|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2014 | Volume
: 2
| Issue : 1 | Page : 23-27 |
|
Theoretical versus practical application of prosthodontic techniques in private dental clinics in India: A survey
Gurminder Singh1, Ramandeep Singh Gambhir2, Rina Singh1, Harpreet Kaur3
1 Department of Prosthodontic, Gian Sagar Dental College and Hospital, Rajpura, Punjab, India
2 Department of Public Health Dentistry, Gian Sagar Dental College and Hospital, Rajpura, Punjab, India
3 General Dentistry Department, Private Practitioner, Chandigarh, India
| Date of Web Publication | 12-Dec-2013 |
Correspondence Address:
Ramandeep Singh Gambhir
Department of Public Health Dentistry, Gian Sagar Dental College, Rajpura - 140 601, Punjab
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2347-4610.122990

Objectives: To know the various prosthodontic techniques followed by the private dental practitioners as compared withthe techniques taught to them in the dental schools. Materials and Methods: A survey was done to determine the prosthodontic techniques by private practitioners in India. A pretested questionnaire performa containing questions on complete denture, removable partial denture, and fixed partial denture fabrication was prepared for the private practitioners to be filled up. A total of 700 subjects were included in the final study (70% response rate). Results: A total of 80.4% of the practitioners used to do the whole prosthetic treatment themselves. A total of 61.7% used to make study casts before the treatment. And, 85% of the practitioners preferred to make complete dentures using double impression technique. Most practitioners faced problems during fabrication of complete dentures, removable partial denture, and fixed partial prosthesis. Conclusion: The findings from this study showed that the respondents did not follow the techniques and procedures which were being taught in the dental schools which had been deemed to be clinically essential for the successful prosthodontic treatment and there was a need for continuing dental education programs for the private practitioners for upgradation of their clinical skills. Keywords: Dental school, private practitioners, prosthodontic, techniques
How to cite this article:
Singh G, Gambhir RS, Singh R, Kaur H. Theoretical versus practical application of prosthodontic techniques in private dental clinics in India: A survey. Eur J Prosthodont 2014;2:23-7 |
How to cite this URL:
Singh G, Gambhir RS, Singh R, Kaur H. Theoretical versus practical application of prosthodontic techniques in private dental clinics in India: A survey. Eur J Prosthodont [serial online] 2014 [cited 2018 Jul 5];2:23-7. Available from: http://www.eurjprosthodont.org/text.asp?2014/2/1/23/122990 |
| Introduction | |  |
Prosthodontics is defined as the branch of dentistry pertaining to the restoration and maintenance of oral function, comfort, appearance, and health of the patient by the restoration of the natural teeth and/or replacement of missing teeth with artificial substitutes. [1] It is a branch of dentistry pertaining to the oral rehabilitation of the patient by the practitioner who provides complete dentures, removable partial dentures, fixed partial dentures, and maxillofacial prosthesis. Also, the practitioner must be aware of the biocompatibility and bioacceptability of the prosthesis and techniques which are being used for the patient.
It is wisely said that "It is more important to preserve what already exists than to replace what is missing." [2] This statement indicates that the prosthesis which the practitioner fabricates should not only replace the missing structures but also preserve what is existing. There are various authors and textbooks describing these techniques which guide the operator and help in providing optimal care and they may have different opinion regarding each technique. In other words, each dental school and teacher has a unique philosophy of imparting education to the patient. However well these techniques are taught or learned they are sometimes not carried out as they should be. Various studies have reported about the following of prosthodontic procedures by private dental practitioners and techniques taught in dental institutions. [3],[4],[5],[6],[7] A survey reported that there is a difference in procedures followed for complete denture construction in dental schools as compared with general dental practice. [7] For this survey the standardized syllabus prescribed by the Dental Council of India (DCI) is taken as the benchmark and we have accepted that all the dental graduates are fully acquainted with the ideal prosthodontic procedures as they have passed from recognized dental colleges. [8]
This study was undertaken to know the various prosthodontic techniques followed by the private dental practitioners, to know the problems encountered by the private dental practitioners in various prosthodontic treatments, and to compare the techniques taught and techniques followed by them.
| Materials and Methods | | |
A survey was planned to determine the prosthodontic techniques applied by private dental practitioners of India and to know the problems faced by the practitioners during the various phases of the complete dentures, removable partial denture and fixed partial denture treatments, and to compare the techniques taught to them and techniques followed by the practitioners.
