|
 
 |
| CASE REPORT |
|
| Year : 2015 | Volume
: 3
| Issue : 2 | Page : 47-50 |
|
Prosthetic treatment of nonsyndromic oligodontia
Müjde Sevimay, Ceyda Akın
Department of Prosthodontics, Faculty of Dentistry, Selcuk University, Konya, Turkey
| Date of Web Publication | 29-May-2015 |
Correspondence Address:
Dr. Müjde Sevimay
Department of Prosthodontics, Faculty of Dentistry, Selcuk University, Konya
Turkey
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2347-4610.157842

Oligodontia is the agenesis of six or more teeth, excluding the third molars. Genetic factors play an important role in oligodontia, which can occur as an isolated finding or as part of a syndrome. The characteristic dental symptoms are reduced number of teeth, reduction in tooth size, anomalies of tooth form, and delayed eruption. The absence of teeth in patients can cause aesthetic, functional, and psychological problems, particularly if the anterior region is involved. This case report describes the prosthetic treatment approach to a 19-year-old patient with nonsyndromic oligodontia characterized by the absence of 10 permanent teeth. The objectives of the treatment were the prosthetic restoration of the missing teeth and the provision of occlusion with full-mouth zirconia restorations. Keywords: Hypodontia, oligodontia, prosthetic therapy
How to cite this article:
Sevimay M, Akın C. Prosthetic treatment of nonsyndromic oligodontia. Eur J Prosthodont 2015;3:47-50 |
| Introduction | |  |
Agenesis of permanent teeth is one of the most common human developmental anomalies. [1],[2],[3] Hypodontia is the congenital agenesis of five or fewer permanent teeth, excluding third molars; oligodontia, which is also called severe hypodontia, [1],[4] is the congenital agenesis of six or more permanent teeth, excluding the third molars; [1],[5] and anadontia is the congenital agenesis of all deciduous and/or permanent teeth.
The prevalence values of oligodontia mentioned in the literature range from 0.08% to 1.1%. [1],[6] It affects females more often than males, with a gender ratio of 3:2. [7] Oligodontia can be found as an isolated nonsyndromic trait or as part of a malformative syndrome, [2],[5],[8],[9],[10] such as ectodermal dysplasia, [2],[3],[5],[10] Rieger's syndrome, [11] Van Der Woude syndrome, Down syndrome, oto-palato-digital syndrome, [10] Witkop syndrome (tooth and nail syndrome), [12] oro-facial-digital syndrome, [13] oculo-facial-cardio-dental syndrome, [10],[14] and incontinentia pigmenti. [10],[15] When part of a syndrome, oligodontia usually involves concomitant abnormalities in the skin, nails, ears, or skeleton. [2],[10],[12],[13],[14],[15] To date, mutations in the MSX1 or the PAX9 genes have been identified as a possible cause of nonsyndromic oligodontia. [16] In majority of the cases, it is transmitted as an autosomal dominant, autosomal recessive, or X-linked genetic condition. [17],[18],[19] Congenitally, absent maxillary lateral incisors, maxillary second premolars, and mandibular central incisors are commonly seen in oligodontia cases, [3] whereas the agenesis of maxillary central incisors, maxillary or mandibular canines, and first permanent molars are rare. [1] Moreover, oligodontia may result in several dental and oral symptoms, such as reduction in size and form of teeth and alveolar processes, delayed eruption of teeth, persistent deciduous teeth, anomalies of the enamel, increased free-way space and cleft lip/palate, false diastema, and deep overbite. [1],[5],[6],[9] Residual teeth can vary in size, shape, and rate of development, and the permanent dentition is more affected than the primary dentition. [20] Speech and masticatory functional disorders occur most frequently, but aesthetic, physiological, and psychological problems may also arise at an early age. [18],[21] Therefore, early diagnosis and treatment of these patients are important. Treatment options depend on the severity of the cases. Treatments can include orthodontic space opening or closure before prosthetic therapy; use of adhesive restorative techniques, removable or fixed partial dentures, and implant-supported restorations; or combinations of these approaches. [1]
This case report describes the prosthetic treatment approach to a 19-year-old patient with nonsyndromic oligodontia characterized by the absence of 15 permanent teeth.
| Case Report | | |
A 19-year-old female patient was referred to the Faculty of Dentistry, Department of Prosthodontics of Selcuk University for unpleasant smile and replacement of missing teeth.
