|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2016 | Volume
: 4
| Issue : 1 | Page : 12-16 |
|
An in vivo study to compare and correlate sagittal condylar guidance obtained by radiographic and extraoral gothic arch tracing method in edentulous patients
V Vinutha Kumari, Gouri V Anehosur, Roseline Meshramkar, Ramesh K Nadiger, K Lekha
Department of Prosthodontics, SDM College of Dental Sciences and Hospital, Dharwad, Karnataka, India
| Date of Web Publication | 25-May-2016 |
Correspondence Address:
Gouri V Anehosur
Department of Prosthodontics, SDM College of Dental Sciences and Hospital, Dharwad - 580 009, Karnataka
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2347-4610.182961

Purpose: To compare the sagittal condylar guidance angle obtained by extra oral gothic arch tracing and orthopantomogram in completely edentulous subjects. Material and Methods: Ten completely edentulous subjects were selected by the inclusion and exclusion criteria. Conventional steps in the fabrication of complete denture with balanced occlusion were carried out. Extra oral gothic arch tracing records were obtained for every patient. Protrusive interocclusal records were used to program the Hanau wide vue semiadjustable articulator, thus obtaining the sagittal condylar guidance angle by clinical method. On the orthopantomogram obtained for every patient in the study, orbitale and porion were located and the Frankfurts horizontal reference line was drawn. The most superior and the inferior points on the glenoid fossa curvature were located and a mean curvature line was obtained. A third reference line passing through the most superior and the inferior points on the glenoid fossa was extended to intersect the Frankfurts horizontal plane, thus obtaining the radiographic sagittal condylar guidance. These values were tabulated and subjected to Wilcoxon Signed Ranks test. Results: There is statistically significant difference between the sagittal condylar guidance values obtained between right and left sides with extra oral gothic arch tracing and orthopantomographic method (p value is 0.014 and 0.007 respectively). Conclusions: The use of orthopantomogram to set the condylar guidance on the semi adjustable articulator for complete denture therapy is questionable. Keywords: Completely edentulous, condylar guidance registration, Hanau Wide Vue articulator, panoramic radiograph, radiographic articular eminence
How to cite this article:
Kumari V V, Anehosur GV, Meshramkar R, Nadiger RK, Lekha K. An in vivo study to compare and correlate sagittal condylar guidance obtained by radiographic and extraoral gothic arch tracing method in edentulous patients. Eur J Prosthodont 2016;4:12-6 |
How to cite this URL:
Kumari V V, Anehosur GV, Meshramkar R, Nadiger RK, Lekha K. An in vivo study to compare and correlate sagittal condylar guidance obtained by radiographic and extraoral gothic arch tracing method in edentulous patients. Eur J Prosthodont [serial online] 2016 [cited 2018 Jun 29];4:12-6. Available from: http://www.eurjprosthodont.org/text.asp?2016/4/1/12/182961 |
| Introduction | |  |
For a successful treatment outcome, a prosthesis has to be in harmony with the patient's stomatognathic system.[1],[2] In edentulous subjects, this is possible when the articulator is programmed according to the patient's condylar guidance to simulate the mandibular movements, hence developing an occlusion in harmony with health and function of the stomatognathic system.[3],[4],[5] Occlusal interferences are unavoidable during mandibular movements if the condylar guidance is not recorded accurately, therefore increasing the chairside denture adjustment time.[6]
Condylar guidance can be recorded clinically by various intra- and extra-oral methods.[6],[7],[8],[9] However, graphic registering technique is recommended to verify the centric relation and to record the condylar guidance.[9] Gothic arch tracings and interocclusal records are commonly adopted in clinical practice.[9] Several studies have shown these methods to be unreliable due to inconsistency of the recordings in consecutive registrations, between operators and between materials.[7],[10],[11],[12],[13],[14] Hence, there has always been a need for an accurate method to record condylar guidance.
Other than clinical methods, literature indicates the use of radiographic techniques as they involve stable bony landmarks and can be standardized.[6],[11] Various radiographic techniques used are lateral cephalograms, orthopantomograms (OPGs), and tomographs.[1] OPG is the routinely obtained diagnostic aid with least radiation exposure. It is also preferred over computed tomography for recording the condylar guidance.[15] Various studies have been conducted to find if any correlation exists between clinically recorded sagittal condylar guidance (SCG) values and the one traced on radiographs. However, these studies were primarily done on dentulous subjects.[6],[16],[17] Moreover, there is a relative lack of literature in finding if this correlation exists in edentulous patients.
