two on the third molars, while three showed a distinct root formation that has not been reported previously. All the patients were males in their second, third, and fourth decades of life. Five cases had their protostylids on the right side, whereas in only one was it present on the left side.
Etiologic considerations
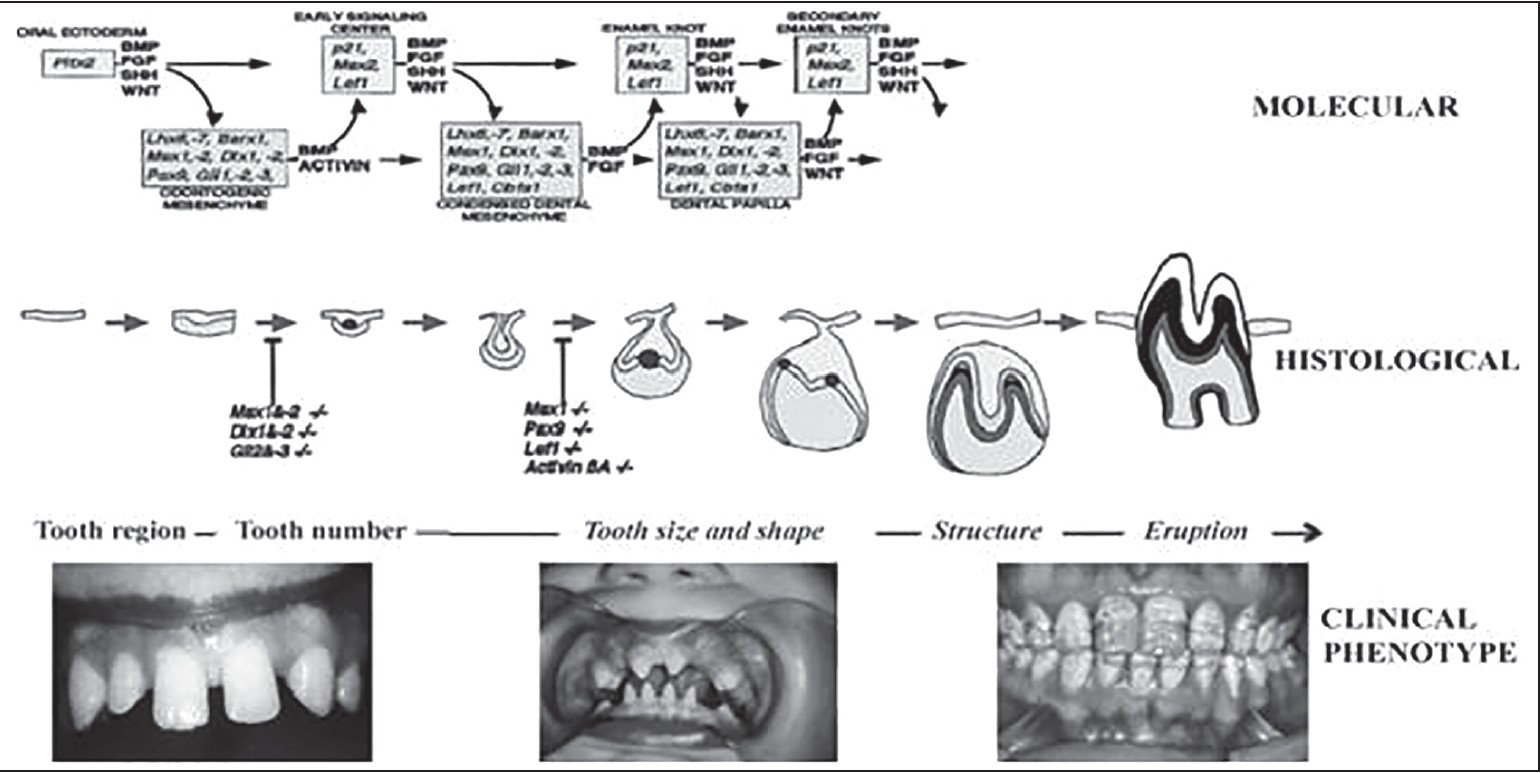
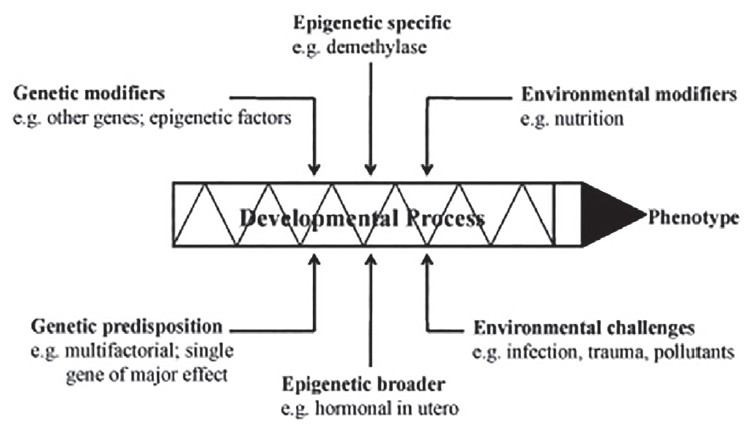
Before understanding the variations in any process, it is necessary to understand the development of the same. Dental anomalies are the result of the complex interactions among genetic, epigenetic, and environmental factors that occur during the process of tooth development. [15],[16] The entire process is multifactorial, multilevel, multidimensional, and progressive over time, as shown in [Figure 8] and [Figure 9].
The shape of the tooth crown is the result of morphogenesis during the cap and bell stages, when there is rapid proliferation of cells related to the folding of the epithelium to form cusp shapes. As the process of tooth morphogenesis advances, the primary and secondary enamel knots control the development of crown dimensions and cusp formation. The tumor necrosis factor (TNF) signaling pathway is an important regulator of tooth germ epithelial morphogenesis, which establishes tooth shape and especially the typical cusp/depression pattern of the molar crown. [17]
The repeated activation and inhibition of signaling is related to differential growth and folding within the tooth germ, and this determines the dimensions and cusp pattern. Apoptosis has been suggested as the probable mechanism controlling the duration of signaling in the enamel knots. The macroscopic morphology shows major differences after the inhibition of apoptosis. Thus, apoptosis in the enamel knot plays an important role in regulating tooth size and shape. [18],[19]
