|
 
 |
| REVIEW ARTICLE |
|
| Year : 2016 | Volume
: 4
| Issue : 1 | Page : 1-6 |
|
Intricate relations and concepts of reference points in prosthodontics: A literature review
Deepti Raghav1, Karan Kapoor1, Abdullah Ali Alqahtani2, Mohammed Zaheer Kola2, Fawaz Alqahtani2
1 Department of Prosthodontics, Shree Bankey Bihari Dental College and Research Centre, Ghaziabad, Uttar Pradesh, India
2 Department of Prosthetic Dental Sciences, College of Dentistry, Prince Sattam Bin Abdulaziz University, Al-Kharj, Kingdom of Saudi Arabia
| Date of Web Publication | 25-May-2016 |
Correspondence Address:
Deepti Raghav
Department of Prosthodontics, Shree Bankey Bihari Dental College and Research Centre, Masuri, Ghaziabad - 201 302, Uttar Pradesh
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2347-4610.182959

Oral rehabilitation presents a variety of clinical situations needing fabrication of prostheses that could satisfy the overall requirement of the patients. In various prosthodontic procedures, exact articulation of the maxillary cast to the articulator necessitates minimum three reference points that could decide the plane to which maxillary cast is mounted. Therefore, the correct choice of reference points in anterior and posterior areas is very crucial failing which one can end up with fabricating intolerable prosthesis. This reference plane is usually created by two points located posterior to the maxillae and one point located anterior to them. In general, the two posterior points are located by measuring prescribed distances from the skin surface landmarks. Literature has well evidenced various anterior and posterior points of reference used for mounting the maxillary cast on the different type of articulator systems. The most common reference plane is the Frankfort plane, which has been assumed to be horizontal when the patient is in the natural head position. However, this relationship is not simply opening or closing, but a complex relationship which exists in three dimensions. Variations may occur in any direction – superoinferior, anteroposterior, or mediolateral. Thus, it is essential to record this relationship with the least possible error to obtain a successful prosthesis. Keywords: Frankfort plane, orbitale, point of reference
How to cite this article:
Raghav D, Kapoor K, Alqahtani AA, Kola MZ, Alqahtani F. Intricate relations and concepts of reference points in prosthodontics: A literature review. Eur J Prosthodont 2016;4:1-6 |
How to cite this URL:
Raghav D, Kapoor K, Alqahtani AA, Kola MZ, Alqahtani F. Intricate relations and concepts of reference points in prosthodontics: A literature review. Eur J Prosthodont [serial online] 2016 [cited 2018 Jun 29];4:1-6. Available from: http://www.eurjprosthodont.org/text.asp?2016/4/1/1/182959 |
| Introduction | |  |
In the fabrication of complete or partial dentures, clinicians frequently require one or more reference planes that could be used in accurate positioning of cast models on an articulator. The articulator, a mechanical device which simulates the movement of the jaw and mutual relations of the teeth during functioning, is essential for diagnostic and therapeutic procedures.[1] Therefore, transfer of a cast of the jaws into the articulator using suitable reference points is deemed necessary. Various opinions have been expressed in literature on the mutual relations of reference planes used in the prosthetic care of patients. The evolution of reference planes was primarily related to the restoration of occlusion in well-controlled form and position of the teeth.[2] The maxillary cast in the articulator usually creates a basic orientation from which all occlusal relationships start, and it should be positioned in space by identifying three points of different orientations, which cannot be on the same line. Most of the planes are formed by two points located posterior to the maxillae and one point located anterior to them. Horizontal plane of reference is plane established on the face of the patient by one anterior reference point and two posterior reference points from which measurements of the posterior anatomic determinants of occlusion and mandibular motion are made.[3] Anterior reference point is the point located on the mid face that, together with two posterior reference points, establishes a reference plane. Whereas posterior reference points are located one on each side of the face in the area of the transverse horizontal axis, which, together with an anterior reference point, establish the horizontal reference plane. Many clinicians have stated that the appropriate selection of a third or posterior point of reference on the Frankfort horizontal plane is essential in prosthetic procedures for esthetic reasons as well as the establishment of a correct plane of occlusion. One study of 21 edentulous patients showed that the relationships of the planes of reference are not maintained in transfer from the patient to the articulator.[4] In another study of 87 dentulous dental students, the variability of the relationship of the planes of reference was described.[5] Keeping all these things in mind, authors have genuinely attempted to review the basic ideology and conceptual applications of different reference points and planes used in routine prosthodontic rehabilitative procedures.
