|
 
 |
|
CASE REPORT |
|
|
|
| Year : 2013 | Volume
: 19
| Issue : 1 | Page : 101-103 |
| |
Short stature and an interesting association
Latha Magatha Sneha, Kishore Thanasegarapandian, Venkataraman Paramasivam, Julius Xavier Scott
Department of Pediatrics, Sri Ramachandra University, Chennai, Tamil Nadu, India
| Date of Web Publication | 4-Jun-2013 |
Correspondence Address:
Julius Xavier Scott
Department of Pediatrics, Sri Ramachandra University, Porur, Chennai - 600 116, Tamil Nadu
India
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0971-6866.112919

 Abstract Abstract | | |
Untreated hypothyroidism in children usually results in delayed puberty, but juvenile hypothyroidism causes isosexual precocious puberty in a rare syndrome called Van Wyk Grumbach syndrome, with a complete reversal to the pre pubertal state following thyroid hormone replacement therapy. We report here, a 7-year-old girl who presented with short stature, constipation and isosexual precocious puberty due to the long standing untreated severe hypothyroidism with this syndrome.
Keywords: Hypothyroidism, precocious puberty, short stature
How to cite this article:
Sneha LM, Thanasegarapandian K, Paramasivam V, Scott JX. Short stature and an interesting association. Indian J Hum Genet 2013;19:101-3 |
How to cite this URL:
Sneha LM, Thanasegarapandian K, Paramasivam V, Scott JX. Short stature and an interesting association. Indian J Hum Genet [serial online] 2013 [cited 2016 May 24];19:101-3. Available from: http://www.ijhg.com/text.asp?2013/19/1/101/112919 |
| Introduction | |  |
Van Wyk Grumbach syndrome (VWGs) is characterized by juvenile hypothyroidism, delayed bone age and isosexual precocious puberty with complete reversal to the pre pubertal state after thyroid replacement therapy. We report a case of a 7-year-old girl with isosexual precocious puberty, short stature and constipation due to the untreated, long standing hypothyroidism.
| Case Report | | |
A 7-year-old girl presented with complaints of growth failure and constipation since last 1 year and regular vaginal bleeding for last 6 months which was reassured by their family physician as normal variant of early menarche. Mother has not noticed any breast development or abnormal hair growth. She was also found to have decreased physical activity, excessive sleepiness, easy fatiguability, lack of interest in interaction with family members and deteriorating performance at school. There was no history suggestive of any intra cranial mass, head trauma or receiving radiation therapy and hormonal drugs in the past. She was first born to non-consanguineous parents, without any significant family history or any medical illness. She was a developmentally normal child, with good scholastic performance. The other sibling is normal who was 3 years younger but still taller than her.
Physical examination revealed pallor, expressionless face, coarse facies, facial puffiness, short neck [Figure 1] and short stubby fingers [Figure 2]. There was no thyroid enlargement. Tanner staging was pre pubertal with just palpable breast buds, no axillary or pubic hair and without any enlargement of external genitalia. Examination of abdomen demonstrated diffuse distention with palpable fecal mass. Anthropometry values showed height and weight less than the 3 rd centile, body mass index was 20 and upper segment: Lower Segment ratio was 1:1.1. Investigations showed microcytic hypochromic anemia with a hemoglobin level of 7.5 g/dl, Thyroid Stimulating Hormone >150 μIU/ml (0.35-5.5), T 4 <0.01 ng/ml (4.5-12.6), Follicle Stimulating Hormone 8.32 mIU/ml (0.3-2) and Leutenizing Hormone 0.05 mIU/ml (0.1-6). Her radiological investigations revealed a bone age corresponding to 5 years. Ultrasonography of the pelvis showed enlarged ovary on the left side with multiple follicles in both the ovaries. Endocrinologist opinion was sought and she was started on Sodium levo thyroxin. After 2 weeks of treatment with thyroxine replacement therapy, she had dramatic improvement with resolution of constipation and cessation of menstrual cycles. She was found to be cheerful and active, during her review after 3 months.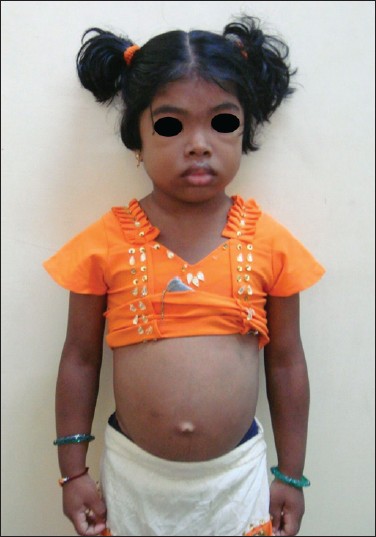 | Figure 1: Coarse facies, facial puffiness, short neck and abdominal distention
