|
 
 |
| CASE REPORT |
|
| Year : 2014 | Volume
: 2
| Issue : 3 | Page : 89-92 |
|
Claspless denture design using milled abutment surfaces as precision attachment
Ajay Jain1, Sharad Vaidya2, Sridevi Ugrappa3, Charu Kapoor4
1 Department of Prosthodontics and Implantology, Institute of Technical Sciences Centre for Dental Studies and Research, Ghaziabad, Uttar Pradesh, India
2 Departments of Prosthodontics and Implantology, Bhojia Dental College, Baddi, Himachal Pradesh, India
3 Department of Oral Medicine and Radiology, Sri Sai College of Dental Surgery, Vikarabad, Andhra Pradesh, India
4 Departments of Oral Pathology and Microbiology, Bhojia Dental College, Baddi, Himachal Pradesh, India
| Date of Web Publication | 10-Sep-2014 |
Correspondence Address:
Sharad Vaidya
Department of Prosthodontics and Implantology, Bhojia Dental College, Baddi, Solan, Himachal Pradesh
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2347-4610.140518

This case report describes the combined use of fixed partial denture prosthesis (FPD) and removable partial denture (RPD) prosthesis for a patient with partially edentulous arches and few remaining teeth. The RPD was designed such that it would take advantage of benefits from milled palatal surfaces of the FPD to enhance stability and retention of the RPD and allow maitainance of oral hygiene.
Keywords: Extracoronal and intra-coronal attachments, milled abutment, precision attachment
How to cite this article:
Jain A, Vaidya S, Ugrappa S, Kapoor C. Claspless denture design using milled abutment surfaces as precision attachment
. Eur J Prosthodont 2014;2:89-92 |
| Introduction | |  |
Prosthetic rehabilitation of the complex partially edentulous patients using the combination of fixed and removable partial dentures and precision/semi-precision attachments as retentive elements has long been considered as one of the most sophisticated forms of treatment. The amount of remaining tooth structure is extremely critical for the accommodation of an intra-coronal precision attachment and requires additional removal of tooth structure to maintain tooth form. [1],[2] The placement of extra-coronal precision attachment often creates contours that are difficult to keep free of plaque, and the placement may alter the emergence profile of the crown as well, resulting in compromised periodontal tissues. Because of these complications, it would seem advisable to limit the use of precision attachments if other viable treatment options exist and if esthetics will not be compromised. The combination of fixed and removable partial denture involves full veneer crowns and the creation of milled guiding planes on the lingual surfaces that can serve as precision attachments to enhance the stability and retention of the removable partial denture. [3],[4],[5] This article presents a case report of rehabilitation of partially edentulous maxillary arch with the combination of fixed-removable prosthesis.
| Case Report | | |
A forty-year-old female patient was referred from the Department of oral and maxillofacial surgery after extraction of periodontally compromised teeth [Figure 1] and [Figure 2]. Intraoral examination revealed unhealed sockets in relation to maxillary left premolar region. The patient was recalled after a period of 2 weeks for the complete healing to take place. A variety of treatment options were presented to the patient including single tooth implants in edentulous areas but were rejected by the patient. For financial reasons as well as technical considerations, the definitive treatment plan included maxillary milled precision fit cast partial denture with crowns on a few natural teeth and mandibular conventional complete denture. | Figure 1: (a) Pre-operative view of maxillary and mandibular arch showing carious 12, 27, and unhealed sockets in the region of 24 and 25, (b) Completely edentulous mandibular arch
Click here to view |
| Procedure | | |