Survey performa
To conduct the survey, a pretested questionnaire performa was prepared for the private dental practitioners to be filled up. The performa contained questions relating to complete denture, fixed partial denture, and removable partial denture treatment. There is no standardized version of the performa, but it was specially designed in the department of prosthodontics for the present survey. This questionnaire performa was tested on 50 private dental practitioners.
The removable partial denture treatment was divided into acrylic partial denture and cast partial denture treatments. The complete denture section of the performa contained two diagrams of edentulous maxillary and mandibular basal seat area on which the respondents were asked to draw the following: Area where the spacer is provided, area where vertical tissue stops are provided, and area where perforations are made.
Sample size
A total of 1000 private dental practitioners from fourmajor cities of India (New Delhi, Chandigarh, Bangalore, and Pune) were contacted through personal visits and also through post. The directories of private dental practitioners were obtained from Indian Dental Association branches in the four selected cities. [9] Every 5 th practitioner from the each directory was included in the study by systematic random sampling. Those practitioners who were busy in their practice and could not fill the form on the day of the visit were requested to send the questionnaire through post in a self-addressed envelope. Out of 1000 private dental practitioners, 700 responded to the survey. Nonresponders were not included in the study. Informed consent was obtained from all the private dental practitioners and they were assured that the information collected will be kept confidential.
Statistical analysis
Since it was a simple descriptive study dealing with only numbers and percentages, only Microsoft excel was used to calculate the results and no other statistical software was used. The results are presented in text, tables, and graphical manner.
| Results | | |
Selected results of the survey are useful in describing the current conditions of private prosthodontic practice in various dental clinics situated in major cities of India.
Out of 700, 563 (80.4%) of the private dental practitioners reported that they did the prosthodontic treatment themselves. A total of 70 (10%) had a visiting prosthodontist in their clinics for treating the patients who had prosthetic needs. And 67 (9.6%) private practitioners were doing some of the prosthodontic work themselves and were calling a prosthodontic for complex prosthetic work like cast partial dentures and implant prosthesis.
A total of 670 private practitioners responded to the question of making study casts before the start of the treatment and only 413 (61.7%) made the study casts.
Complete denture fabrication
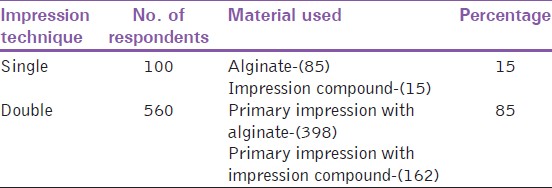
Private practitioners who responded regarding the impression technique followed by them were 660 out of 700. Majority of the practitioners followed double impression technique 560 (85%) as compared with140 (15%) who followed single impression technique [Table 1].
A total of 455 (81.2%) subjects responded to the question of providing spacer in the denture basearea from a total of 560 subjects who practiced double impression technique. Almost half of the respondents (50%) provided the spacer in the mid palatine raphe area, whereas 190 (41.7%) provided the spacer on the ridge crest area and 38 (8.3%) provided on other areas. In the mandibular spacer area, 247 (54.3%) practitioners out of 455 provided the spacer on anterior crest and rest on the premolar and molar area [Figure 1].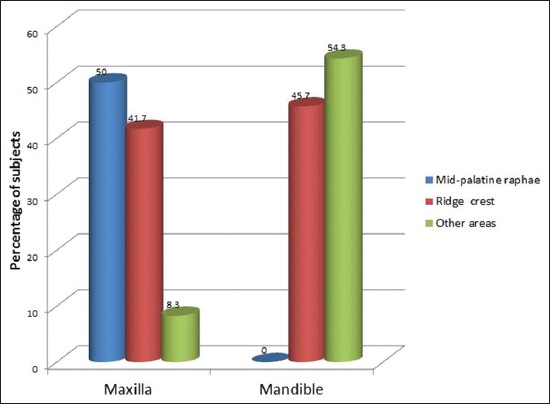 | Figure 1: Place of spacer in the maxillary and mandibular denture base area
Click here to view |
A total of 204 private practitioners responded regarding the provision of vertical tissue stops in the maxillary and mandibular special tray and that too in the premolar and molar area. The perforations in the maxillary special tray in the midpalatine raphe, rugae area, and incisive papilla was the response of 343 (62.2%) practitioners out of total of 560 practitioners. A total of 217 (38.8%) practitioners provided perforation in the ridge crest area. In the mandibular tray, 217 (100%) practitioner made the perforations and all were made in the mandibular ridge crest.