Extra-orally, frontal and profile examination revealed a mild decrease in lower facial height and a flat profile. The nasolabial angle was within normal limits, and the lower lip was full and slightly protruded relative to the upper lip at closure.
Intraoral and radiographic examination revealed that 15 permanent teeth were developmentally missing: Maxillary first and third molars, mandibular incisors, mandibular right first and third molars, mandibular right second premolar, and mandibular left first and third molars. Maxillar deciduous lateral, premolar, canine, and mandibular deciduous premolars were present in the dental arches. The mandibular second premolar was impacted. The maxillary and mandibular first and second premolars had a marked conical shape, and the mesiodistal diameters of the teeth were reduced [Figure 1]. | Figure 1: Preoperative panoramic radiograph of the mouth, 15 permanent teeth are absent
Click here to view |
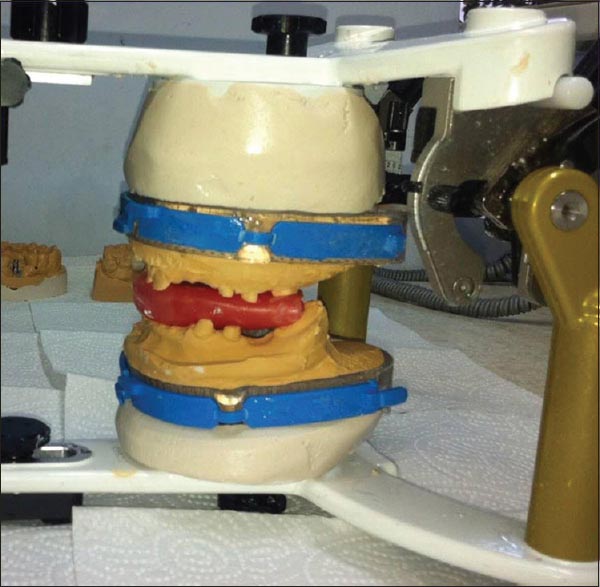
The treatment plan comprised two phases. Phase I consisted of the extraction of deciduous and impacted teeth. Phase II involved prosthetic therapy to provide function and aesthetics. After 2 weeks of extraction healing, the remaining teeth were prepared [Figure 2] and [Figure 3], and impressions were made. Theimpressions were poured using type II dental stone (Elite Model, Zhermack, Italy). Casts were mounted on the articulator with 2 mm increased occlusal vertical dimension (OVD). A 2 mm increase in OVD was determinedto facilitate the placement of fixed prosthetic restoration and to improve facial aesthetics. Then, full-mouth porcelain fused to metal restorations (VITA VM 13; VITA Zahnfabrik, Bad Sackingen, Germany) was fabricated at the newly established OVD. The restorations were fitted and adjusted in the mouth [Figure 4] and [Figure 5]. After provisional cementation, the restorations were maintained intraorally for 3 months before the final impressions were made. During this period, periodic recalls at intervals of 1-4 weeks were performed to evaluate the increased OVD. In the evaluation period, the patient's anterior and posterior speaking space and function were assessed. The muscles of mastication and the temporomandibular joint were evaluated for clinical signs of discomfort. Moreover, the temporomandibular joint was evaluated by taking magnetic resonance. The patient was asymptomatic and comfortable during this period. For the final restorations, the maxillary and mandibular impressions were made with a putty-wash technique using polieter (Ivoclar Vivadent AG, Schaan, Liechtenstein) impression material. Full-mouth zirconia restorations (Zirkonzahn GmbH, Bruneck/South Tirol, Italy) were fabricated using a semi-adjustable articulator [Figure 6]. Canine guidance was developed to reduce lateral forces in the posterior dentition. The restorations were cemented using polycarboxylated cement (Adhesor Carbofine, Spofa Dental, Frankfurt, Germany). In the final restorations, a diestema was found between the central incisors. When we made contact between the central incisors, they became larger and square shaped. Foraesthetic reasons and depending on the patient's request, a diestema could be left between the central incisors [Figure 7]a-c. | Figure 4: Metal adjustment of the provisional porcelain fused to metal restorations
Click here to view |
 | Figure 5: Maxiller and mandibular provisional restorations at the newly established occlusal vertical dimension
Click here to view |
 | Figure 7: (a) Lateral view (right side) of the final restorations (b) anterior view of the final restorations (c) lateral view (left side) of the final restorations
Click here to view |
The patient has been well functioning with her restorations for 12 months and is pleased with the treatment outcome.