Upper and lower casts were mounted on semi-adjustable articulator to evaluate the inter-arch space. On the maxillary arch right lateral incisor, left canine, and first molar were planned to receive single metal ceramic crowns. Preparations were finished and definitive impression was made in rigid impression material (Affinis, Coltene/Whaledent, Altstätten, Switzerland). Full-contour diagnostic waxing (GEO Milling wax, Renfert, Germany) was completed with parallel guide planes on proximal and lingual tooth surfaces. The posterior milled surfaces were limited to the coronal two-third of the fixed restorations to reduce the coverage of the gingival tissue by removable partial denture (RPD). The width of the lingual ledge rest was 1.0-1.2 mm, and the lengths of vertical guide planes were 3.0-4.0 mm [Figure 3]. The parallel surfaces, combined with an accurate RPD casting, would provide for some frictional retention for the partial denture.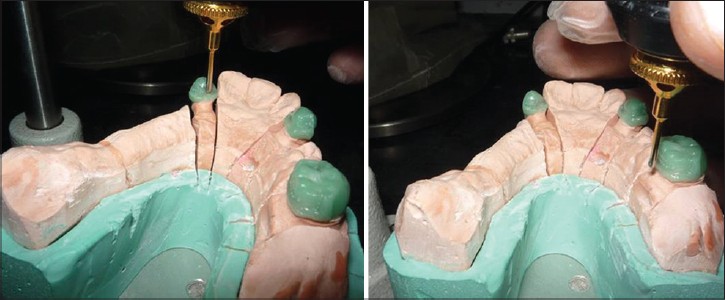 | Figure 3: Wax patterns cut back and milled in wax on posterior palatal surface to create positive rests and guide plane components
Click here to view |
The crowns were cast (Olympia; Jelenko) and verified intraorally before the addition of porcelain (Ceramco 3, Dentsply, USA; [Figure 4]). A rigid impression material (Affinis, Coltene/Whaledent, Altstätten, Switzerland) was used to transfer the individual crowns for RPD definitive cast [Figure 5]. Provisional cement (TempBond; Kerr Corp, Orange, Calif) was placed in small amounts to stabilize and retain the crowns before the definitive impression. The intaglio surfaces of the crowns were lubricated with petroleum jelly. The impression was poured in type IV stone (Kalrock, Kalabhai Karson, Mumbai). After recovery of the definitive cast, final milling was completed using an electrical milling machine (Schick Dental Gerade, Germany) with a fine milling bur [Figure 6]. The definitive cast was sent to a commercial dental laboratory for block-out and duplication. Commercially available wax patterns (Bego, USA) were used to create the major connector and finish lines [Figure 7]. The wax framework was sprued, invested, and cast (Jelenko JD; Jelenko) in the conventional manner. The internal surface of the casting was left in the as-cast condition in the areas in contact with the milled surfaces while all other surfaces received a normal finish and polish. | Figure 6: Metal surfaces of guide planes; final milling with milling burs
Click here to view |
 | Figure 7: (a) Wax pattern of cast partial framework on refractory cast, (b) Cast partial framework
Click here to view |
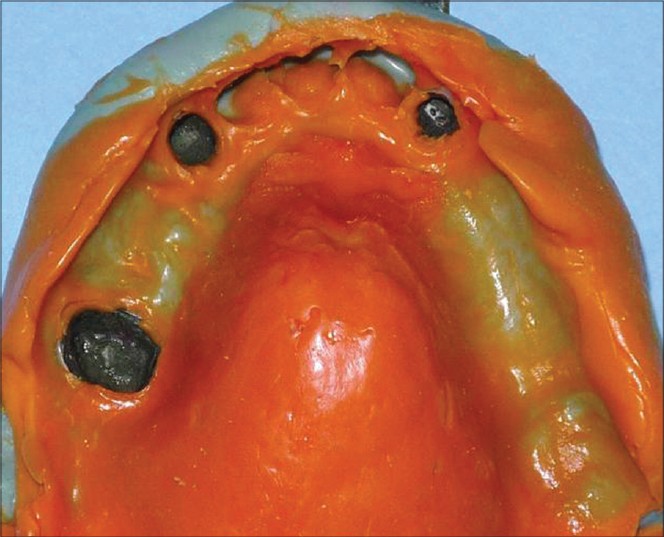
The framework was checked for the initial intraoral fit with the crowns cemented to the teeth. After assuring the complete seating of the framework, an over-impression was made with the framework [Figure 8] and the cast was poured in type IV dental stone. It is essential that the component fit both intra-orally and on the definitive cast in an identical manner so that errors are not induced during resin processing. Artificial teeth were positioned in balanced occlusion, waxing and carving was completed, following which the denture was processed, finished, and polished [Figure 9]. Instructions regarding insertion, removal, oral hygiene, and required home care were given to the patient.
| Discussion | | |
Oral rehabilitation of complex partially edentulous arches is one of the most challenging situations that a dentist could come across. Among the various treatments available, implant-supported prosthesis serves to be the finest treatment because there is a large population that does not opt for this treatment due to financial constraints. Amalgamation of fixed and removable partial denture prostheses with milled surfaces serves to be an acceptable option in these situations. Yada et al. explained the philosophy of combined prosthesis: (1) The major and minor connector should cover minimum amount of soft tissue while being in contact with the remaining teeth, (2) the milled palatal and proximal surfaces, which are left in the as-cast state, create frictional retention and enhance stability. [3],[4],[6],[7] Axial surfaces, milled to perfection, are only half of the equation. The framework must have maximal possible contact with the milled surfaces so that they function as precision attachments.
