|
 
 |
| CASE REPORT |
|
| Year : 2014 | Volume
: 2
| Issue : 1 | Page : 37-40 |
|
Magnetically retained extra oral prosthesis and maxillary interim obturator
Shelly Goyal1, Mukesh K Goyal1, Parithimar Kallingan2
1 Department of Prosthodontics and Maxillofacial Prosthetics, Maharaja Ganga Singh Dental College Center, Sri Ganganagar, Rajasthan, India
2 Department of Prosthodontics and Maxillofacial Prosthetics, Sri Ramachandra Dental College and Hospital, Chennai, Tamil Nadu, India
| Date of Web Publication | 12-Dec-2013 |
Correspondence Address:
Mukesh K Goyal
Dental Care, 62-G, Sector-7, Near Living Style Mall, Behind Apollo Hospital, Jasola Vihar, New Delhi - 110 025
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2347-4610.122993

Rehabilitation of patients with acquired defects of the maxilla is a challenge in terms of re-establishing oro-nasal separation. In most patients, these goals are met by means of prosthetic rehabilitation with an obturator prosthesis. Prosthetic rehabilitation can be achieved satisfactorily if all facets of treatment planning and design consideration are taken into account prior to the rehabilitation process. In many cases, effective obturation is achieved, but, in the relative majority, the prosthesis is usually rejected by the patient as being non-retentive and the outcome is a failure. Therefore, making the prosthesis hollow and incorporation of retentive features in effective way can have a dramatic effect on the stability and retention of the obturator prosthesis in partially dentulous maxillectomy patients. This clinical report describes prosthetic rehabilitation of acquired maxillofacial defect with magnetically retained maxillary interim obturator with extra-oral prosthesis. Extra-oral prosthesis was retained with closed-field magnet system. Defect was developed following post-maxillectomy due to olfactory neuroblastoma and surgical obturator. Keywords: Acquired maxillary defect, magnet, obturator, olfactory neuroblastoma, rehabilitation
How to cite this article:
Goyal S, Goyal MK, Kallingan P. Magnetically retained extra oral prosthesis and maxillary interim obturator. Eur J Prosthodont 2014;2:37-40 |
| Introduction | |  |
Defects involving the maxillae, hard palate, and paranasal sinuses present unique surgical and prosthodontic rehabilitation challenges. The etiology may be congenital or developmental (cleft lip and cleft palate) or acquired as a result of inflammatory perforations, traumatic defects, and surgical resections. [1],[2],[3],[4],[5],[6] Patients with maxillary defects commonly experience difficulties in speech, deglutition, and mastication. These patients may also demonstrate a diminished sensation in the resected area, poor lip competency, esthetic and psychological impairment, scar tissue formation, trismus, and xerostomia, especially if the patient receives radiotherapy in addition to surgical resection and tissue crusting in the defect. Treatment modalities for maxillary defect is a combined team approach including surgery, chemotherapy, radiation therapy, speech therapy, diet, nursing, and maxillofacial prosthodontistry. [1] Prosthodontic prognosis is affected by the volume and location of postsurgical bony anatomy, availability of abutment teeth, size of the defect, quality of mucosa, history of therapeutic radiation therapy, the patient's experience with dental prostheses, and neuromuscular control of the patient. After surgical resection of the maxilla, the retention and stability of the surgical obturator are compromised and require more retentive and improved interim prosthesis to restore function and esthetic. The loss of the palatal denture-bearing area and vestibular retentive undercuts leaves an anatomically deficient base to construct the prosthesis. Robinson reported the use of magnetic stabilizers imbedded in a silicone bar suspended above the zygomas to aid in the retention of a complete denture for a hemi-maxillectomy patient. [2] Nadeau used magnets to enhance retention of the permanent obturator and the facial prosthesis. [3],[4] The use of magnets to assist in the retention of an interim maxillary obturator for a large oro-facial defect can markedly improve, both the physical and psychological well-being of the patient during the very critical period of rehabilitation. This report describes the clinical and laboratory management of a patient with Aramany's class IV maxillary defect with magnetically (closed-field) retained interim obturator and extra-oral prosthesis. [6] A successful prosthodontic rehabilitation should recreate the partition between the oral and nasal cavity, restore facial contour, improve mastication and speech intelligibility, provide lip support, improve articulation, and reduce drooling. Aim of this case presentation is to focus on timely rehabilitation of the patient with interim prosthesis to fulfill functional, esthetical, and psychological requirement until definite treatment is planned.
