|
 
 |
| REVIEW ARTICLE |
|
| Year : 2015 | Volume
: 3
| Issue : 1 | Page : 10-15 |
|
Preventive aspect of prosthodontics: An overview
Rina Singh1, Jagjit Singh2, Ramandeep Singh Gambhir3, Kavalbir Singh Bhinder4
1 Department of Prosthodontics, Gian Sagar Dental College and Hospital, Rajpura, India
2 Department of Periodontics, Himachal Institute of Dental Sciences, Paonta Sahib, Himachal Pradesh, India
3 Department of Public Health Dentistry, Gian Sagar Dental College and Hospital, Rajpura, India
4 Department of General Dentistry, Dental Aesthetix Centre, Phase-7, Mohali, Punjab, India
| Date of Web Publication | 5-Jan-2015 |
Correspondence Address:
Dr. Ramandeep Singh Gambhir
Department of Public Health Dentistry, Gian Sagar Dental College, Rajpura - 140 601, Punjab
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2347-4610.148510

Prosthetic dentistry is one of the fundamental pillars of dentistry. The most effective prosthetic prophylaxis could be the prevention of causes leading to tooth extractions. As a dentist our main aim should be prevention, which not only includes prevention of caries and or periodontal disease but also prevention of residual alveolar bone loss after teeth are extracted Modern treatment options improve the overall prognosis of the stomatognathic system and the quality of life of the affected patients significantly. Preventive prosthodontics highlights the importance of any procedure that can delay or eliminate future prosthodontic problems. The present review was conducted after doing extensive literature search of peer-reviewed journals and extracting information on the concept of preventive prosthodontics. The present paper discusses the concept of preventive prosthodontics engaging all the three levels of prevention-primary, secondary and tertiary. Procedures and prosthetic interventions that can be undertaken in each level are discussed. Keywords: Implants, levels, prevention, procedures, prosthodontics
How to cite this article:
Singh R, Singh J, Gambhir RS, Bhinder KS. Preventive aspect of prosthodontics: An overview. Eur J Prosthodont 2015;3:10-5 |
| Introduction | |  |
Life expectancy has increased substantially since the beginning of 20 th century. Average life expectancy about 2000 years back was 20-30 years. According to a survey in 1910 in USA, the life expectancy was calculated to be around 45-30 years. [1] In 1986, average life expectancy in men was seen to be 65-70 years and in women it was 70-78 years After the year 2010, number of elderly people will increased rapidly and 1 in 4 people is above the age of 65 years. [2] The growing population of elderly people has not only increased their medical needs but also the dental needs. [3]
Preventive dentistry is defined as procedures employed in practice of dentistry and community dental health programs, which prevent the occurrence of oral diseases and oral abnormalities. [4] There are many forms of preventive dentistry, such as daily brushing and annual dental cleanings. These practices are designed to ensure that teeth are clean, strong, and white. The branch of the dentistry pertaining to the restoration and maintenance of oral function, comfort, appearance and health of the patient by the restoration of the natural teeth and/or the replacement of missing teeth and craniofacial tissues with biocompatible substituents is termed as "Prosthodontics." [5] The most effective prosthetic prophylaxis could be the prevention of causes leading to tooth extractions. As now the caries and the periodontal prevention are not efficient enough we are obligated to deal with the consequences of tooth loss. [6] Within the framework of "Preventive Prosthodontics," attention is focused on prevention of defects of the oral tissues, as well as the prevention of alveolar bone resorption.
| Literature Search | | |
A comprehensive of the literature search was done (electronic and manual) which engaged most of the articles published in peer-reviewed journals relating to the subject of preventive prosthodontics. The review itself began with the search of relevant key words linked with prosthetic dentistry like prevention, prosthodontics, primary, dentistry, levels, implantology etc., in various search engines including PubMed, MEDLINE, etc. Reports published only in English language were included in the review. The spotlight of the present review would be on various preventive procedures that can be done in prosthetic dentistry. The review also targeted preventive techniques in oral implantology that can be used to minimize alveolar ridge resorption after tooth extraction.