After the process of apoptosis at the late cap stage, the primary enamel knot no longer exists at the bell stage. Secondary enamel knots develop at the sites of the cusps in teeth with multiple cusps. They produce signaling molecules stimulating the proliferation of nearby cells, leading to folding of the inner enamel epithelium and resulting in cusp formation at this stage. Here the presence or absence, and the size and shape of the individual tooth are determined. [16],[17],[18]
Turner and Harris have suggested that in the case of a molar tubercle, cusps arise during the morphogenesis process, starting from an accessory enamel knot developed at the surface where the future apex forms. These tubercles do not provide any functional adaptation such as enlarging the occlusal (masticatory) surface because these tubercles do not enter into function, not occluding against any cusp or groove of the antagonist tooth. [3] The Pax and Msx genes are responsible for the abnormal shape of the teeth. [20]
Clinical implications
These suprastructures attach to the tooth, forming deep grooves that are sites vulnerable to plaque accumulation. As oral hygiene maintenance is difficult in these areas, the tooth becomes prone to dental caries, gingivitis, or localized periodontitis, as was seen in many of our cases. As a result, difficulties in orthodontic banding, root canal treatment, and extractions may be faced by the dentist.
When these structures present problems for the patient, such as dental caries or discolored teeth, an early and definitive treatment in line with the general principles of caries management has to be undertaken. Keen observation also suggests that if the tubercle rises slightly below the CEJ, it may result in periodontal breakdown, as it did in case 12. Thus, early diagnosis could prevent the unnecessary loss of teeth, as in one of our cases, where the patient opted for extraction.