| Discussion | | |
Nonsyndromic oligodontia is the most common developmental anomaly, and it presents many problems for both patient and clinician. [22],[23] Previous studies reported that mutations in the genes MSX1 and PAX9 that encode transcription factors were associated with nonsyndromic oligodontia. [23],[24] Whereas mutations in the MSX1 gene cause human tooth agenesis of various types of teeth, preferentially premolars, mutations of PAX9 could be the cause of the presented clinical report. Therefore, the genetic components behind the serious dental anomalies have to be revealed and taken into consideration.
Patients with this anomaly often seek treatment because of their unpleasant appearance, impaired mastication, and speech difficulties. [21] Moreover, the lack of uniformity of the occlusal plane, supereruption, loss of vertical dimension, and bone morphology in edentulous areas may cause prosthodontic challenges. [25]
In cases of multiple congenitally missing permanent teeth, an interdisciplinary approach may be required. A number of treatment options are available for these cases. For example, before the prosthetic treatment, the localizations of the teeth are corrected by orthodontic therapy. Direct composite restorations may be considered to reshape the conical teeth. In residuous spaces, implants are inserted, and implant-supported fixed partial dentures are planned. In the present case report, the patient rejected the orthodontic and implant treatment, and thus the definitive therapeutic approach was conducted using full-mouth, tooth-supported zirconia restorations to replace the missing teeth and to restore occlusion and OVD.
Subtle visual differences in facial soft tissue profiles were reported when OVD was increased by 2-6 mm with fixed restorations. [26] The facial soft tissue appearance of the present case was not markedly changed after OVD was increased by 2 mm. The patient was well adapted to the increased OVD and showed no signs and symptoms of temporomandibular joint disorders in the 3 months with provisional restorations.
In consideration of the level of complexity in the management of oligodontia patients, treatment should begin with early diagnosis to prevent future functional and aesthetic problems. The type of malocclusion, degree of oligodontia, age of patient, and psycho social aspects should aid the clinician in planning and managing the treatment.
| Conclusion | | |
The consequences of missing teeth are numerous and depend on the number and type of teeth missing. Speech, masticatory functional disorders, and aesthetic problems caused by disturbed growth and development of the oro-facial area occur frequently in oligodontia cases. Although oligodontia is mostly considered to be associated with several syndromes, the nonsyndromic aspect of oligodontia should also be taken into consideration. In the management of oligodontia patients, treatment should begin with early diagnosis to prevent future functional and aesthetic problems.