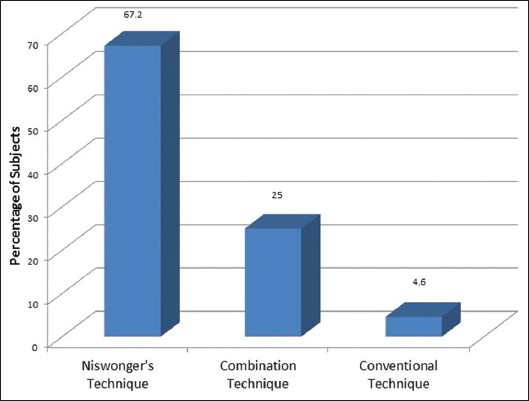
And 660 subjects responded to the question regarding the method used to record vertical jaw relations during fabrication of complete denture. Majority of the practitioners (67.2%) followed Niswonger's technique. Combination and conventional techniques were followed by 25% and 4.6% of the practitioners respectively [Figure 2].
A total of 240 (36.4%) responded regarding the problems encountered in the fabrication of complete dentures. And 104 (43.3%) had problems in jaw relation recording, 30 (12.5%) faced problem in obtaining retention, and 22 (9.2%) reported that it was a time consuming procedure.
Fixed partial denture fabrication
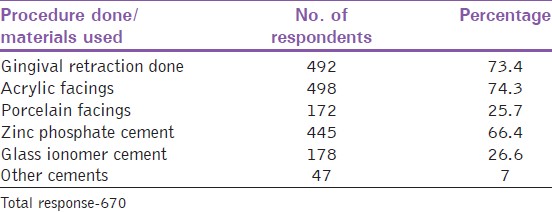
95.8% of the practitioners did the fixed partial denture fabrication. 598 (89.2%) did themselves, whereas 72 (10.8%) had specialist visiting their clinic for fabrication. 492 practitioners out of 670 did gingival retraction before crown preparation. Various types of facings (acrylic and porcelain) were given and different types of crown cementing materials were used by the practitioners [Table 2].
Postcare instructions after fixed prosthesis were given orally by 595 (80.7%) of the practitioners, while 75 (11.2%) gave them in written form. From 310 respondents who faced problems during fabrication of fixed partial prosthesis, 87 (28.2%) faced the problem of sensitivity during tooth preparation, while 86 (27.7%) quoted ''high point'' as the main problem. Facing fracture or detachment was the reply of 20 (6.4%) of practitioners, while 18 (6.5%) felt shade selection as the major problem.
Removable partial denture fabrication
675 practitioners responded to the question regarding the fabrication of removable prosthesis. 480 (71.1%) did only acrylic partial denture fabrication, 10 (1.5%) did exclusive cast partial denture treatment, and 185 (27.4%) did both acrylic partial denture and cast partial denture treatment.
A total of 195 practitioners did the cast partial denture treatment. [Table 3] depicts the various procedures like surveying, metal framework try-in, and postcare instructions given by the practitioners.
115 practitioners responded regarding the problems encountered during the fabrication of cast partial denture. 52 (45.2%) reported poor lab work as the main problem, 33 (28.7%) cited high cost, and 20 (17.4%) reported lack of coordination between the dentist and the laboratory.
| Discussion | | |
The private dental practitioners who did not respond to the questionnaire were contacted for the second time, but none of them agreed to participate in the study therefore the final sample size was 700.
According to DCI syllabus for recognized dental colleges in India, students in their undergraduate level spend more than 30% of their academic career in the development of prosthodontics, staring from the first year to final year learning the various aspects of prosthodontics. [8] Even though theoretically they study prosthodontics in general, clinically they are mainly trained with removable prosthodontics, that is, conventional removable complete dentures and removable acrylic partial dentures.
As already mentioned, literature reveals that there is large difference between theprosthodontic techniques taught in undergraduate curriculum in dental recognized dental institutions and techniques, followed by some of the private practitioners. Different prosthodontic techniques are mentioned by various authors and textbooks an all these techniques are universally accepted. [7],[9]
It has been documented in several studies [10],[11],[12],[13],[14] that to make an accurate impression and to achieve the objective of impression it is necessary to take two impressions (preliminary and final) but in the present study still 15% of the practitioners followed single impression technique. It is also reported in many studies [3],[10] that impression compound in the material of choice for making preliminary impression, but findings of the present study support that 71% of the practitioners used alginate instead of impression compound.