Radiography
IOPA radiography shows the presence of these tubercles, but the exact morphology and anatomy of these structures have to be configured if treatment has to involve the concerned tooth. A problem arises in cases of endodontic therapy, where the relationship between the pulp of the tubercle and that of the associated tooth must be ascertained. RVG or IOPA radiography, being two-dimensional (2D) views of three-dimensional (3D) structures, do not give a clear picture of the internal anatomy of paramolar tubercles. IOPA radiography only shows a radiopacity overlapping the normal tooth structure, with not much of the overall structure of the extra cusp discernible-the level of attachment, the pulp chamber, or the pulp canal in cases where a root structure is also present. Additionally, if present, it remains to be studied whether a separate canal is present throughout or merges with the main canal. Thus, for all these queries, a 3D imaging modality would be a better option.
In the present case series, CBCT imaging of one of the teeth was done to learn about the usefulness of such a modality in delineating the structure of paramolar tubercles. This was done after obtaining consent from the patients, but it could not be advised for all the patients, for ethical reasons.
The authors opine that CBCT would be a better tool if the treatment required involvement of the concerned tooth, as the dose of radiation, though higher than in IOPA radiography, is much lower than in other 3D imaging modalities (such as spiral CT) suggested previously.
Unlike in traditional 2D radiography, which has the same inherent limitations of magnification and minification of structures, superimposition of anatomical and/or pathological entities, and misrepresentation of structures, in CBCT structural superimposition and image enlargement and distortion does not occur, thus allowing a precise 3D visualization of dental and maxillofacial structures. CBCT involves much lower radiation exposure, which ranges 29-577 uSV, compared to a conventional CT scanner with its radiation exposure of approximately 2000 uSV. [21],[22],[23] Moreover, concentrating the radiation at the area of interest, that is, the posterior teeth of a particular quadrant, can further limit the radiation dose.
Future perspectives
Case reports of this kind can increase awareness among dental practitioners about such rare entities and help in their identification and proper management. Certain preventive therapies can be done, such as placing pit and fissure sealants on the concerned tooth to prevent future damage. There is limited information about any relationship of racial differences with frequencies of paramolar tubercles because of their apparently low overall occurrence. [2] The reporting of such cases can help us learn the percentage of their occurrence in different populations or geographic areas, and aid in forensic investigation.
Another interesting thing observed while compiling the cases was that five out of 15 cases had mandibular tori as an additional finding along with an extra cusp. Whether this finding was purely incidental or points to any association between the two entities needs to be studied.
There exists a controversy regarding whether the tubercles having roots should be considered extra cusps or should be categorized as a fusion of a supernumerary tooth with a primary/permanent tooth. Thus, an in-depth study is required in this area.
In addition, studies need to be done to understand the significance of such extra cusps in modern human teeth- whether they have newly appeared in evolution or are remnants from earlier stages of evolution. Further, in-depth genetic analysis should be considered.
| Conclusion | | |
As oral physicians, we should be aware of these kinds of morphological variations observed during routine dental examinations and not be very dogmatic about the standard morphological features of teeth. Proper documentation of these variations may help anthropologists in their study of a population. However, before any valid data can be gathered, the diagnostic features and classifications of these dental traits need to be determined so as to ensure the accurate and consistent recording of data and, further, to permit appropriate comparisons between investigators.