| Clinical Report | | |
A 52-year-old man was referred to the Department of Prosthodontics for the fabrication of a surgical obturator following a hemi-maxillectomy for an olfactory neuroblastoma. Following surgery, the surgical obturator was kept in place for 1 week and post-surgical radiation therapy was planned. The patient developed skin reactions, mucositis, and subcutaneous pheophyphomycotic cyst associated with fungal infection as a complication of post-radiation therapy suggestive of immunodeficiency. The patient also developed extraoral naso-cutaneous fistula communicating with intraoral defect, which was diagnosed as post-operative olfactory neuroblastoma. On examination, the patient presented with generalized weakness and was psychologically depressed due to the development of extra-oral defect. On extraoral examination, the patient revealed right facial asymmetry with loss of lip support and severe halitosis [Figure 1]. The patient had naso-cutaneous fistula measuring 2.5 cm in diameter lateral to the root of nose and inferior to inferior orbital rim [Figure 2]a. On intraoral examination, the patient revealed atrophic oral mucosa, reduced salivary flow, and large Aramany's Class lV maxillary defect with extra-oral communication. On examination, palatal defect was extending medially from median suture to alveolar ridge laterally. Antero-posteriorly defect was extended from lip to posterior border of the hard palate. There was no superior border since the palatal defect was directly connected with the facial defect [Figure 2]b. The patient presented with extracted maxillary right third molar to left lateral incisor with other teeth present. The patient also showed generalized severe attrition and abrasion of teeth with dentinal hypersensitivity. The patient also revealed generalized periodontitis and gingival recession with poor oral hygiene. Depending on history and clinical findings treatment plan was divided into three phases: Phase I included pre-prosthetic phase where surgical obturator was in place for 1 week (3 months); phase II included fabrication of intraoral and extra oral prosthesis (6-10 months); phase III involved reconstructive plastic surgery or replacement with definite prosthesis depending on the overall response and general medical health of the patient. [5] T reatment plan was explained to the patient and photographs, radiographs, and informed consent was obtained. Depending on the clinical finding, magnets were considered as an added mode of retention with wrought stainless steel wire clasps for interim obturator.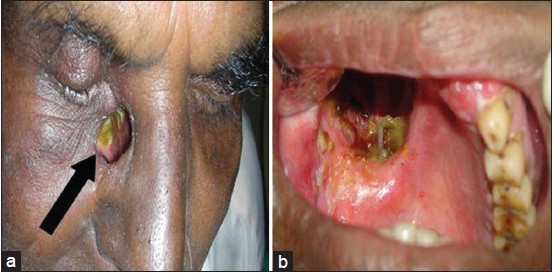 | Figure 2: (a) Extra-oral view, arrow indicates nasocutaneous fistula. (b) Intraoral view, indicates Aramany's Class IV maxillary defect
Click here to view |
For fabrication of intraoral prosthesis, impressions of both arches were made with irreversible hydrocolloid (Tropicalgin Chromatic, Zhermack, Badia Polsine, Italy) using stock trays after appropriate block-out of the defect and poured in type III dental stone (Kalstone, Kalabhai Karskarson Pvt. Ltd., Mumbai, India) and custom tray was fabricated auto-polymerizing acrylic resin (DPI-cold cure, Dental Products of India Ltd., Mumbai, India) after adequate spacer thickness of 4 mm. A final impression was made of the remaining palate and the surgical defect with medium-body addition silicone impression material (Extrude XP; Kerr Corporation, Orange, California, USA) in the modeling compound border-molded custom tray and poured in type IV die stone (Ultrarock, Kalabhai Karskarson Pvt. Ltd., Mumbai, India.) to obtain master cast. After block-out of the master cast, the casts were mounted on a semi-adjustable articulator (Hanau Wide-Vue, Waterpik, Fort Collins, USA) using face-bow transfer and a centric relation record. After evaluation of the teeth trial, the palatal portion of the obturator was processed with heat-curing acrylic resin (DPI-heat cure, Dental Products of India Ltd., Mumbai, India) with incorporation of retentive wrought stainless steel wire clasps. To fabricate bulbal portion of the obturator, blocked-out wax was removed and it was