Thus, the study was designed to compare the SCG angle obtained by extraoral gothic arch tracing records to the SCG angle measured on OPG in edentulous subjects. Thus, the objectives were to compare the SCG angulations (on left and right sides) obtained from extraoral gothic arch tracing records and OPG in edentulous patients.
| Materials and Methods | | |
Ethical clearance was taken by the Institutional Review Board and informed consent was obtained from the patients. Ten completely edentulous patients of either sex were selected according to the inclusion and exclusion criteria [Table 1].
Clinical method
Conventional steps in the fabrication of complete dentures with balanced occlusion were carried out. Wax occlusal record rims were fabricated to record the jaw relation. Combinations of mechanical and physiological methods were used to record the vertical jaw relation. Hanau Wide Vue semi-adjustable articulator along with Hanau ™ Springbow (Whip Mix Corporation, USA) was used in the study. Facebow registrations were accomplished using the standard technique.[18] Maxillary and mandibular casts were secured onto the articulator using the centric interocclusal record. A set of height extraoral tracers were attached to each record rims on the articulator. The patient was trained to give extraoral gothic arch tracings. Intraoral centric and protrusive records approximately 6 mm from centric were made with Registrado X-tra, addition silicone (VOCO GmbH, Cuxhaven, Germany) for bite registration.
The protrusive records were used to program the articulator. The centric locks and the horizontal inclination of the condylar guidance on the articulator were loosened. The incisal pin was raised to remove the possibility of mechanical interference with the incisal guide. The protrusive interocclusal relation record was seated onto the lower occlusal rim. The upper member was carefully guided into protrusion, lightly engaging into the imprint of the protrusive relation record. The right and left condylar guidance were rotated back and forth to accurately seat the upper and lower rims into the protrusive relation record. Making sure that the occlusion rims seated without rocking in or deforming the record, the thumb-nuts for horizontal inclination were tightened. The protrusive relation record was then removed. Thus, horizontal condylar inclinations on both sides of the articulator were set. The right and left SCG value on articulator were tabulated for all the 10 patients. This entire procedure was carried out by the same operator for all patients.
Radiographic method
An OPG was made for every patient. All radiographs were made by the same operator using the same radiographic unit. The radiographic unit comes with a beam of light aligned along the anatomic planes, and a cephalostat was used to align the head in the same position for all patients. The images were acquired at 74 kVp and 10 mA. The landmarks were traced using the guidelines as given by Gilboa et al.[11] Clear acetate sheets were overlapped on OPG and tracings were done manually as shown in [Figure 1]. The left and right &##8220;orbitale” (lowest point on the margin of the orbit - O) and &##8220;porion” (highest point on the margin of the auditory meatus - P) were identified and the Frankfurt's horizontal plane (O-P) was drawn by joining the two landmarks on both the left and right side. The most superior and most inferior point on the glenoid fossa curvature (A and B. respectively) were identified and mean curvature line was obtained by joining the two points. A third reference line passing through the same points was extended to intersect the Frankfurt's horizontal plane to obtain radiographic SCG angle. The data recordings comprised two sets of values for 10 patients, i.e., the SCG obtained by programming the Hanau Wide Vue articulator by extraoral gothic arch tracing records and the SCG obtained from tracings on the OPG [Table 2].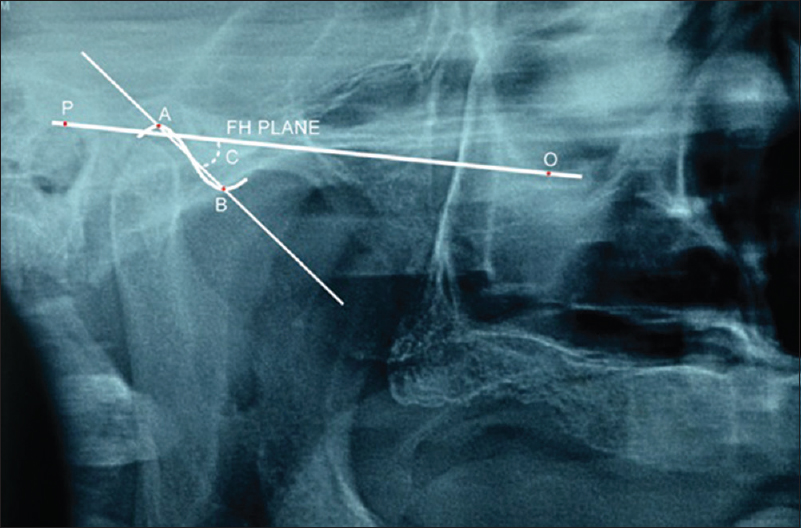 | Figure 1: Tracing on the right temporomandibular joint of the orthopantomogram to obtain the sagittal condylar guidance angle radiographically
Click here to view |
 | Table 2: The condylar guidance angles obtained by extraoral gothic arch tracing and orthopantomogram were tabulated and the mean angle was derived
Click here to view |
The results obtained were subjected to statistical analysis using SPSS 10 software (Statistical Package for the Social Sciences, IBM Software Group, USA). Test of significance was carried out by Wilcoxon signed ranks test to determine the difference between the condylar guidance by two methods. It revealed a significant difference between the SCG values obtained by OPG and extraoral gothic arch tracing since P = 0.014 and 0.007 for the two methods, respectively.