| References | | |
| 1. | Katzenberg MA, Saunders SR. Dental morphology. In: Katzenberg MA, Saunders SR, Scott RG, editors. Biological Anthropology of the Human Skeleton. 2 nd ed. Hoboken, NJ: John Wiley & Sons; 2008. p. 265.  |
| 2. | Scott GR, Turner CG 2nd. Description and classification of permanent crown and root traits. In: Scott GR, Turner CG 2nd, editors. The Anthropology of Modern Human Teeth-Dental Morphology and its Variation in Recent Human Populations. 1st ed. Cambridge: Cambridge University Press; 1997. p. 15-69. |
| 3. | Carolina R, Freddy M. Paramolar tubercle in the left maxillary second premolar: A case report. Dental Anthropol 2006;19:65-9. |
| 4. | Kustaloglu OA. Paramolar structures of the upper dentition. J Dent Res 1962; 41:75-83. |
| 5. | Jernvall J, Jung HS. Genotype, phenotype, and developmental biology of molar tooth characters. Am J Phys Anthropol 2000;(Suppl 31):171-90. |
| 6. | Djuric-srejic M, Radonjic V, Nikolic V, Markovic M. Anthropological analysis of dental remains of two Medieval Serbian populations. Variability and Evolution 1997; 6:73-9. |
| 7. | Bolk L. Problems of human dentition. Am J Anat 1916;19:91-148. |
| 8. | Dahlberg AA. The paramolar tubercle (Bolk). Am J Phys Anthropol 1945;3:97-103. |
| 9. | Dahlberg AA. The evolutionary significance of the protostylid. Am J Phys Anthropol 1950;8:15-25. |
| 10. | Magalee RE, Kramer S. The Paramolar tubercle: A morphological anomaly with clinical considerations. N Y State Dent J 1984;50: 564, 566. |
| 11. | Chao-Mao M. Statistical observation of morphological and numerical anomalies in the teeth of Japanese. Shikagaku Zasshi 1949;6:248-56. |
| 12. | Turner CG, Regan M, Irish J. Physical Anthropology Analysis, Roosevet Platform Mould Study: A Laboratory Plan for Salado Research. Archaeological Research Institute - Arizone State University. Available from: http://archaelogy.asu.edu/library/lab/chapter_ninepdf. [Last accessed on 2011 Apr 18]. |
| 13. | Skinner MM, Wood BA, Hublin JJ. Protostylid expression at the enamel-dentine junction and enamel surface of mandibular molars of paranthropus robustus and Australopithecus Africanus. J Hum Evol 2009;56:76-85. |
| 14. | Hanihara K. Criteria for classification of crown characters of the human deciduous dentition. Zinriugaku Zassi 1961;69:27-45. |
| 15. | King NM, Tongkoom S, Wong HM. Morphological and numerical characteristics of the southern chinese dentitions. Part IV: Traits in the primary dentition. Open Anthropol J 2010;3:37-53. |
| 16. | Brook AH. Multilevel complex interactions between genetic, epigenetic and environmental factors in the aetiology of anomalies of dental development. Arch Oral Biol 2009;54(Suppl 1): S3-17. |
| 17. | Thesleff I, Keränen S, Jernvall J. Enamel Knots as signaling centers linking tooth morphogenesis and odontoblast differentiation. Adv Dent Res 2001;15:14-8. |
| 18. | Thesleff I. Developmenttal biology and building a tooth. Quintessence Int 2003;34:613-20. |
| 19. | Tummers M, Thesleff I. The importance of signal pathway modulation in all aspects of tooth development. J Exp Zool B Mol Dev Evol 2009;312B:309-19. |
| 20. | Turner RA, Harris EF. Maxillary second premolars with paramolar tubercles. Dent Anthropol 2004;17:75-8. |
| 21. | Kerebel B, Dard M, Le Cabellec MT, Kerebel LM. Dental enamel pearls: Histopathological study. J Biol Buccale 1986;14:239-48. |
| 22. | Nirmala SV, Challa R, Velpula L, Nuvvula S. Unusual occurrence of accessory central cusp in the maxillary second primary molar. Contemp Clin Dent 2011;2:127-30. [ PUBMED]  |
| 23. | Nayak G, Shetty S, Singh I. Paramolar tubercle: A diversity in canal configuration identified with the aid of spiral computed tomography. Eur J Dent 2013;7:139-44. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7], [Figure 8], [Figure 9]
[Table 1], [Table 2], [Table 3]
|









 Search Pubmed for
Search Pubmed for