These are the actions taken to prevent the factors, which affect the normal oral function, comfort, health, appearance and general health of the patient. Preventive prosthodontics includes the prevention of the factors which affects the dental structures, supporting structures such as periodontium, alveolar bone, basal bone and surrounding musculo-skeletal structures like muscles of mastication, facial expression, temporomandibular joint (TMJ), maxilla and surrounding cranium. [7]
| Preventive Prosthodontics at Primary Level | | |
It is a prepathogenic phase. It includes the steps like health promotion and specific protection. Dental caries prevention, plaque control, regular checkup for caries activity diet counseling etc., are included in health promotional phase at primary prevention level. Specific protection includes topical fluoride application and application of pit and fissure sealants. [8] In the case of the old patients due to decreased salivation, gingival recession root exposure, cervical abrasion, attrition, an increase risk of the caries susceptibility is there. So for these patients fluoride rinses and fluoridated tooth pastes are recommended.
Correction of mal-aligned teeth if any and regular care for the prosthesis like complete dentures, removable partial dentures and fixed partial dentures is essential. The patient is also educated about the chewing habits, tongue postures for better maintenance of the occlusion and maintenance of the prosthesis. [9] The jaw exercises are recommended for the complete denture patients because complete edentulousness may alter the normal muscle engrams. The primary prevention also involves the protection of the dentoalveolar structures by providing mouth guards for the personals involved in contact sports and radiation shields for the patients who are undergoing the radiotherapy. [10]
| Mouth Guards | | |
The mouth guards are indicated to prevent the dental and dentofacial injuries in contact sports [Figure 1]. The injuries such as tooth fractures, concussion, crown root fractures, TMJ fractures, dentoalveolar fractures, soft tissue injuries can be prevented or minimized. [11] Use of mouth guards reduced the risk of dental and maxillofacial trauma <7.5%. The mouth guards with moderate resiliency absorb the forces, protect the teeth, TMJ and prevent the contact of teeth and thus prevents ankylosis. [12]
| Protection against the Radiation Injuries during Radio Therapy | | |
Some authors have recommended protecting the adjacent tissues during radiotherapy in the maxillofacial region by shielding with the appropriate shields. The protection can be provided by various methods like providing the radiation docking (cone positioning) devices, making spacers in the interstitial brachytherapy for tongue cancer and fabrication of tongue shields. [13] Radiation locking devices are utilized for directing the radiation cones for a particular area of the oral cavity. In many conditions, the radiation therapy has to be provided in divided doses. In those conditions, the docking device helps in the proper orientation of the radiation cones and also protects the adjacent soft tissue by deflecting them out of the radiation path. [14] When other areas of the oral cavity are irradiated, the tongue needs to be protected. This can be done with the help of tongue shielding radiation stent. [15]
| Preventive Prosthodontics at Secondary Level | | |
It includes the early detection of the disorders and providing prompt treatment. Various treatment modalities include preventive resin restorations of initial caries, direct and indirect pulp protection scaling and curettage, etc. [16] Preventive prosthodontic procedures which can be performed at this level are- occlusal interference correction, treatment for bruxism, treatment for trauma from occlusion (TFO), correction of plunger cusps and treatment of obstructive sleep apnea. [17]
| Occlusal Interference | | |
Any tooth contact that inhibits the remaining occluding surface from achieving stable and harmonious contact. Occlusal interference produces mandibular deviation during closure to maximum intercuspation (MIC) position or may hinder the smooth passage to and from MIC position. The inference may be also be present during latero-trusive movements and protrusive movements. [18] If the occlusal interference cross the threshold of adaptive capacity of the Temporo-mandibular joint, muscles of mastication and neuromuscular system, it leads to muscle hypertrophy, muscle fatigue, spasm, headaches, cranio-mandibular dysfunction syndrome, wear facets, fractured cusps, tooth mobility. Parafunctional habits like bruxism. So correction of occlusal interference is recommended in the early stages. Care should be taken during the occlusal correction, if not it may aggravate the situation. [19]