| References | | |
| 1. | Ruf S, Klimas D, Hönemann M, Jabir S. Genetic background of nonsyndromic oligodontia: A systematic review and meta-analysis. J Orofac Orthop 2013;74:295-308.  |
| 2. | Tunç ES, Bayrak S, Koyutürk AE. Dental development in children with mild-to-moderate hypodontia. Am J Orthod Dentofacial Orthop 2011;139:334-8. |
| 3. | Paixão-Côrtes VR, Braga T, Salzano FM, Mundstock K, Mundstock CA, Bortolini MC. PAX9 and MSX1 transcription factor genes in non-syndromic dental agenesis. Arch Oral Biol 2011;56:337-44. |
| 4. | De Coster PJ, Marks LA, Martens LC, Huysseune A. Dental agenesis: Genetic and clinical perspectives. J Oral Pathol Med 2009;38:1-17. |
| 5. | Vieira AR. Genetics of tooth agenesis: How to move the field forward. J Appl Oral Sci 2013;21. |
| 6. | Bergendal B, Klar J, Stecksén-Blicks C, Norderyd J, Dahl N. Isolated oligodontia associated with mutations in EDARADD, AXIN2, MSX1, and PAX9 genes. Am J Med Genet A 2011;155A: 1616-22. |
| 7. | Nordgarden H, Jensen JL, Storhaug K. Reported prevalence of congenitally missing teeth in two Norwegian counties. Community Dent Health 2002;19:258-61. |
| 8. | Gungor AY, Turkkahraman H. Effects of severity and location of nonsyndromic hypodontia on craniofacial morphology. Angle Orthod 2013;83:584-90. |
| 9. | Kotsiomiti E, Kassa D, Kapari D. Oligodontia and associated characteristics: Assessment in view of prosthodontic rehabilitation. Eur J Prosthodont Restor Dent 2007;15:55-60. |
| 10. | Bailleul-Forestier I, Berdal A, Vinckier F, de Ravel T, Fryns JP, Verloes A. The genetic basis of inherited anomalies of the teeth. Part 2: Syndromes with significant dental involvement. Eur J Med Genet 2008;51:383-408. |
| 11. | Prabhu NT, John R, Munshi AK. Rieger's syndrome: A case report. Quintessence Int 1997;28:749-52. |
| 12. | Jumlongras D, Bei M, Stimson JM, Wang WF, DePalma SR, Seidman CE, et al. A nonsense mutation in MSX1 causes Witkop syndrome. Am J Hum Genet 2001;69:67-74. |
| 13. | Gurrieri F, Franco B, Toriello H, Neri G. Oral-facial-digital syndromes: Review and diagnostic guidelines. Am J Med Genet A 2007;143A: 3314-23. |
| 14. | McGovern E, Al-Mudaffer M, McMahon C, Brosnahan D, Fleming P, Reardon W. Oculo-facio-cardio-dental syndrome in a mother and daughter. Int J Oral Maxillofac Surg 2006;35:1060-2. |
| 15. | Minic S, Novotny GE, Trpinac D, Obradovic M. Clinical features of incontinentia pigmenti with emphasis on oral and dental abnormalities. Clin Oral Investig 2006;10:343-7. |
| 16. | Gerits A, Nieminen P, De Muynck S, Carels C. Exclusion of coding region mutations in MSX1, PAX9 and AXIN2 in eight patients with severe oligodontia phenotype. Orthod Craniofac Res 2006;9:129-36. |
| 17. | Fekonja A. Hypodontia in orthodontically treated children. Eur J Orthod 2005;27:457-60. |
| 18. | He X, Shu W, Kang Y, Li Z, Zhang J, Kari K, et al. Esthetic and functional rehabilitation of a patient with nonsyndromic oligodontia: A case report from China. J Esthet Restor Dent 2007;19:137-42. |
| 19. | Boeira BR Jr, Echeverrigaray S. Novel missense mutation in PAX9 gene associated with familial tooth agenesis. J Oral Pathol Med 2013;42:99-105. |
| 20. | Mostowska A, Kobielak A, Trzeciak WH. Molecular basis of non-syndromic tooth agenesis: Mutations of MSX1 and PAX9 reflect their role in patterning human dentition. Eur J Oral Sci 2003;111:365-70. |
| 21. | Gungor AY, Turkkahraman H. Tooth sizes in nonsyndromic hypodontia patients. Angle Orthod 2013;83:16-21. |
| 22. | Wagenberg BD, Spitzer DA. Therapy for a patient with oligodontia: Case report. J Periodontol 2000;71:510-6. |
| 23. | Arte S, Nieminen P, Apajalahti S, Haavikko K, Thesleff I, Pirinen S. Characteristics of incisor-premolar hypodontia in families. J Dent Res 2001;80:1445-50. |
| 24. | Créton MA, Cune MS, Verhoeven W, Meijer GJ. Patterns of missing teeth in a population of oligodontia patients. Int J Prosthodont 2007;20:409-13. |
| 25. | White SN, Zarb GA. Narrative: Case history 1. Int J Prosthodont 2009;22:500-4. |
| 26. | Gross MD, Nissan J, Ormianer Z, Dvori S, Shifman A. The effect of increasing occlusal vertical dimension on face height. Int J Prosthodont 2002;15:353-7. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7]
|











 Search Pubmed for
Search Pubmed for