|
 
 |
|
ORIGINAL ARTICLE |
|
|
|
| Year : 2011 | Volume
: 17
| Issue : 3 | Page : 188-193 |
| |
Tracing disease gene(s) in non-syndromic clefts of orofacial region: HLA haplotypic linkage by analyzing the microsatellite markers: MIB, C1_2_5, C1_4_1, and C1_2_A
R Rajendran1, Saleem F Shaikh2, Sukumaran Anil3
1 Department of Oral Medicine and Diagnostic Science, College of Dentistry, King Saud University, Post Box: 60169, Riyadh-11545, Kingdom of Saudi Arabia
2 Department of Human Molecular Genetics, RGCB, Trivandrum 695014, Kerala, India
3 Department of Periodontics and Community Dentistry and Dental Implant and Osseointegration Research Chair, College of Dentistry, King Saud University, Post Box: 60169, Riyadh-11545, Kingdom of Saudi Arabia
| Date of Web Publication | 20-Jan-2012 |
Correspondence Address:
R Rajendran
College of Dentistry, King Saud University, P.O. Box: 60169, Riyadh 11545
Kingdom of Saudi Arabia
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0971-6866.92101

 Abstract Abstract | | |
Background : Cleft lip with or without cleft palate (CL/P) is the most frequent craniofacial malformation seen in man. The etiology of CL/P is complex involving both genetic and epigenetic (environmental) factors, and the genes play an almost deterministic role in the normal development of craniofacial structures. This study was aimed at ascertaining the association of HLA microsatellites in CL/P patients.
Materials and Methods : Case DNA was obtained from 76 patients (40M and 36 F, average age 7.8 years, range 1-16 years). Unaffected individuals from the same geographical area without population mixing included as controls (n=154, 76 M and 78 F, average age 8.2 years, range 2-17 years). All DNA samples were purified from peripheral blood by standard techniques.
Results :0 Four microsatellites were compared in this case-control study. C1_2_5 locus was the most polymorphic marker with 15 observed alleles while C1_4_1 had the least number of alleles. Three of the four markers viz MIB,C1_4_1 and C1_2_5 showed a significant association of microsatellite alleles with CL/P. Five alleles (MIB_326,332,350; C1_4_1 - 213 and C1_2_5-204) were seen with an increased frequency among the test samples, whereas two alleles (C1-4_1_217, and C1_2_5_196) had an increased frequency among the control samples. One allele (C1-4-1-209) had an increased frequency in patient group but was not observed in the controls.
Conclusion : The role of HLA complex in the pathogenesis of CL/P is speculative and has not been established so far. The result of this study shows that a few alleles have an increased frequency of expression in the diseased group which suggests that these alleles may predispose the individuals to clefting. This finding may be beneficial to aid in early diagnosis and plan intervention strategies.
Keywords: Cleft lip, cleft palate, inheritance, nonsyndromic cleft, orofacial cleft
How to cite this article:
Rajendran R, Shaikh SF, Anil S. Tracing disease gene(s) in non-syndromic clefts of orofacial region: HLA haplotypic linkage by analyzing the microsatellite markers: MIB, C1_2_5, C1_4_1, and C1_2_A. Indian J Hum Genet 2011;17:188-93 |
How to cite this URL:
Rajendran R, Shaikh SF, Anil S. Tracing disease gene(s) in non-syndromic clefts of orofacial region: HLA haplotypic linkage by analyzing the microsatellite markers: MIB, C1_2_5, C1_4_1, and C1_2_A. Indian J Hum Genet [serial online] 2011 [cited 2016 May 13];17:188-93. Available from: http://www.ijhg.com/text.asp?2011/17/3/188/92101 |
| Introduction | |  |
Craniofacial anomalies (CFA) are a diverse group of deformities in the growth of the head and facial bones. There is no single factor solely responsible for these abnormalities. Instead, there are many factors that may contribute to their development, including combination of genes, environmental factors, and folic acid deficiency. Some of the most common types of craniofacial anomalies include cleft lip and/ or cleft palate (CL/P), cleft lip (CL), cleft palate (CP) and craniosynostosis (premature closure of sutures).