| Results | | |
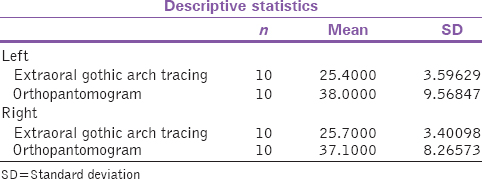
[Table 3] shows the condylar guidance values and standard deviations measured by the radiographic and gothic arch tracing methods. [Table 4] shows the correlation between the condylar guidance values measured by gothic arch tracing method and OPG method. The radiographic values were on an average 13° greater than the values obtained by gothic arch tracing method.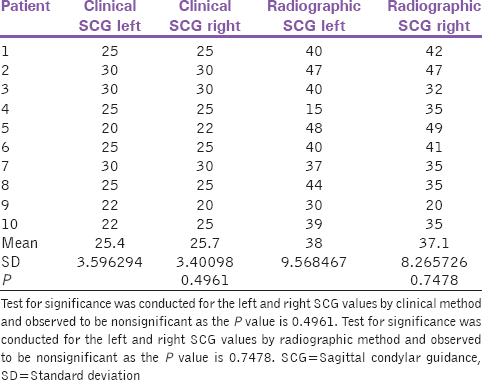 | Table 3: The sagittal condylar guidance values of left and right sides obtained by clinical method and radiographic method
Click here to view |
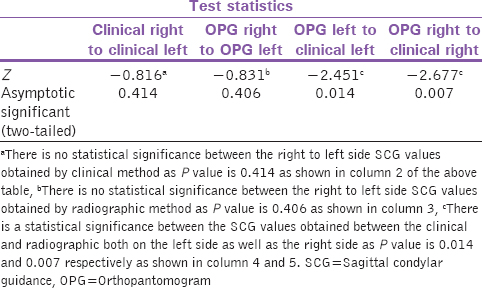
[Table 4] shows that there is no statistical significance between the right to left side SCG values obtained by clinical method as the P value is 0.414 as shown in column 2. SCG values obtained by radiographic method also show no statistical significance between the right to left side as the P value is 0.406 as shown in column 3.
[Table 4] shows that there is a statistical significance between the SCG values obtained between the extraoral gothic arch tracing method and radiographic method, both on the left side as well as the right side as the P value is 0.014 and 0.007 as shown in column 4 and 5, respectively.
| Discussion | | |
An OPG provides a comprehensive view of the entire maxillomandibular region and adjoining areas on a single film. Image magnification and distortion limit the accuracy in OPG. White and Pharaoh, Langland et al., and Stramotas et al. suggested that if the degree of magnification was the same, both horizontally and vertically in the central plane of the focal trough, all structures would be in focus on the final radiograph.[19],[20],[21]
The temporal region in the OPG shows two distinct radiopaque lines. These lines which often intersect can be confusing due to inherent inaccuracies and limitations in the OPG and combined with parallax errors in patient head positioning.[19],[20],[21]
In this study, the OPG machine used is equipped with a cephalostat and therefore accurately placing the patient's head. The articular eminence inclination in the OPG image was traced from the most superior to the most inferior points of curvature and was recorded as SCG angle.