| Bruxism | | |
If occlusal interferences are present, the patient tries himself to equilibrate the occlusion and thus develop the habit of clenching or grinding of teeth. This can occur due to periodontitis, over a contoured restoration, psychological and physical stresses, sleep disorder, central nervous system disturbances and alcohol. [20] Bruxism leads to attrition, mobility, muscle hypertrophy, occlusal facets, alveolar bone loss and TMJ disorders. Symptoms include muscle soreness, fatigue of masticatory muscle early in morning, hypermobility, hypercementosis, cusp fractures, pulpitis break in lamina dura, furcation involvement. Treatment of bruxism involves controlling the psychological stress, occlusal correction, coronoplasty and occlusal splints or intraoral orthoses. [21]
| Trauma from Occlusion | | |
It is a reversible condition. When occlusal forces exceed the adaptive capacity of the periodontal tissues, tissue injury results. This tissue injury is called as TFO. Acute TFO is due to sudden heavy forces. Chronic TFO is due to continuous and long duration occlusal forces, e.g. bruxism, drifting and extrusion of the teeth. Primary TFO is caused due to high occlusal forces whereas main cause of secondary TFO is a low threshold or low resistance of the periodontium. Occlusal corrections are needed for the correction of the TFO. [22]
| Plunger Cusps | | |
The cusps which wedge the food forcefully into the interdental spaces of the opposing arch. These plunger cusp are usually the functional cusp (i.e., palatal cusp of maxillary teeth and buccal cusp of mandibular teeth) and sometimes palatal incline of maxillary buccal cusp and buccal incline of lingual cusp. Treatment involves rounding and shortening of the plunger cusps, and the opposing interproximal space is protected by splinting the adjacent teeth. [23]
| Obstructive Sleep Apnea | | |
The role of dentistry in sleep disorders is becoming more significant, especially in co-managing patients with simple snoring and mild to moderate obstructive sleep apnea. [24] It is characterized by cessation of airflow through upper airway while diaphragm movement continues. It can cause due to enlarges tonsils, enlarged soft palate, large tongue and retrognathism. This can be taken care by fabrication of prosthetic mandibular advancement appliances like soft palate lifters, tongue retainers, mandibular repositioners, snore guards etc., and surgery to remove portions of the soft palate and uvula [Figure 2]. [25]
| Preventive Prosthodontics at Tertiary Level | | |
Tertiary level prevention involves limiting the disability of the patient and rehabilitation. Various dental procedures that can be performed include complex restorative treatment of decayed teeth, root canal treatment and extractions. Prosthodontic rehabilitation incorporates procedures like post and core treatment, removable partial denture, fixed partial denture and implants. [26]
| Prosthodontics Option in Disability Limitation and Rehabilitation | | |
In the year 1990, some authors presented the "preventive prosthetic treatment strategy" for treatment of the young patients with a highly mutilated dentition. [27] It includes restoration of the teeth, timing of extraction, preservation of occluding pairs of teeth, avoidance of contact between the teeth and the opposite edentulous jaw. In rehabilitation phase, planning for the immediate dentures, treatment dentures or interim dentures, complete dentures and provisional restorations can be done.
| Timing of Extraction | | |
Planned extraction of highly mutilated teeth prevents the rapid resorption of the alveolar ridges. Extraction of the maxillary third molar is delayed till the middle age. As third molars have their influence on growth of the tuberosity and help in the development of anterioposterior alveolar ridge. Careful extraction should be done to avoid the presence of unantagonized tooth. [28] If antagonists are not present, supra eruption of opposing dentition leads to contact between the mucosa and teeth of the opposing arches. As a result, arch stability is lost, and this leads to severe resorption of the alveolar ridge in edentulous arch.