The frequency of occurrence of CL/P has been computed on a global scale and is estimated to be 1 in every 800 new born babies. [1] Accurate data on the frequency of occurrence of these disorders is inherently handicapped by the heterogeneity of oro-facial clefting, lack of standard criteria for collection of data and in particular, the lack of and /or failure to apply an internationally comparable classification for oro-facial clefting.
The study of oro-facial clefts has a rich history in human genetics. One of the first birth defect loci mapped using DNA based polymorphisms was that for the X-linked cleft palate and ankyloglossia mapped by linkage to Xq21-q22. [2] Studies have suggested loci for clefts on chromosomes 2, 4, 6,17 and 19. [3],[4],[5] Only loci on 6p have consistently shown linkage to CL/P. [6],[7],[8] Association studies have also been used to examine candidate genes in CL/P, many genes have been evaluated which include TGF-α, interferon regulatory factor-6(IRF-6), [9] muscle segment homeobox gene (MSX-1), [10],[11] TGF-β3 and retinoic acid receptor- α (RARA). [12] MSX-1 and TGF- β3 are the two strongest candidate genes for cleft lip and palate in humans. [13]
The human leukocyte antigen (HLA) loci are the most polymorphic human proteins, and by virtue of their extreme polymorphism HLA typing can be used to identify a subset of population who are at an increased risk of developing or inheriting a particular disease or anomaly. The MHC region (HLA loci) is saturated with numerous microsatellites that are in linkage disequilibrium with various alleles of the HLA genes. "Microsatellite" is the term used to describe tandem repeats of short sequence motifs, no more than 6 bases long and have been found in every organism investigated so far. Microsatellites are highly polymorphic and are therefore useful genetic markers in studies of disease gene mapping.
Studies on the relationship of HLA haplotype and CL/P are found to be very few especially in the context of people of Indian ethnic extraction. Four microsatellite markers around the HLA class 1 genes were studied for their putative association with non-syndromic CL/P.
| Materials and Methods | | |
Case DNA was obtained from 76 subjects (40 males and 36 females, average age 7.8 years, range 1-16 years) belonged to the state of Kerala, south India with non-syndromic CL/P. Subjects with isolated CP, known teratogenic exposure and other recognized anomalies and /or developmental delay were excluded from this study. Unaffected individuals from the same geographical area without evidence of population mixing, migration and /or ethnic stratification, who have had no craniofacial anomalies or any family history to the effect were enrolled as controls (n=154, male 76 and female 78, average age 8.2 years, range 2-17 years). All DNA samples were purified from peripheral blood by standard techniques [14] after the subjects provided written informed consent and approval was obtained from the institutional "Human Ethical Committee" (HEC).
Sample collection
Peripheral blood samples of volume 10 ml were collected by anti-cubital vein puncture from patients and controls in plastic falcon tubes containing EDTA.
Quantification of DNA
The quality and quantity of genomic DNA was checked using an UV spectrophotometer (Biospec 1601; Shimadzu, Japan). The quality of DNA was checked by taking the ratio of absorbances at 260 nm and 280 nm (260/280) respectively. A ratio between 1.7 and 1.8 indicates good quality DNA without protein contamination. The absorption of 10D (A) is equivalent to approximately 50 ugm/ml of double stranded DNA. The concentration of DNA in 1 ul of DNA sample was calculated using the following equation, absorbance at 260 nm × dilution factor (50) × 1 OD at 260 nm of DNA / 1000.
Polymerase chain reaction was performed to amplify the DNA stocks and to check for the allelic variants. The extracted DNA samples along with the primers for the genes underwent PCR amplification. The sequencing of the PCR product was carried out on agarose gel slice containing the amplified DNA fragments using Flour S TM multi-imager system (Biorad).