Several studies have suggested the use of adequate spacer over the entire denture bearing area with vertical tissue stops which is contrary with the findings of the study as still 18.8% of the practitioners were not providing spacers. [14],[15],[16] It has been reported by various authors that best way to record the posterior palatal seal area is by the combination of methods but in the present study still 88.2% of the practitioners followed the physiologic method. [17],[18] Moreover, there were many problems quoted by the practitioners during the fabrication of complete dentures. Most of the problems are directly related to the technique applied and expertise of the practitioners as well as sound knowledge in the subject. Lacunae in any one of these will render an unsatisfactory final product by the practitioners.
Tooth sensitivity was one of the problems faced by the practitioners during tooth preparation in fixed partial dentures. Certain patients have very sensitive teeth, and it is difficult to anesthetize them adequately during the treatment. Such teeth are better treated with cements that do not irritate the pulp. While most of the practitioners used zinc phosphate for cementation, resin-modified glass iononer cement andortho-ethoxy benzoic acid cements are good choices for these patients. [19]
It is very essential to fabricate a study cast before the starting with removable partial prosthodontics. [20] The results of the present study reveal that only 13.6% of the practitioners made the study cast which is contrary with the above statement. Lab technicians are inefficient in designing the removable partial denture frameworks, as they lack basic biological knowledge of the oral structures and hence should not be employed to design the removable partial denture framework. [21] But according to the findings of the present study, majority of the dental practitioners (74%) used lab technicians for designing their framework. Similar was the case reported in another study conducted in Alberta. [22]
It is reported that surveying of the diagnostic cast is mandatory for fabricating cast partial denture. [20] But only 30% of the practitioners in the present study were doing the survey. Most of the problems which the practitioners faced during the removable partial denture treatment are related to the callous attitude of the practitioners toward the patient as well as lack of the proper knowledge and expertise for the required treatment.
This survey was conducted in four major cities of India, where most of the modern dentistry is practiced. [9] The survey highlighted the techniques used by the private practitioners in these cities and it can be said from the results that some of the private practitioners in these modern cities still utilize short cut and nonappropriate techniques for prosthodontic rehabilitation of the patients which is the main strength of the survey.
This study has some weaknesses also, and their influence on the accuracy of the results must be acknowledged. For example, it cannot be known with certainty how accurate self-reports of usage are, whether a technique is always or sometimes employed. Also as we have no information regarding the technique followed by nonresponders, this could also influence the outcome of the results to some extent
| Conclusion | | |
The sample of private dental practitioners provides a unique opportunity to determine the various prosthodontic techniques followed by them and to know the problems encountered by them while treating prosthodontic subjects. For the fabrication of an ideal prosthesis, it is required that the practitioners follow the protocol and methods which have been mentioned in standard text books, cited by various authors and taught in the undergraduate curriculum. One possible conclusion is that there is a disconnection between the undergraduate prosthodontic curriculum and the general practice of dentistry. Majority of the private practitioners follow short cut procedures and many of them follow their own convenient method for the treatment of prosthodontic problems. Almost all of them do practice fixed partial denture treatment, even they are not clinically trained. There is a lot of difference between the techniques prescribed and the techniques being followed by the practitioners. The problems encountered by the practitioners during various phases of prosthodontic treatment are avoidable and can be attributed to the lack of knowledge regarding materials and techniques and due to the adoption of various inappropriate methods. One of the problems experienced by the practitioners was sensitivity of teeth during tooth preparation which can be avoided by doing tooth preparation under local anesthesia. Other problem was that of porcelain facing fracture that can be avoided by sticking to the guidelines mentioned in text books for tooth preparation and fabrication of prosthesis and properly imparting post care instructions to the patient. Lack of retention was also one of the problems encountered during fabrication of complete denture and it can be avoided by making the initial impression with appropriate impression material, followed by final impression for capturing the minute details of the soft tissues.