| Scientific Inference of Various Reference Points and Planes | | |
A face-bow is used to transfer the spatial relationship of cranium base to the articulator, usually by relating it to a plane of reference. The most common reference plane is the Frankfort plane (FP), which has been assumed to be horizontal when the patient is in the natural head position. The axis-orbitale plane (AOP) has also been considered horizontal and used as a reference.[6] However, some studies have shown that these planes are not horizontal, and mounting a maxillary cast according to these planes can result in an inaccurate mounting and even end up in incorrect centric relation. The criteria used in the selection of these reference points have been ease of location, convenience, and reproducibility. In general, two points are positioned in the area of the temporomandibular joints (TMJ) and a third or posterior point is selected, anterior to the TMJs, to define a plane of reference, which is oriented in the articulator so that the three-dimensional (3D) position of the upper cast is reproduced as it is in the patient.[7],[8] Ellis suggested that proper mounting of the maxillary cast can be achieved when two relationships are established: (1) The distance of the maxillary arch from the intercondylar hinge axis. (2) the 3D relationship between the maxillary occlusal plane and the skull.[9] A plane of reference which has been used to record the angular relationship between the condylar path and the occlusal plane relationship is FP. Hence, the FP is marked over the lateral cephalometric radiograph by joining of the lowest point in the margin of the left and right bony orbit (orbitale) and the highest point in the margin of the right or left bony auditory meatus (porion).[6],[10],[11],[12]
In 1906, the International Agreement for the Unification of Craniometric and Cephalometric Measurement in Monaco further defined the FP as horizontal. This concept is so widely accepted that the glossary of prosthodontic terms-7 also defines the FP as horizontal.[13] Since the porion point is not reproducible on the articulator, manufacturers of articulators substituted the axis for porion. In this way, &##8220;the AOP was assumed to coincide with the FP.” Thus, the misconception was created that parallelism exists among the FP, the AOP, and the upper member of the articulator (when the incisal pin is set at zero).[14] The selection of the anterior and posterior point of reference determines which plane in the head will become the plane of reference when the prosthesis is being fabricated. When three points are used, the position can be repeated so that different maxillary casts of the same patient can be positioned in the articulator in the same relative position to the end-controlling guidance. It also authenticates the level at which the casts are mounted.[10],[15],[16],[17],[18]
| Different Reference Points | | |
Selection of perfect anterior and posterior reference point is a really crucial step in maxillofacial rehabilitation procedures. Comprehensive understanding of all these points is required for their logical clinical applications [Figure 1] and [Table 2].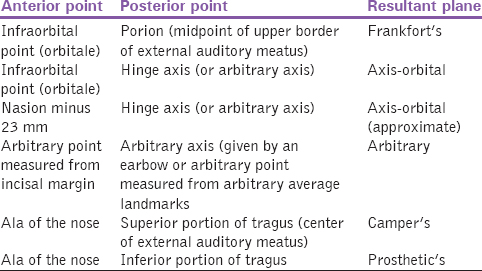 | Table 2: Anterior and posterior points of references and their resulting reference plane
Click here to view |
| Anterior Points of Reference | | |
Orbitale