HLA microsatellite analysis
Four microsatellites around the HLA class 1 genes were selected to study their association with CL/P. The selected microsatellites were MIB (D6S2810), C1_2_A (D6S2793), C1_2_5 (D6S2811), and C1_4_1 (D6S2927). The loci were amplified using primers labeled with fluorescent dyes. The sense strand primers were labeled with 6-FAM, 6-TET, and 8-HEX dyes at the 5' end while the reverse primers were unlabelled. Amplification was carried out in a total reaction volume of 15 ul containing 50 ng DNA, 2.5 mM dNTPs, 1.5 mM MgCl 2 , 5 units of amplitaq and 10X amplitaq gold buffer.
Primers used for microsatellite analysis
MIB - 6FAM - 5' -CTACCATgACCCCCTTCCCC
5' - CCACAgTCTCTATCAgTCCA
C1_4_1-6FAM - 5' - CgAgAgAACAACTggCAggACTg
5' - gACAgTCCTCATTAgCgCTgAgg
C1_2_5 -6TET - 5' - CAgTAgTAAgCCAgAAgCTATTAC
5' - AAgTCAAgCATATCTgCCATTTgg
C1_2_A - 8 HEX - 5' - AATAgCCATgAgAAgCTATgTgggggAg
5' - CTACCTCCTTgCCAAACTTgCTgTTTgTg
A multiplex PCR was used for the amplification of all four microsatellites simultaneously in one PCR reaction (MJ Research Thermal Cycler-PTC 200). The molecular weights of the reaction products were calculated using the "Applied Biosystems" software, "Gene Scan 3.1".
Statistical analysis
The allele frequencies for the four microsatellites were calculated using SPSS 1.0 software. The individuals in each allele category was compared with that of controls using Fisher's exact 't' test and a 'P' value of less than 0.05 was considered as significant.
| Results | | |
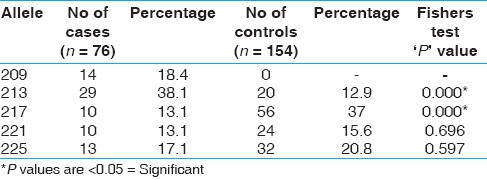
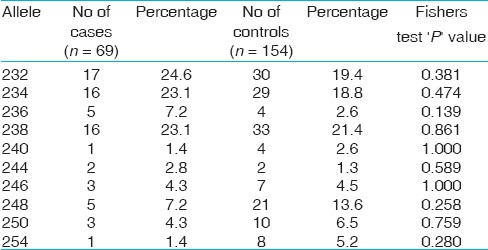
Four microsatellites were compared in this case-control study [Figure 1]. All the four markers were highly polymorphic in the control as well as patient samples. C1_2_5 locus was the most polymorphic marker with 15 observed alleles [Table 1], while C1_4_1 had the least number of alleles [Table 2]. Alleles showing marked differences in frequency between test and control cases were statistically analyzed using Fisher's exact test. A 'P' value of < 0.05 was considered as significant. Three of the four markers namely MIB [Table 3], C1_4_1 and C1 _2_5 showed significant association of microsatellite alleles with cleft lip and palate. Five alleles (MIB - 326,332, 350; C1_4_1 - 213 and C1_2_5 - 204) were seen with a significantly increased frequency among test cases, whereas two alleles (C1_4_1 -217 and C1_2_5 -196) had an increased frequency among the control samples. One allele (C1_4_1 -209) had an increased frequency in the patient group but was not observed in the control samples. None of the alleles in the C1_2_A locus [Table 4] recorded significant comparison.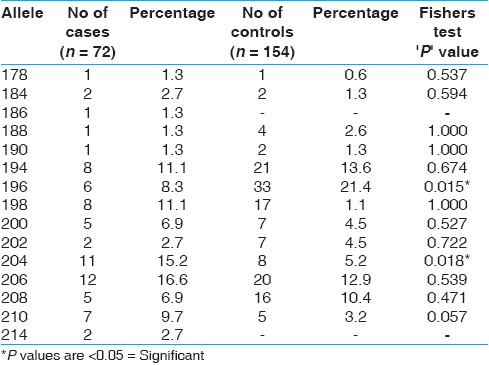 | Table 1: C1_2_5 The microsatellite markers exhibiting polymorphism of allelic frequencies and their percentage distribution among cases and controls is depicted. Alleles showing marked differences in frequency between test and control cases were analyzed using Fisher's extract test.