Continuing dental education programs in the field which can highlight the hazards of shortcuts and stress the importance of prescribed techniques can help to improve the practitioners' clinical effectiveness and the quality of the treatment rendered to the patients. It may also be necessary to emphasize strongly the basic prosthodontic principles in the undergraduate teaching curriculum.
| References | | |
| 1. | Blarcom V, Clifford W. The glossary of prosthodontic terms. J Prosthet Dent 1999;81:44-106. 
|
| 2. | Carlsson GE, Omar R. The future of complete dentures in oral rehabilitation. A critical review. J Oral Rehabil 2010;37:143-56.
[PUBMED] |
| 3. | Hyde PT, McCord JF. Survey of prosthodontic impression procedures for complete dentures in general dental practice in the United Kingdom. J Prosthet Dent 1999;81:295-9.
|
| 4. | Petropoulos VC, Rashedi B. Complete denture education in U.S. dental schools. J Prosthodont 2005;14:191-7.
|
| 5. | Rashedi B, Petropoulos VC. Preclinical complete dentures curriculum survey. J Prosthodont 2003;12:37-46.
[PUBMED] |
| 6. | Harrison A, Huggett R, Murphy WM. Complete denture construction in general dental practice: An update of the 1970 survey. Br Dent J 1990;169:159-63.
[PUBMED] |
| 7. | Clark RK, Radford DR, Juszczyk AS. Current trends in complete denture teaching in British dental schools. Br Dent J 2010;208:e10.
[PUBMED] |
| 8. | Kadagad P, Tekian A, Pinto PX, Jirge VL. Restructuring an undergraduate dental curriculum to global standards-a case study in an Indian dental school. Eur J Dent Educ 2012;16:97-101.
[PUBMED] |
| 9. | Wieder M, Faigenblum M, Eder A, Louca C. An investigation of complete denture teaching in the UK: Part 1. A survey of undergraduate teaching. Br Dent J 2013;215:177-81.
[PUBMED] |
| 10. | Bachhav VC, Aras MA. A simple method for fabricating custom sectional impression trays for making definitive impressions in patients with microstomia. Eur J Dent 2012;6:244-7.
|
| 11. | Haney SJ, Nicoll R, Mansueto M. Functional impressions for complete denture fabrication. A modified jump technique. Tex Dent J 2010;127:377-84.
[PUBMED] |
| 12. | Batista AU, Carreiro Ada F, Souza AA, Filho JN, de Almeida EO. Dynamic functional impression technique for severely resorbed alveolar ridges. Eur J Prosthodont Restor Dent 2011;19:160-2.
[PUBMED] |
| 13. | de Souza e Silva ME, de Magalhães CS, Ferreira e Ferreira E. Complete removable prostheses: From expectation to (dis) satisfaction. Gerodontology 2009;26:143-9.
|
| 14. | McCord JF, Grant AA. Impression making. Br Dent J 2000;188:484-92.
[PUBMED] |
| 15. | Futris SC. Prerequisites for trouble-free fully functional dentures. Dent Today 2012;31:116-8.
[PUBMED] |
| 16. | Bindhoo YA, Thirumurthy VR, Kurien A. Complete mucostatic impression: A new attempt. J Prosthodont 2012;21:209-14.
[PUBMED] |
| 17. | Chen MS. Reliability of the fovea palatine for determining the posterior border of the maxillary denture. J Prosthet Dent 1980;43:133-7.
[PUBMED] |
| 18. | Rashedi B, Petropoulos VC. Current concepts for determining the postpalatal seal in complete dentures. J Prosthodont 2003;12:265-70.
[PUBMED] |
| 19. | Hill EE, Lott J. A clinically focused discussion of luting materials. Aust Dent J 2011;56 Suppl 1:67-76.
[PUBMED] |
| 20. | Lechner SK, Thomas GA. Removable partial denture design: Importance of clinical variables. Eur J Prosthodont Restor Dent 1994;2:127-9.
[PUBMED] |
| 21. | Avrampou M, Kamposiora P, Papavasiliou G, Pissiotis A, Katsoulis J, Doukoudakis A. Design of removable partial dentures: Asurvey of dental laboratories in Greece. Int J Prosthodont 2012;25:66-9.
[PUBMED] |
| 22. | Wolfaardt JF, Tan HK, Basker RM. Removable partial denture design in Alberta dental practices. J Can Dent Assoc 1996;62:637-44.
[PUBMED] |
[Figure 1], [Figure 2]
[Table 1], [Table 2], [Table 3]
|









 Search Pubmed for
Search Pubmed for