Clinically significant range of protrusion is approximately 4–6 mm to set condylar guidance.[7],[22] Several investigators have found variations in SCG angles ranging between 5 degrees to 55 degrees, owing to this great variation many clinicians use average condyle guide setting.[4], 8, [22],[23],[24],[25],[26] The SCG values obtained from OPG were greater than those obtained from clinical methods. The results indicate that the clinical methods exhibit statistically significant difference with radiographic technique. Christensen and Slabbert and Brewka in their studies have concluded that radiographically obtained SCG always has a greater mean value than intraoral/clinical technique.[12],[27] The low degree of association between radiographic and clinical method can be attributed to the 6 mm protrusion in the tracer method. SCG changes with the degree of protrusion [28] and clinical methods represent only one point along the condyle path.[4]
It can be inferred from the present study that the SCG obtained by clinical/gothic arch tracing technique is not comparable with that obtained radiographically. At the same time, it is important to note the increased precision and chemomechanical properties of the present day technique and materials and apply computerized tomographic methods of measuring condylar determinants to clinical work. However, the clinical methods have proven to be more practical and economical.[6] At the same time, on the basis of the results of this pilot study, it is not justified to omit the use of radiographic techniques.
Hanau Wide Vue semi-adjustable articulator was used to receive the intraoral records obtained from extraoral gothic arch tracing. Fixed intercondylar distances and the straight condylar pathways limit the capability of the articulator to accurately simulate the temporomandibular joints and their movements, leading to errors in horizontal and frontal plane.[29] Arbitrary hinge axis is being used to transfer the facebow record to the articulator. This may be the reason for the difference in radiographic and clinical technique.
As a pilot study, the sample size was small and therefore a long-term clinical study with more sample size is required to verify the results. Radiographic error exists despite standardization. The extraoral tracing method, though better among the lot, has some disadvantages. Computerized electronic axiographs are thought to be superior to the conventional methods for determination of condylar guidance. However, knowledge about their clinical use is limited. Therefore, they have to be researched upon.
| Conclusions | | |
Within the limitations of the study, it was concluded that a definite difference was found between the condylar guidance values obtained by the OPG and the most commonly used extraoral gothic arch tracing method in edentulous patients. Hence, the use of OPG to set the condylar guidance on the articulator is questionable in edentulous patients. Clinical studies to evaluate patient comfort and long-term effects of complete denture therapy using SCG by clinical and radiographic technique on stomatognathic system need to be evaluated.
Acknowledgments
We would like to thank the staff and postgraduate students in the Department of Oral Radiology for their support.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Shah RJ, Agarwal P, Negi P. A comparative analysis of sagittal condylar guidance determined by two articulator systems and orthopantomographs (OPG) in completely edentulous patients. Indian J Dent Sci 2013;4:72-6.  |
| 2. | Tejo SK, Kumar AG, Kattimani VS, Desai PD, Nalla S, Chaitanya KK. A comparative evaluation of dimensional stability of three types of interocclusal recording materials-an in vitro multi-centre study. Head Face Med 2012 5;8:27. |
| 3. | Thakur M, Jain V, Parkash H, Kumar P. A comparative evaluation of static and functional methods for recording centric relation and condylar guidance: A clinical study. J Indian Prosthodont Soc 2012;12:175-81. |
| 4. | Donegan SJ, Christensen LV. Sagittal condylar guidance as determined by protrusion records and wear facets of teeth. J Prosthet Dent 1991;45:469-72. |
| 5. | Celenza FV. An analysis of articulators. Dent Clin North Am 1979;23:305-26. |