| Interim Denture/Treatment Denture | | |
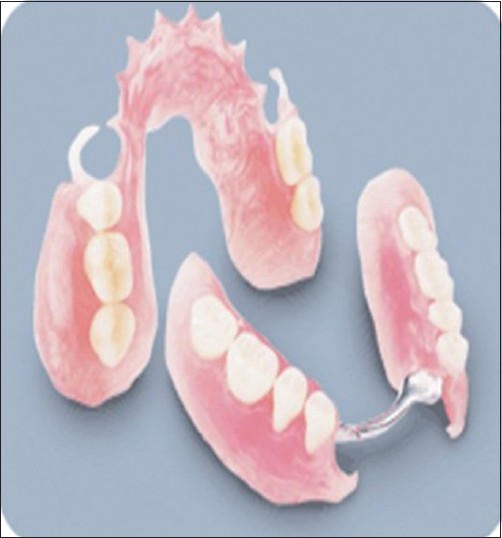
In the case of early loss of the permanent teeth, if the definitive treatment cannot be done for various reasons, the interim denture (treatment dentures) can be utilized as preventive measures [Figure 3]. The treatment dentures acts as space maintainers, prevent the migration/drifting, prevent the supra eruption and prevent the contact between the teeth, alveolar ridge, restore the function, esthetics, restore the muscular tonicity, restore the vertical height, jaw health and avoids the abnormal jaw habits. [29]
| Preservation of Occluding Pair of Teeth | | |
In the treatment of mutilated dentition, preservation of an incomplete dentition with a minimum of occluding pairs of teeth in combination with a partial denture is preferable than the total tooth extraction. This is advantageous for utilization of the natural teeth for retention and stability of the prosthesis. Presence of the periodontal ligament provides the advantage of biofeedback mechanism in controlling the occlusal forces. [30]
| Immediate Denture | | |
If the dentition is very compromised and indicated for total extraction, then immediate dentures are planned to promote better healing (immediate dentures act as surgical stents), protect the blood clot and aid early healing and promote better ridge form. The immediate dentures apply functional forces within the physiological limit results in an edentulous ridge with better form and more resilient soft tissue covering. [31] Immediate dentures also prevent the facial musculature from collapsing, provide a guide for the vertical dimension, esthetic, easy adaptation to the dentures and provide psychological comfort.
| Provisional Restorations | | |
After the tooth preparation is done for fixed prosthesis, provisional restoration is advocated to prevent the events like pulpal inflammation (pulp protection), mesial migration, supra eruption and arch integrity, protection of the tooth preparation margins (e.g., partial veneer crown) and protection of the periodontium. [32] Clinicians have many choices of provisional materials from which to choose when fabricating provisional restorations. While traditional materials are still in use today, temporary materials are continuously being updated and improved upon. In addition to the functional necessities required of the provisional material, it must also provide esthetic value for the patient. [33]
| Single Complete Denture/Complete Denture | | |
When the teeth are completely absent in any one of the arch, the fabrication of a single complete denture is highly recommended to prevent the contact of the teeth and alveolar ridge, to restore function, vertical dimension, esthetics and prevent the development of parafunctional habits. [34] The complete dentures are provided for edentulous patients (edentulous in both jaws) to rehabilitate them by restoring the function form and aesthetics and general health of the patients. The complete dentures are provided with various occlusal schemes such as balanced occlusion, lingualized occlusion, neutrocentric concept and others depending upon the condition of the patients. [35]
| Overdentures | | |
Some authors advised to retain the stumps beneath the artificial teeth, and stated that these roots maintain the alveolar bone health and height for longer duration. This can be achieved by fabricating an overdenture. [36] This can be advantageous in terms of conserving the natural teeth, reducing the rate of residual ridge resorption, proprioceptive feedback by existing periodontal ligaments and thus controlling the occlusive forces and preventing the rapid residual ridge resorption. [36]
| Obturator | | |
Obturator is a prosthesis used to close a congenital or acquired tissue opening primarily of the hard palate and contiguous alveolar tissues. [37] Immediate obturators are placed immediately after the surgery with or without surgical packing. It is retained by screws or wire fixation, re-establishes the oral contours, prevents the regurgitation of the fluids into nasopharynx, protects the wounds allows uneventful healing and prevents the cicatrisation or shrinkage. [38] Interim obturator is given after the removal of the surgical packing. The interim obturator is retained up to 3 months with repeated checking and relining with the tissue conditioner, followed by definitive obturator. [39]
| Preventive Implant Therapy | | |
Preventive dentistry is mainly concerned with caries and periodontal disease and little, or no attention is paid to the prevention of alveolar bone loss. Preventive implantology is concerned with the preservation of the alveolar ridge of the (edentulous) jaw. After tooth extraction, the atrophy of edentulous lower jaws can be prevented or delayed by using implants supporting an over denture or a fixed mandibular prosthesis. [40] Studies have shown that mandibular ridge shows a slower resorption pattern when it is loaded by implants supported prosthesis rather than a conventional mucosa supported dentures. Kalk et al. proposed the resorption stages of the residual ridges which are used in preventive implantlogy. [41]
Preventive stage I
Anatomic situation after tooth extraction. Further resorption can be prevented by implantation of the bone substituents. e.g. a non resorbable hydroxyl appetite.
Preventive stage II
After the initial resorption has occurred. In this case, further resorption can be prevented by placing cylindrical endosteal implants to maintain adequate width and height. [42]
Preventive stage III
Knife edged ridge. Bone removal is necessary for implant placement.