waxed with 6 mm of pink base-plate wax on the master cast (to incorporate 3-mm thick disc shaped magnet) and processed with heat-curing acrylic resin (DPI-heat cure, Dental Products of India Ltd., Mumbai, India). Processed bulbal portion of obturator was indexed with palatal portion and sealed with pink autopolymerizing acrylic resin (DPI-cold cure, Dental Products of India Ltd., Mumbai, India). Position of the magnet was evaluated from the extraoral defect on the intraoral prosthesis and a 3-mm thick and 2.5 cm in diameter, disc-shaped attractive Co 5 -Sm magnet (Innovadent, Dental ventures of America, Corona, USA) with magnetizable metal ferromagnetic keeper was attached with (DPI-cold cure, Dental Products of India Ltd., Mumbai, India). The finished prosthesis was evaluated intraorally and adjusted and polished [Figure 3]a and b.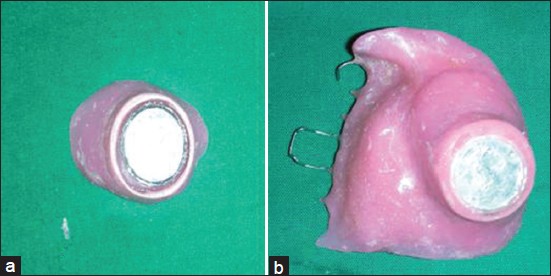 | Figure 3: (a) Finished extra-oral prosthesis with magnet attachment. (b) Finished maxillary interim obturator (intaglio surface) with magnet attachment with retentive wrought stainless steel clasps
Click here to view |
For fabrication of extra-oral prosthesis, final impression was made on auto-polymerized custom stent of appropriate diameter and length as core. Final impression was made with high-viscosity putty impression material (Extrude XP; Kerr Corporation, Orange, California, USA) after blocking out of undesirable undercut areas in the defect. The impression was removed and invested in type III dental stone (Kalstone, Kalabhai Karskarson Pvt. Ltd., Mumbai, India) to obtain two piece moulds. On the external surface of the mould, cast circumferential bevel was created to make prosthesis margins inconspicuous. The prosthesis was waxed carefully by keeping it hollow and external surface duplicating the internal anatomy of the defect, and external prosthesis junction was established at 2 mm from the mucocutaneous junction. A 14-gauge stainless steel wire was inserted along the length of the wax form to evaluate prosthesis fit and its accurate position radiographically on lateral cephalogram. The wax form was processed in pink heat-polymerizing acrylic resin (DPI-heat cure, Dental Products of India Ltd., Mumbai, India) after initial try in. The extraoral part of the prosthesis was tinted with oil-based paint (Tri-Star Colman; Tri-Star Creative Products Private Ltd., Noida, Uttar Pradesh, India.), mixed, and incorporated into the heat-polymerizing acrylic resin to match skin color of the patient. The prosthesis was retrieved, trimmed, and well-polished to prevent injury to the friable mucosa and the growth of microorganisms. Care must be taken not to reduce the retentive extensions and the areas of the extraoral wing that prevent displacement of the prosthesis. On the tissue side of the prosthesis, a 3-mm thick and 1 cm in diameter, disc-shaped attractive Co 5 -Sm magnet (Innovadent, Dental ventures of America, Corona, USA) was attached with (DPI-cold cure, Dental Products of India Ltd., Mumbai, India) [Figure 3]a and b. Both the prosthesis were seated in place and evaluated for its precise fit and accuracy of orientation of both sections, strength of magnetic field, retention, stability, and occlusal harmony [Figure 4] and [Figure 5].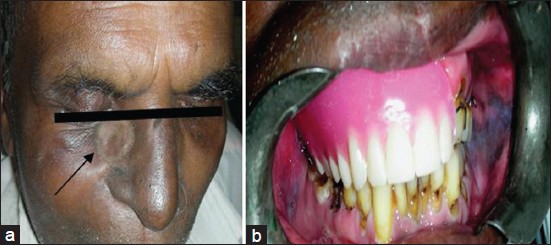 | Figure 4: (a) Extra-oral view. Arrow indicates prosthesis in place. (b) Intra-oral view, prosthesis in place
Click here to view |
The patient was instructed regarding the method of placement and removal of the sections as well as the techniques for cleansing of the prostheses and anatomic defects at home. Removal of the extraoral prosthesis can usually be achieved by digital pressure to the side of the nose. Patient was recalled on frequent appointments to eliminate pressure areas and adjustments and to ascertain proper tissue healing and patient comfort. For future treatment, the patient was planned for either reconstructive plastic surgery to close nasocutaneous fistula or defect of both, or definitive prosthesis with complete rehabilitation of oral tissues depending on the patient's overall general health and immunological status.