| 6. | Shreshta P, Jain V, Bhalla A, Pruthi G. A comparative study to measure the condylar guidance by the radiographic and clinical methods. J Adv Prosthodont 2012;4:153-7. |
| 7. | dos Santos J Jr., Nelson S, Nowlin T. Comparison of condylar guidance setting obtained from a wax record versus an extraoral tracing: A pilot study. J Prosthet Dent 2003;89:54-9. |
| 8. | Preti G, Scotti R, Bruscagin C, Carossa S. A clinical study of graphic registration of the condylar path inclination. J Prosthet Dent 1982;48:461-6. |
| 9. | Zarb GA, Bolender CL. Prosthodontic Treatment For Edentulous Patients: Complete Dentures And Implant-Supported Prostheses. 12 th ed. St Louis: Mosby; 2004. p. 294. |
| 10. | Sharma LA, Azhagarasan NS, Shankar C, Sharma A. A comparative study of the effect of three different interocclusal recording materials on reproducibility of horizontal condylar registrations in two different semiadjustable articulators: A clinical study. Int J Prosthodont Rest Dent 2011;1:155-62. |
| 11. | Gilboa I, Cardash HS, Kaffe I, Gross MD. Condylar guidance: Correlation between articular morphology and panoramic radiographic images in dry human skulls. J Prosthet Dent 2008;99:477-82. |
| 12. | Christensen LV, Slabbert JC. The concept of the sagittal condylar guidance: Biological fact or fallacy? J Oral Rehabil 1978;5:1-7. |
| 13. | Gross M, Nemcovsky C, Friedlander LD. Comparative study of condylar settings of three semiadjustable articulators. Int J Prosthodont 1990;3:135-41. |
| 14. | Gross M, Nemcovsky C, Tabibian Y, Gazit E. The effect of three different recording materials on the reproducibility of condylar guidance registrations in three semi-adjustable articulators. J Oral Rehabil 1998;25:204-8. |
| 15. | Prashanti E. Comparison of condylar guidance angulations obtained from protrusive records, orthopantomographic tracings, and 3-dimensional computed tomographic tracings in edentulous subjects- an in-vivo study. Int Poster J Dent Oral Med 2014;16:Nr.1 Poster 745. |
| 16. | Tannamala PK, Pulagam M, Pottem SR, Swapna B. Condylar guidance: Correlation between protrusive interocclusal record and panoramic radiographic image: A pilot study. J Prosthodont 2012;21:181-4. |
| 17. | Prasad KD, Shah N, Hegde C. A clinico-radiographic analysis of sagittal condylar guidance determined by protrusive interocclusal registration and panoramic radiographic images in humans. Contemp Clin Dent 2012;3:383-7. [ PUBMED]  |
| 18. | Hanau wide vue arcon articulators and wide vue II articulators. Illustrated instruction manual. Whipmix corporation, 2008. p.16. |
| 19. | White SC, Pharaoh MJ. Oral Radiology: Principles and Interpretation. 6 th ed. St. Louis: Mosby; 2008. p. 175-7. |
| 20. | Langland OE, Langlais RP, Preece JW. Principles of Dental Imaging. 2 nd ed. Philadelphia: Lippincott Williams & Wilkins; 2002. p. 202. |
| 21. | Stramotas S, Geenty JP, Petocz P, Darendeliler MA. Accuracy of linear and angular measurements on panoramic radiographs taken at various positions in vitro. Eur J Orthod 2002;24:43-52. |
| 22. | Mohl ND, Zarb GA, Carlsson GE: A Textbook of Occlusion. Chicago, Quintessence, 1988. p. 139-40. |
| 23. | Zamacona JM, Otaduy E, Aranda E. Study of the sagittal condylar path in edentulous patients. J Prosthet Dent 1992;68:314-7. |
| 24. | Lundeen HC, Wirth CG. Condylar movement patterns engraved in plastic blocks. J Prosthet Dent 1973;30:866-75. |
| 25. | Woelfel JB, Winter CM, Igarashi T. Five-year cephalometric study of mandibular ridge resorption with different posterior occlusal forms. Part I. Denture construction and initial comparison. J Prosthet Dent 1976;36:602-23. |
| 26. | Hobo S, Mochizuki S. Study of mandibular movements by means of an electronic measuring system. Part II. J Jpn Soc 1982;26:635-53. |
| 27. | Brewka RE. Pantographic evaluation of cephalometric hinge axis. Am J Orthod 1981;79:1-19. |
| 28. | Posselt U, Skytting B. Registration of the condyle path inclination: Variations using the Gysi technique. J Prosthet Dent 1960;10:243-7. |
| 29. | Price RB, Kolling JN, Clayton JA. Effects of changes in articulator settings on generated occlusal tracings. Part I: Condylar inclination and progressive side shift settings. J Prosthet Dent 1991;65:237-43. |
[Figure 1]
[Table 1], [Table 2], [Table 3], [Table 4]
|









 Search Pubmed for
Search Pubmed for