Preventive stage IV
Severe resorption of the alveolar ridge has taken place. Only basal bone is present. Implants are placed directly into the basal bone to prevent total loss of function of the arches.
| Conclusion | | |
Tough prosthodontics has evolved highly as a specialized field in replacement of missing teeth and adjacent soft and hard oral tissues; the cooperation with other aspects of dentistry, especially preventive cannot be ignored. Meeting the expectations of an ever increasing elderly population with quite rightly youthful outlooks of both function and esthetics is demanding. The loss of several teeth doesn't have to be an immediate threat to the function of the whole dentition, but it can initiate serious problems related to the whole orofacial region, psychics and the wellbeing of the patient. From this point of view prosthetic dentistry is a valuable tool with high therapeutical and preventive character. Clinical application of various preventive measures in relation to the function of the masticatory system as well as prosthetic treatment is reviewed in the above discussion. Potential problems can be avoided and resolved by properly instituting a preventive prosthodontic procedure or practice according to the degree or level of prevention needed to correct it.
| References | | |
| 1. | Salomon JA, Wang H, Freeman MK, Vos T, Flaxman AD, Lopez AD, et al. Healthy life expectancy for 187 countries, 1990-2010: A systematic analysis for the Global Burden Disease Study 2010. Lancet 2012;380:2144-62.  [ PUBMED] |
| 2. | Daniels N. Global aging and the allocation of health care across the life span. Am J Bioeth 2013;13:1-2. |
| 3. | Gulland A. People are living longer but are not in best health, global study finds. BMJ 2012;345:e8511. [ PUBMED] |
| 4. | Gerrie NF. A definition of preventive dentistry. J Public Health Dent 1969;29:60. [ PUBMED] |
| 5. | John MT, Reissmann DR, Szentpétery A, Steele J. An approach to define clinical significance in prosthodontics. J Prosthodont 2009;18:455-60. |
| 6. | Fazekas A. The fundamental method of preventive prosthodontics: Complex rehabilitation of the masticatory organ. Fogorv Sz 1992;85:71-9. |
| 7. | Payne SH. Preventive prosthodontics. J Prosthet Dent 1973;30:491. |
| 8. | Baelum V. Dentistry and population approaches for preventing dental diseases. J Dent 2011;39 Suppl 2:S9-19. |
| 9. | Peracini A, Andrade IM, Paranhos Hde F, Silva CH, de Souza RF. Behaviors and hygiene habits of complete denture wearers. Braz Dent J 2010;21:247-52. |
| 10. | Glenn G. Orthodontists encourage use of mouth guards for all contact sports. N J Nurse 2014;44:8. [ PUBMED] |
| 11. | Scott J, Burke FJ, Watts DC. A review of dental injuries and the use of mouthguards in contact team sports. Br Dent J 1994;176:310-4. |
| 12. | Barnett F. Prevention of sports-related dental trauma: The role of mouthguards. Pract Proced Aesthet Dent 2003;15:391-4. |
| 13. | Beumer J 3 rd , Silverman S Jr, Benak SB Jr. Hard and soft tissue necroses following radiation therapy for oral cancer. J Prosthet Dent 1972;27:640-4. |
| 14. | American Association of Physicists in Medicine. Protocols for the Radiation Safety Surveys of Diagnostic Radiological Equipment. New York: AAPM; 1988. Available from: http://www.aapm.org/pubs/reports/rpt_25.pdf. [Last accessed on 2014 Sep 30]. |
| 15. | Fleming TJ, Rambach SC. A tongue-shielding radiation stent. J Prosthet Dent 1983;49:389-92. [ PUBMED] |
| 16. | Gluzman R, Katz RV, Frey BJ, McGowan R. Prevention of root caries: A literature review of primary and secondary preventive agents. Spec Care Dentist 2013;33:133-40. |
| 17. | Davliakos J. Preventive and interceptive prosthodontics: Bridging the gap between restorative and implant dentistry. Interview. Dent Implantol Update 2003;14:81-7. [ PUBMED] |