The recommended anterior reference point is orbitale for mounting casts in a Hanau Wide Vue (Teledyne Water Pik, Fort Collins, Colorado, USA) semi-adjustable articulator. Whenever Hanau Spring Bow (Teledyne Water Pik, Fort Collins, Colorado, USA) is used, it is generally being located by Hanau face-bow with the help of an orbital pointer whereas it is actually the lowest point of the infraorbital rim of the skull, which can be palpated on the patient through the overlying tissues and the skin. One orbitale and the two posterior points that determine the horizontal axis of rotation will define the axis – orbital plane.[19] In a patient, it can be palpated through the overlying tissue and the skin. Orbitale and the two posterior landmarks defining the plane are transferred from the patient to the articulator with the face-bow. The articulator must have an orbital indicator guide. The earlier Hanau articulators had different anterior points of references marked on the incisal guide pin at the levels 30 mm, 37 mm, and 51 mm below the condylar plane. Lauciello and Appelbaum suggested a new incisal notch situated 47 mm below the condylar plane (54 mm below the orbital plane). The presence of many markings on the incisal guide pin would put the practitioner in confusion as to which one should be used and when. The Hanau Wide Vue articulator is provided with two incisal notches at the levels of 37 mm and 54 mm from the orbital plane. The 37 mm incisal notch orients the maxillary cast based on Balkwell's triangle and the 54 mm incisal notch orients the maxillary cast in an average position.[20]
Orbitale minus 7 mm
Bailey and Nowlin have used Hanau model 130–28 articulator and concluded that neither the orbitale nor the incisal notch on the incisal guide pin when used as anterior reference point could accurately transfer the relationship of maxillary plane to the Frankfort horizontal plane. The authors have used Hanau model 130–28 articulator.[21],[22] Gonzalez and Kingery found that the relationships of the planes of reference are not maintained during the transfer from the patient to the articulator and suggested using an anterior point of reference 7 mm below the orbitale. However, the 7 mm difference between the orbital plane and the condylar plane is being compensated in the Hanau Arcon H2 and Hanau Wide Vue articulators. [4] Lauciello and Appelbaum recommended using orbitale as an anterior point of reference and then adjusting the pointer 7 mm above the condylar plane as the most accurate method for anatomically orienting the maxillary cast to an articulator. However, the orbital plane in the Hanau Wide Vue articulator is situated 7 mm above the condylar plane.[20] Later on, Bergstrom developed Arcon articulator that automatically compensates for this error by placing the orbital index 7 mm higher than the condylar horizontal axis.
Nasion minus 23 mm
Nasion is the deepest part of the midline depression just below the level of eyebrows. The nasion guide, or positioner, or relator of the Quick Mount face-bow (Whip-Mix Corporation, United States of America), which is specially designed to be used with the Whip-Mix articulator (Whip-Mix Corporation, United States of America), fits into this depression. The nasion guide of the Quick Mount face-bow used in Whip-Mix articulator fits into this depression.