In the maxillary arch, right lateral incisor, left canine, and first molar teeth were planned to receive single metal ceramic crowns and RPD. Antero-posterior palatal strap was the major connector of choice as it derived good support from the tissues of hard palate despite its open design. The shape of the connector provides L-beam effect, thereby increasing the resistance to flexure. In general, the retention of RDPs is achieved through clasps, adhesive attachments, crowns, and fixed partial dentures with intra- or extra-coronal attachments, but in this particular case, the friction achieved between two semiprecious alloys forms the basis of retention. While clasps potentially interfere with aesthetic demands in the anterior region, friction fit design is not visible from the facial aspect. Different methods have been described viz. milling via CAD/CAM and spark erosion in the literature for the fabrication of removable partial dentures. Spark-erosion techniques allow the creation of very precise restorations for implant-supported as well as tooth-supported removable prostheses. This technique offers maximum stability and retention. Unfortunately, such precisely fitting superstructures are so expensive that cost precludes their use for most patients, as in our case. The laboratory cost for spark-eroded castings is about 1.5-2 lakh rupees (Indian currency), and the prosthesis must be created in a laboratory specially equipped to provide this service. An alternative type of prosthesis, developed with the refined techniques used for removable partial dentures, can offer similar results at a fraction of the cost. [7]
The greatest possibility of error in the creation of a precise fit between the milled surface and the casting occurs through the procedures employed in finishing and polishing. The uncontrolled loss of metal that normally occurs in the fitting phase dramatically alters the fit of the casting to the milled surface. Every effort must be made to leave the internal surface of the casting in the as-cast condition in the areas of desired contact with the milled surfaces. The laboratories must neither electro strip these surfaces nor grossly grind them to fit the frame to the master cast. Rather, the fitting of the frame must be first done in the mouth with all restorations present. Accuracy of the cast metal depends on the expansion of the refractory cast. It has been stated that even an error of 1 mL of liquid will alter the powder/liquid ratio so that a discrepancy can be seen clinically. The dental laboratory must give the highest level of attention to the accurate measurement of both powder and liquid when pouring the duplicated refractory cast. [8],[9],[10]
The major drawback with a conventional RDP is the continued loss of teeth after the restoration. Moreover, plaque retention, fracture of the components, periodontal ligament (PDL) breakdown of the abutment teeth, and unacceptable aesthetics adds to the failure of these prostheses. Clinical studies report that the PDL condition of surviving abutment is related to RPD designs and oral hygiene. By incorporating the milled guide plane on the palatal aspect of (FPD), improvement in the stability of RPD increased its resistance to rotational movements and most importantly eliminated the need for visible anterior clasping, thus achieving the basic principles of retention, stability, and support along with patient compliance. [11],[12]
| Conclusion | | |
When limitations exist with respect to either finances or the number of missing teeth in an arch, a combination of fixed and removable prostheses with milled contacting surfaces should be considered. The creation of milled parallel surfaces in natural or restored abutment teeth, coupled with removable partial denture castings that have optimal contact with these preparations, results in a path of insertion and removal that is controlled in a manner similar to one using conventional precision attachments. Because the milled surfaces are primarily extra-coronal, little, if any, additional tooth reduction is required for adequate mouth preparation. Avoiding additional tooth reduction minimizes abutment fracture in later junctures. The great increase in stability and resistance to rotational movements, when combined with conventional posterior clasping, provides a reasonable alternative to the precision attachment in providing maximal aesthetics in partially edentulous patients. In cases of fixed-removable restorations with precision attachments, abutment selection is crucial for the long-term success of the whole restoration when the removable denture is retained by only two or three selected abutment teeth of the remaining dentition. Because abutment loss will usually result in costly repair or redoing of the complete restoration, only teeth with an excellent prognosis should be selected to retain RPD.
| References | | |
| 1. | Brudvik JS, Shor A. The milled surfaces as a precision attachment. Dent Clin North Am 2004;48:685-708. 
|
| 2. | Owall B. Precision attachment removable partial dentures. Technical long-term study. Int J Prosthodont 1991;4:249-57.
[PUBMED] |
| 3. | Kern M, Wagner B. Periodontal findings in patients 10 years after insertion of removable partial dentures. J Oral Rehabil 2001;28:991-7.
|
| 4. | Chaiyabutr Y, Brudvik JS. Removable partial denture design using miled abutment surfaces and minimal soft tissue coverage for periodontally compromised teeth: A clinical report. J Prosthet Dent 2008;99:263-66.
|
| 5. | NaBadalung DP, Nicholls JI, Brudvik JS. Frictional resistance of removable partial dentures with retrofilled resin composite guide planes. Int J Prosthodont 1997;10:116-22.
|
| 6. | Brudvik JS. Advanced removable partial dentures. Chicago: Quintessence; 1999. p. 65-73.
|
| 7. | Brudvik JS, Reimers D. The tooth-removable partial denture interface. J Prosthet Dent 1992;68:924-7.
|
| 8. | Cholia SS, Wilson PH, Makdissi J. Multiple idiopathic external apical root resorption: Report of four cases. Dentomaxillofac Radiol 2005;34:240-6.
|
| 9. | Zlataric DK, Celebic A, Valentic-Peruzovic M. The effect of removable partial dentureson periodontal health of abutmentand non-abutment teeth. J Periodontol 2002;73:137-44.
|
| 10. | Zitzmann NU, Hagmann E, Weiger R. What is the prevalence of various types of prosthetic dental restorations in Europe? Clin Oral Implants Res 2007;18 Suppl 3:20-33.
|
| 11. | Kuzmanovic DV, Payne AG, Purton DG. Distal implants to modify the Kennedy classification of a removable partial denture: A clinical report. J Prosthet Dent 2004;92:8-11.
|
| 12. | Zitzmann NU. Point of care: When restoring the teeth of partially edentulous patients with removable partial dentures, do you consider placing implants to enhance the retention and stability of the prosthesis? J Can Dent Assoc 2005;71:552-3.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7], [Figure 8], [Figure 9]
|












 Search Pubmed for
Search Pubmed for