| Discussion | | |
Acquired diseases like malignancies can cause tremendous psychological, functional, and surgical effects on human beings. A proper treatment plan for a maxillary resection requires a presurgically assessment of the patient by a team consisting of surgeons and prosthodontists. If the defect is not surgically reconstructed, an immediate surgical obturator is indicated for the closure of defect, supporting the surgical dressing and restoring oral function. In order to overcome the complication of the postsurgical radiation therapy and in view of patient's reduced immunological response, the patient was planned for the interim prosthesis. An intact delayed surgical obturator was placed in the present case and responded with well-healed surgical site at the time of evaluation and was coping with normal activities reasonably well, although the large maxillary defect was not surgically reconstructed or rehabilitated with an obturator prosthesis. Aramany's Class lV defect creates a unilateral linear design problem where leverage cannot be used to an effective degree and retention is problematic. [6],[7],[8],[9] Use of magnets have advantages of self-seating, constant retention, small size prosthesis with strong attractive forces, dissipates lateral functional forces, and magnets are placed within prosthesis, and reduces the weight of the prosthesis. [3] Acrylic resin extra oral prosthesis was planned to reduce the cost of the prosthesis as being it interim. In future, in fabrication of definite prosthesis, it could be replaced with silicone material. Phase III of the treatment plan depends on patient's response to the radiotherapy, maintenance of interim prosthesis, and overall general health of the patient.
Routine insertion and withdrawal of the prosthesis requires considerable psychomotor skill from the patient. Proper patient training and meticulous oral hygiene maintenance were instituted to improve the prosthetic prognosis. The disadvantage of this approach is that a few additional laboratory steps were necessary for the fabrication of the prosthesis and corrosion of magnet in oral environment, which has to be maintained well. An experienced dental technician and a dental laboratory in close proximity are the major assets in the management of such clinical presentation. The obturator prosthesis demonstrated adequate retention, stability, and support with restoration of patient's deglutition, speech, articulation, esthetic, and psychological well-being. [10]
| References | | |
| 1. | Buller AS, Sela M. Acrylic resin prosthesis for obturation of an orocutaneous fistula. J Prosthet Dent 2007;97:179-80. 
|
| 2. | Robinson JE. Magnets for the retention of a sectional intraoral prosthesis: A case history. J Prosthet Dent 1963;13:1167-71.
|
| 3. | Nadeau J. Maxillofacial prosthetics with magnetic stabilizer. J Prosthet Dent 1956;6:114-9.
|
| 4. | Nadeau J. Special prostheses. J Prosthet Dent 1968;20:62-76.
|
| 5. | Cheng AC, Somerville DA, Wee AG. Altered prosthodontic treatment approach for bilateral complete maxillectomy: A clinical report. J Prosthet Dent 2004;92:120-4.
|
| 6. | Aramany MA. Basic principles of obturator design for partially edentulous patients Part I: Classification. J Prosthet Dent 1978;40:554-7.
|
| 7. | Aramany MA. Basic principles of obturator design for partially edentulous patients Part II: Design principles. J Prosthet Dent 1978;40:656-62.
|
| 8. | Parr GR, Gardner LK. The evolution of the obturator framework design. J Prosthet Dent 2003;89:608-10.
|
| 9. | Parr GR. Prosthodontic principles in the framework design of maxillary obturator prosthesis. J Prosthet Dent 1989;62:205-12.
|
| 10. | Panje WR, Hetherington HE, Toljanic J, LaVelle WE, Fyler A. Bilateral maxillectomy and midfacial reconstruction. Ann Otol Rhinol Laryngol 1995;104:845-9.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5]
|











 Search Pubmed for
Search Pubmed for