[23] This guide can be moved in and out but not up and down, from its attachment to the face-bow crossbar. The crossbar is located 23 mm below the midpoint of the nasion positioner. When the face-bow is positioned anteriorly by the nasion relator, the crossbar will be in the approximate region of orbitale. The face-bow crossbar and not the nasion relator is the actual anterior reference point locator. While doing the face-bow transfer, the crossbar of the face-bow supports the upper frame of the Whip-Mix articulator. The inferior surface of the frame is in the same plane as the articulator's hinge points. From this, it can be concluded that the Quick Mount face-bow used with the Whip-Mix articulator employs an approximate axis-orbital plane. Therefore, locating the orbital point with this method is very subjective and depends on the large nasion relator, the morphological features of the nasion notch, and the discrepancy of the nasion-orbitale measurement from 23 mm in the patient.[24],[25]
Incisal edge plus articulator midpoint to articulator axis - horizontal plane distance
Accurate positioning of the master casts in the articulator would be the one which would orient the plane of occlusion near the mid-horizontal plane of the articulator. In case of minute error, one can expect the relative position of casts very high or low relative to the instrument's upper and lower arms.[26] Such detrimental effect of these positions could results in mistaken and unclear occlusal relationships. In accordance with this concept, the distance from the articulator's mid-horizontal plane to the articulator's axis-horizontal plane is measured. This same distance is measured above the existing or planed incisal edges on the patient, and its uppermost point is marked as the anterior point of reference on the face. This point can be recorded for future use by measuring vertically downward to it from the inner canthus of the eye and recording this measurement. The inner canthus is used because it is accessible unchanging landmark on the head. It must be documented that this method does not relate the FP or the axis-orbital plane parallel to the horizontal plane.[27]
Alae of the nose
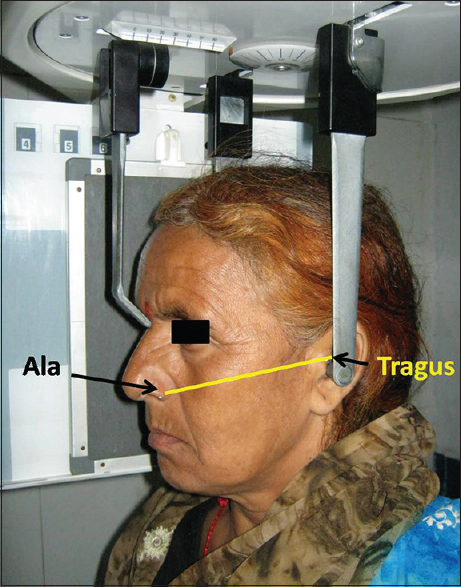
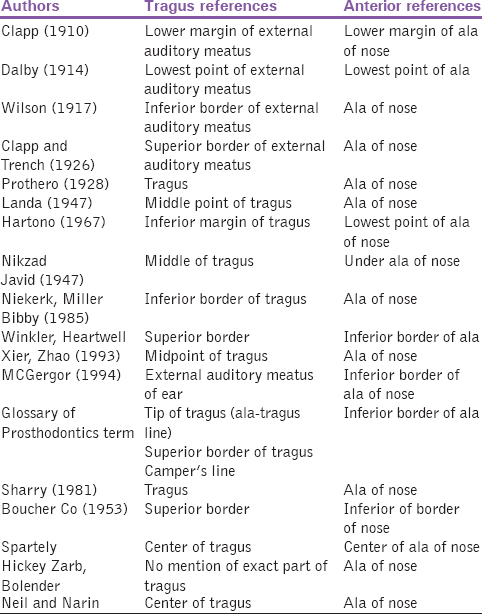
The use of the ala-tragus line (Camper's line) as a guideline has gained popularity since it is easily visualized, thus making the determination of plane of occlusion more convenient. Incomplete denture fabrication procedure, it is very important to make the actual occlusal plane parallel with the horizontal plane [Figure 1].[27] This relationship can be achieved as a line drawn from the ala of the nose to the center of the auditory meatus, i.e., Camper's line. The preferred position for the maxillary incisal edge should be marked on the wax occlusion rim as an initial step in the determination of the occlusal plane. The use of ala-tragus line for the determination of occlusal plane has been a subject of debate over past many years. This is because various researchers cannot come to a consensus as to which tragal reference should be used for the formation of ala-tragal line [Table 1]. In addition, the effect of age on level of the ala-tragal line has not been investigated in the past.[2],[27],[28]
| Posterior Point of Reference | | |
Beyron point
About 13 mm anterior to the posterior margin of the tragus of the ear on a line from the center of tragus extending to the corner of the eye.[1],[29],[30]
Bergstrom's point
About 10 mm anterior to the center of the spherical insert for the external auditory meatus and 7 mm below the Frankfort horizontal plane. Bergstrom point is found to be the most frequently closest to the hinge axis, and Beyron point is the next most accurate posterior point of reference.[3],[19],[30]
Gysi's point
Gysi placed it 11–13 mm anterior to the upper third of the tragus of the ear on a line extending from the upper margin of the external auditory meatus to the outer canthus of the eye.[1],[28],[29],[30]