Click here to view |
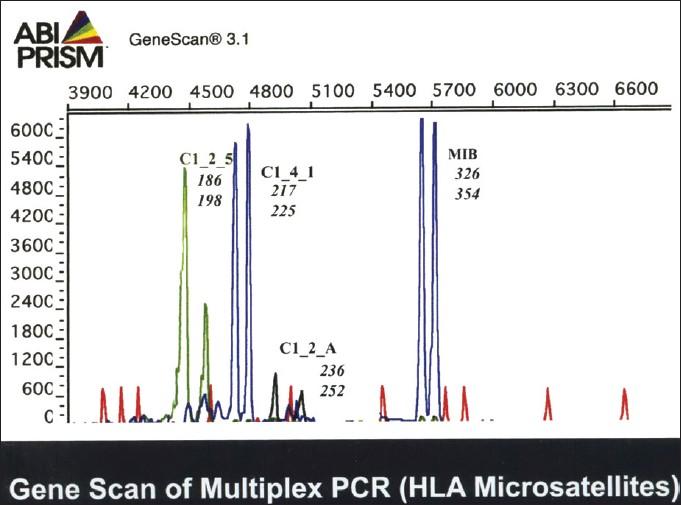 | Figure 1: Gene scan depicting allelic frequencies and extend of polymorphism in the test and control cases.
Click here to view |
| Discussion | | |
Human leukocyte antigens (HLA), also referred to as major histocompatibility complex (MHC) antigens, the genetic loci of which is situated on the short arm of chromosome 6 (6p21). They are membrane bound molecules with a peptide binding domain that interacts with the "T" cell receptor. [15] HLA molecules are divided in to class 1 and 2, which are distinct in structure, function and expression pattern. The class 1 and 2 molecules are the most polymorphic human proteins, some of which have over 400 allelic variants. The HLA gene complex encompasses three constituent regions; in the centromeric end of chromosome 6 is the class 2 loci, while near the telomeric end of the short arm is the class 1 region. Located between the class 1 and 2 regions is the class 3 region containing around 75 genes encoding a variety of proteins. The principal class 1 genes are those coding the α chains of six isoforms of HLA viz A,B,C,E,F and G. In addition, there are HLA- H,J,K,L forms which are non-functional pseudogenes closely related to the functional class 1 genes in nucleotide sequence. Microsatellite markers have facilitated identification of a number of disease genes, depending on the extent of linkage disequilibrium occurring between the disease and marker loci. As the microsatellites are located very close to the putative disease genes, any mutation or polymorphism of the genes would be reflected in these microsatellites as well. It has been predicted that the HLA region microsatellites should maintain a high level of disequilibrium (linkage) with selected MHC alleles, to act as effective markers of disease related HLA loci.
The role of HLA complex in the pathogenesis of non-syndromic CL/P has not been explained well; however, the association has been reported consistently. [16] Wegener et al, [17] reported an increased frequency of HLA-A11, HLA-B35 and HLA-DRw6 in cleft patients as against normal control population. Bonner et al, [18] reported an increased frequency of HLA-A24 and HLA-A28 in caucasian and Mexican American males respectively. Similarly Watanabe et al, [19] performed HLA studies on Japanese patients and reported that the frequency of HLA-Cw7 was significantly higher in that population. However, many studies failed to establish a linkage to HLA in non-syndromic cleft lip and palate patients. [20]
Heredity is undoubtedly one of the most important factors to be considered in the etiology of these malformations. However, there is increasing evidence that environmental factors are important as well. According to Fogh- Anderson, [21] slightly less than 40% of the cases of CL/P are genetic in origin, whereas slightly less than 20% of the cases of isolated CP appeared to be genetically derived. Most investigations indicate that the inheritance pattern in CL/P is different from that in isolated CP. The mode of transmission of the defect is uncertain. This has been discussed by Bhatia, [22] who pointed out that the possible main modes of transmission are either by a single mutant gene producing a large effect, or by a number of genes (polygenic inheritance), each producing a small effect which together create this condition. It should be pointed out that cytogenetic studies have failed to reveal visible alterations in chromosomal morphology of the affected individuals. [23] Bixler [23] has expanded upon this concept and it is presumed that every individual carries some genetic susceptibility for clefting, but if this is less than the threshold level, there is no cleft. When the individual susceptibilities of both parents are added together in their offspring, a cleft occurs if the threshold values are exceeded. The second form of cleft is monogenic or syndromic and is associated with a variety of other congenital abnormalities. Since these are monogenic, they are of a high risk type.