| 18. | Simon J. Occlusal interference. Dentistry′s great imposter. Dent Today 2003;22:70-3. |
| 19. | Ishigaki S, Kurozumi T, Morishige E, Yatani H. Occlusal interference during mastication can cause pathological tooth mobility. J Periodontal Res 2006;41:189-92. |
| 20. | Feu D, Catharino F, Quintão CC, Almeida MA. A systematic review of etiological and risk factors associated with bruxism. J Orthod 2013;40:163-71. |
| 21. | Johansson A, Omar R, Carlsson GE. Bruxism and prosthetic treatment: A critical review. J Prosthodont Res 2011;55:127-36. |
| 22. | Pihlstrom BL, Anderson KA, Aeppli D, Schaffer EM. Association between signs of trauma from occlusion and periodontitis. J Periodontol 1986;57:1-6. [ PUBMED] |
| 23. | Khairnar M. Classification of food impaction-revisited and its management. Indian J Dent Adv 2013;5:1113-9. |
| 24. | Padma A, Ramakrishnan N, Narayanan V. Management of obstructive sleep apnea: A dental perspective. Indian J Dent Res 2007;18:201-9. [ PUBMED]  |
| 25. | Lamster IB, Eaves K. A model for dental practice in the 21 st century. Am J Public Health 2011;101:1825-30. |
| 26. | Gupta K, Javiya P, Kumar P, Mallikarjuna R. Rehabilitation of lost vertical dimension with cast post core and cast partial denture. BMJ Case Rep 2013;2013. |
| 27. | Kalk W, van Rossum GM, van Waas MA. Edentulism and preventive goals in the treatment of mutilated dentition. Int Dent J 1990;40:267-74. |
| 28. | Dua P, Singh JP, Aghi A. Aesthetic and functional rehabilitation of a case of mutilated dentition and loss of vertical dimensions. J Indian Prosthodont Soc 2011;11:189-94. |
| 29. | Smith DE. Interim dentures and treatment dentures. Dent Clin North Am 1984;28:253-71. [ PUBMED] |
| 30. | Hanlin SM. The mutilated dentition - Management of the debilitated dentition. Ann R Australas Coll Dent Surg 2012;21:49-50. [ PUBMED] |
| 31. | St George G, Hussain S, Welfare R. Immediate dentures: 1.Treatment planning. Dent Update 2010;37:82-4, 86. |
| 32. | Perry RD, Magnuson B. Provisional materials: Key components of interim fixed restorations. Compend Contin Educ Dent 2012;33:59-60, 62. |
| 33. | Strassler HE. Fixed prosthodontics provisional materials: Making the right selection. Compend Contin Educ Dent 2013;34:22-4, 26. |
| 34. | Vamsi Krishna CH, Rao AK, Sekhar NC, Shastry YM. Rehabilitation of maxillary arch with attachment-retained mesh-reinforced single complete denture. BMJ Case Rep 2014;2014. |
| 35. | Scott BJ, Hunter RV. Creating complete dentures that are stable in function. Dent Update 2008;35:259-62, 265. |
| 36. | de Souza BV, de Faria AD, Junior Joel Ferreira S, Gonçales VA, Piza PE, FellippoRamos V. Root-supported overdentures associated with temporary immediate prostheses - A case-report. Oral Health Dent Manag 2014;13:159-63. |
| 37. | Goyal M, Chopra R, Bansal K, Marwaha M. Role of obturators and other feeding interventions in patients with cleft lip and palate: A review. Eur Arch Paediatr Dent 2014;15:1-9. |
| 38. | Sinha D, Banerjee S, Chowdhury S. Fabrication of an immediate surgical obturator for a patient with resection of the maxillary antrum and bony orbital floor. J Prosthet Dent 2014;112:376-8. |
| 39. | Popli S, Parkash H, Bhargava A, Gupta S, Bablani D, Kar AK. A two-piece sectional interim obturator. A clinical report. J Prosthodont 2012;21:487-90. |
| 40. | Denissen HW, Kalk W. Preventive implantations. Int Dent J 1991;41:17-24. |
| 41. | Kalk W, Denissen HW, Käyser AF. Preventive goals in oral implantology. Int Dent J 1993;43:483-91. |
| 42. | Fagan MJ Jr. Preventive dentistry concepts for endosseous implantology. Oral Implantol 1974;4:345-9. [ PUBMED] |
[Figure 1], [Figure 2], [Figure 3]
|











 Search Pubmed for
Search Pubmed for