Lundeen's point
About 13 mm anterior to tragus on line from the base of tragus to outer canthus of eye.[30]
Simpson's point
About 11 mm anterior to the superior border of tragus on Camper's line.[1],[3]
Weinberg's point
About 11–13 mm anterior on a line drawn from the middle and posterior border of tragus.[29],[30]
Abdal-Hadi point
It is based on the high correlation between the width profile of the face and X co-ordinate of the kinematic point. Y = 9.5 + 0.95 (X), a constant distance equal to 0.5 mm was used above the line passing from the center of the external auditory meatus to canthus to locate the superoinferior position.[3],[29]
| Selective Approach for Reference Points and Planes: Clinical Viewpoints | | |
The dentist should thoroughly understand the concept of the reference points and how it could be chosen to achieve the treatment objectives. Both dentist and student should be meticulously familiar with the difficulties that arise if the choice and the use of the anterior reference point are not well co-ordinated with all individuals taking part in fabricating the prosthesis.[14] Nevertheless, right selection of the reference points for a particular case is deemed necessary as most of the prosthetic procedures would be determined accordingly. One should be very thorough about the basic ideology of reference points which is obviously nothing but achieving a natural appearance in the form and the position of the anterior teeth [Figure 2]. When this reference plane is used, the teeth will be viewed as though the patient was standing in a normal postural position with the eyes looking straight ahead. One of the very common problems occur between the dentist and the laboratory technicians when they apply different objectives to the same patient.[15] The dentist is most frequently concerned with selecting the posterior two of the three reference points. In addition, the dentist will either consciously or unknowingly select of these points of reference. This decision will affect the development of occlusion and esthetics for sure.[31],[32] The dentist and the auxiliaries must share a common objective in using an anterior point of reference.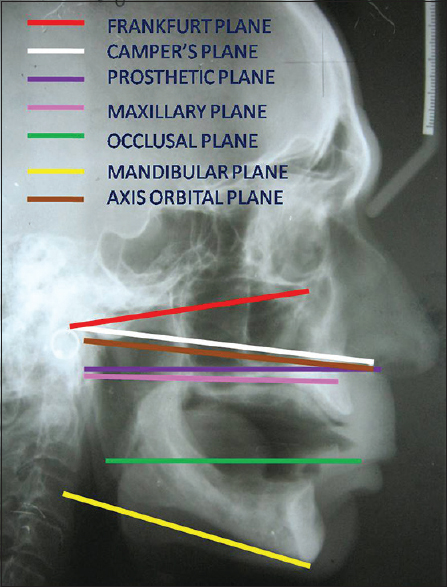 | Figure 2: Various anatomic reference planes marked over the lateral cephalogram
Click here to view |
| Conclusive Remarks | | |
In complete denture fabrication, the prosthodontist is responsible for rehabilitating natural form and function and for developing an occlusion that is most compatible to the craniofacial structures and neuromuscular mechanism. One of the greatest challenges in prosthetic rehabilitation of edentulous patient is to accurately establish the lost occlusal plane. Furthermore, the re-establishment of the lost occlusal plane is very subjective, and it is widely variable depending upon the uncertainty of reference landmarks and the individual judgment. Therefore, it can be commendable that positioning the occlusal plane in the articulator space parallel to the superior and inferior member of the articulator when they are parallel to the Frankfurt plane, is invalid. Therefore, if the occlusal plane is not parallel to the Frankfurt plane, it will decrease the anteroposterior inclination of the upper model and can affect the position of the maxillary anterior teeth. In addition, the occlusal plane will be lowered in the posterior portion, which may harm not only the esthetics of the denture, but also the overall masticatory efficiency of the patient.