Although there is insufficient evidence that nutritional disturbances cause cleft palate in human beings (non-syndromic), abnormal dietary regimens have caused developmental clefts in animals. [24] Cleft palate has been experimentally produced in new born rats by feeding diets either deficient or excessive in vitamin A to maternal rats during pregnancy. Riboflavin deficient diet fed to pregnant rats has also produced offsprings with a high incidence of cleft palate. The administration of cortisone to pregnant rabbits has induced similar clefts in their offsprings. Emotional or traumatic stress may play a significant role in the etiology of human CP, since stress induces increased functional burden on the adrenal cortex and secretion of hydrocortisone. However, Fraser and Warburton [25] have reported data which indicate that neither maternal emotional stress nor the lack of a prenatal nutritional supplement was causally related to the occurrence of CL/P. Despite the numerous clinical and experimental investigations, the etiology of CL/P in human beings is still largely unknown. It must be concluded, however, that heredity is probably the most important single factor.
The role of HLA complex in the pathogenesis of CL/P is still speculative and has not been established so far. However, anecdotal reports and the results of this study show that a few alleles have an increased frequency of expression in the diseased group which suggests that these alleles may predispose the individuals to develop CL/P. On the contrary, whether the alleles which showed an increased frequency of expression in the non-affected, healthy individuals exert a protective effect against cleft is rather speculative at present. Further analysis of the data to ascertain the predominant haplotype of the diseased individuals would be beneficial to aid early diagnosis and planning intervention strategies.
| References | | |
| 1. | Hagberg C, Larson O, Milerad J. Incidence of cleft lip and palate and risks of additional malformations. Cleft Palate Craniofac J 1998;35:40-5. 
|
| 2. | Carinci F, Pezzetti F, Scapoli L, Martinelli M, Carinci P, Tognon M. Genetics of nonsyndromic cleft lip and palate: A review of international studies and data regarding the Italian population. Cleft Palate Craniofac J 2000;37:33-40.
|
| 3. | Peanchitlertkajorn S, Cooper ME, Liu YE, Field LL, Marazita ML. Chromosome 17: Gene mapping studies of cleft lip with or without cleft palate in Chinese families. Cleft Palate Craniofac J 2003;40:71-9.
|
| 4. | Pezzetti F, Scapoli L, Martinelli M, Carinci F, Bodo M, Carinci P, et al. A locus in 2p13-p14 (OFC2), in addition to that mapped in 6p23, is involved in nonsyndromic familial orofacial cleft malformation. Genomics 1998;50:299-305.
|
| 5. | Zeiger JS, Hetmanski JB, Beaty TH, VanderKolk CA, Wyszynski DF, Bailey-Wilson JE, et al. Evidence for linkage of nonsyndromic cleft lip with or without cleft palate to a region on chromosome 2. Eur J Hum Genet 2003;11:835-9.
|
| 6. | Davies AF, Stephens RJ, Olavesen MG, Heather L, Dixon MJ, Magee A, et al. Evidence of a locus for orofacial clefting on human chromosome 6p24 and STS content map of the region. Hum Mol Genet 1995;4:121-8.
|
| 7. | Eiberg H, Bixler D, Nielsen LS, Conneally PM, Mohr J. Suggestion of linkage of a major locus for nonsyndromic orofacial cleft with F13A and tentative assignment to chromosome 6. Clin Genet 1987;32:129-32.