Declaration of Patient Consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Zarb GA, Bolender CL. Prosthodontic Treatment for Edentulous Patients: Complete Dentures and Implant-Supported Prostheses. 12 th ed. St. Louis: Mosby; 2004. p. 262.  |
| 2. | Weisgold AS. Occlusion in dental curriculum. J Prosthet Dent 1962;49:419. |
| 3. | Rahn AO, Heartwell CM. Textbook of Complete Denture. 5 th ed. Philadelphia: Lea & Febiger; 2002. p. 270. |
| 4. | Gonzalez JB, Kingery RH. Evaluation of planes of reference for orienting maxillary casts on articulators. J Am Dent Assoc 1968;76:329. |
| 5. | Olsson A, Posselt U. Relationship of various skull reference lines. J Prosthet Dent 1961;11:1045. |
| 6. | Weinberg IA. An evaluation of the face-bow mounting. J Prosthet Dent 1961;11:32. |
| 7. | Foster TD, Howat AP, Naish PJ. Variation in cephalometric reference lines. Br J Orthod 1981;8:183-7. |
| 8. | Page HL. The cranial plane. Dent Dig 1955;61:152. |
| 9. | Ellis E 3 rd, Tharanon W, Gambrell K. Accuracy of face-bow transfer: Effect on surgical prediction and postsurgical result. J Oral Maxillofac Surg 1992;50:562-7. |
| 10. | dos Santos Júnior J, Nelson SJ, Nummikoski P. Geometric analysis of occlusal plane orientation using simulated ear-rod facebow transfer. J Prosthodont 1996;5:172-81. |
| 11. | Olsson A, Posselt U. Relationship of various skull reference lines. J Prosthet Dent 1961;11:1045-9. |
| 12. | Brandrup-Wognsen T. Face-bow, its significance and application. J Prosthet Dent 1953;3:618-30. |
| 13. | Academy of Prosthodontics. Glossary of prosthodontic terms. J Prosthet Dent 1999;81:41-112. |
| 14. | Pitchford JH. A reevaluation of the axis-orbital plane and the use of orbitale in a facebow transfer record. J Prosthet Dent 1991;66:349-55. |
| 15. | Hanau RL. Articulation defined, analyzed and formulated. J Am Dent Assoc 1926;13:1694-707. |
| 16. | de Freitas A. A comparison of the radiographic and prosthetic measurement of the sagittal path movement of the mandibular condyle. Oral Surg Oral Med Oral Pathol 1970;30:631-8. |
| 17. | Bjerin R. A comparison between the Franklorr horizontal and the Sella Turcica-Nasion as reference planes in cephalometric analysis. Acta Odontol Scand 1957;1:15. |
| 18. | Solow B, Tallgren A. Natural head position in standing subjects. Acta Odontol Scand 1971;29:591-607. |
| 19. | Kumar JS, Gupta G, Bansal S, Gupta P. Variability and validity of the anterior point of reference – A cephalometric study. Baba Farid Univ Dent J 2011;2:107-11. |
| 20. | Lauciello FR, Appelbaum M. Anatomic comparison to arbitrary reference notch on Hanau articulators. J Prosthet Dent 1978;40:676-81. |
| 21. | Bailey JO Jr., Nowlin TP. Evaluation of the third point of reference for mounting maxillary casts on the Hanau articulator. J Prosthet Dent 1984;51:199-201. |
| 22. | Winkler S. Essentials of Complete Denture Prosthodontics. 2 nd ed. St. Louis: Elsevier; 2000. p. 156-66. |
| 23. | Hartono R. The occlusal plane in relation to facial types. J Prosthet Dent 1967;17:549-58. |
| 24. | Kaul HO. The effect of anterio-posterior inclination of the occlusal plane on biting force. J Prosthet Dent 1979;42:497-501. |
| 25. | Leitão P, Nanda RS. Relationship of natural head position to craniofacial morphology. Am J Orthod Dentofacial Orthop 2000;117:406-17. |
| 26. | Aldridge K, Boyadjiev SA, Capone GT, DeLeon VB, Richtsmeier JT. Precision and error of three-dimensional phenotypic measures acquired from 3dMD photogrammetric images. Am J Med Genet A 2005;138A: 247-53. |
| 27. | Singh G. Ala tragus line – A cephalometric evaluation. Int J Prosthet Dent 2010;1:11-5. |
| 28. | Soloman FG, Shetty SN. Reliability of tragus morphology and it's reference to establish Camper's plane. J Indian Prosthodont Soc 2000;11:16-22. |
| 29. | Ercoli C, Graser GN, Tallents RH, Galindo D. Face-bow record without a third point of reference: Theoretical considerations and an alternative technique. J Prosthet Dent 1999;82:237-41. |
| 30. | Wilkie ND. The anterior point of reference. J Prosthet Dent 1979;41:488-96. |
| 31. | Lauritzen AG, Wolford LW. Hinge axis location on an experimental basis. J Prosthet Dent 1961;11:1059-67. |
| 32. | Beck HO. A clinical evaluation of the arcon concept of articulation. J Prosthet Dent 1959;9:409. |
[Figure 1], [Figure 2]
[Table 1], [Table 2]
|









 Search Pubmed for
Search Pubmed for