|
| 8. | Scapoli L, Pezzetti F, Carinci F, Martinelli M, Carinci P, Tognon M. Evidence of linkage to 6p23 and genetic heterogeneity in nonsyndromic cleft lip with or without cleft palate. Genomics 1997;43:216-20.
|
| 9. | Ghassibe M, Bayet B, Revencu N, Verellen-Dumoulin C, Gillerot Y, Vanwijck R, et al. Interferon regulatory factor-6: A gene predisposing to isolated cleft lip with or without cleft palate in the Belgian population. Eur J Hum Genet 2005;13:1239-42.
|
| 10. | Satokata I, Maas R. Msx1 deficient mice exhibit cleft palate and abnormalities of craniofacial and tooth development. Nat Genet 1994;6:348-56.
|
| 11. | Van den Boogaard MJ, Dorland M, Beemer FA, van Amstel HK. MSX1 mutation is associated with orofacial clefting and tooth agenesis in humans. Nat Genet 2000;24:342-3.
|
| 12. | Chenevix-Trench G, Jones K, Green AC, Duffy DL, Martin NG. Cleft lip with or without cleft palate: associations with transforming growth factor alpha and retinoic acid receptor loci. Am J Hum Genet 1992;51:1377-85.
|
| 13. | Suazo J, Santos JL, Carreno H, Jara L, Blanco R. Linkage disequilibrium between MSX1 and non-syndromic cleft lip/palate in the Chilean population. J Dent Res 2004;83:782-5.
|
| 14. | Sambrook J, Fritsch EF, Maniatis T. Molecular Cloning: A laboratory manual. In: Laboratory CSH, editor. 2 nd ed. New York: Cold Spring Harbor Laboratory Press; 1989. p. 1659.
|
| 15. | Seliger B, Ritz U, Ferrone S. Molecular mechanisms of HLA class I antigen abnormalities following viral infection and transformation. Int J Cancer 2006;118:129-38.
|
| 16. | Sakata Y, Tokunaga K, Yonehara Y, Bannai M, Tsuchiya N, Susami T, et al. Significant association of HLA-B and HLA-DRB1 alleles with cleft lip with or without cleft palate. Tissue Antigens 1999;53:147-52.
|
| 17. | Wegener S, Jakubik E, Schmidt M. HLA antigens in cleft lip-palate patients. Dtsch Z Mund Kiefer Gesichtschir 1990;14:378-82.
|
| 18. | Bonner JJ, Terasaki PI, Thompson P, Holve LM, Wilson L, Ebbin AJ, et al. HLA phenotype frequencies in individuals with cleft lip and/or cleft palate. Tissue Antigens 1978;12:228-32.
|
| 19. | Watanabe T, Ohishi M, Tashiro H. Population and family studies of HLA in Japanese with cleft lip and cleft palate. Cleft Palate J 1984;21:293-300.
|
| 20. | Hecht JT, Wang Y, Connor B, Blanton SH, Daiger SP. Nonsyndromic cleft lip and palate: no evidence of linkage to HLA or factor 13A. Am J Hum Genet 1993;52:1230-3.
|
| 21. | Fogh-Andersen P, editor. Inheritance of harelip and cleft palate. Copenhagen, Nyt, Nordisk Forlag: Arnold Busck; 1942.
|
| 22. | Bhatia SN. Genetics of cleft lip and palate. Br Dent J 1972;132:95-103.
|
| 23. | Bixler D. Genetic counseling in dentistry. Dent Clin North Am 1975;19:191-5.
|
| 24. | Tyler MS, Koch WE. In vitro development of palatal tissues from embryonic mice. III. Interactions between palatal epithelium and heterotypic oral mesenchyme. J Embryol Exp Morphol 1977;38:37-48.
|
| 25. | Fraser FC, Warburton D. No association of emotional stress or vitamin supplement during pregnancy to cleft lip or palate in man. Plast Reconstr Surg 1964;33:395-9.
|
[Figure 1]
[Table 1], [Table 2], [Table 3], [Table 4]
|