Click here to view |
| Discussion | | |
Sexual precocity is usually associated with increase in linear height, epiphyseal fusion, acceleration of bone maturity and ultimately leading to short stature. Incomplete isosexual precocity is rarely associated with long standing untreated primary hypothyroidism in both boys and girls causing impaired growth and delayed skeletal maturation. The clinical syndrome of severe primary hypothyroidism associated with isosexual precocious puberty in females was first described by Kendle in 1905. [1] The association in young females of long standing primary hypothyroidism, isosexual precocious pseudopuberty and multi-cystic enlarged ovaries was first described in 1960 by Van Wyk and Grumbach. [2] The precocious puberty seen in this syndrome is always isosexual and incomplete. [3] Girls have breast development, enlarged labia minora, irregular vaginal bleed, estrogenic changes in vaginal smear, usually without appearance of pubic hair. Boys have macro orchidism but with no signs of virilization. Other consistent findings are autoimmune thyroiditis, peripubertal onset of symptoms, elevated serum prolactin and follicular stimulating hormone levels but low or normal luteinizing hormone levels. [4],[5] There is usually pituitary enlargement which may lead to a misdiagnosis of pituitary tumor. It is important to recognize this syndrome because initiating simple thyroid hormone replacement completely resolves symptoms and hormone abnormalities, avoiding unnecessary investigations for malignancies or surgical intervention.
The exact mechanism of the development of precocious puberty in VWGS still remains speculative. Postulated mechanisms are 'specificity spill over' which means positive feed-back effect of low serum thyroxine on pituitary gonadotropins as they are also glycoprotein hormones like TSH, all of which have a common alpha summit. [3] TSH levels are consistently elevated in such patients and the tendency to manifest sexual precocity may be directly related to the severity of TSH elevation, as has been found out that the low FSH like activity of TSH can become significant at very high concentrations. [6] Hyperprolactinaemia, reduced gonadotropin clearance and decreased dopaminergic and opioid tone at the hypothalamo-pituitary axis are other plausible explanations. [7],[8] Though elevated serum gonadotropins and estradiol levels are seen in gonadotropin-dependent precocious puberty (GDPP), however, this can be differentiated by the gonadotropin response to luteinizing hormone releasing hormone which is present in GDPP but not in hypothyroidism-associated precocity. Still others have proposed that the proximate nature of the Thyrotropin Releasing Hormone center to the Gonadotropin Releasing Hormone center in the hypothalamus leads to excessive production of both releasing factors. One more proposal is that prolactin plays a primary role in the disease process, by sensitizing the ovaries to gonadotropins or that TSH itself sensitizes the ovaries to gonadotropin stimulation. [4],[5] The increased FSH or FSH like activity of TSH causes a high FSH/LH ratio in contrast to high LH/FSH ratio in normal puberty, thereby causing the increased ovarian estrogen secretion and multicystic ovaries. [9] The common causes of an incomplete isosexual precocity are intake of hormonal preparations, sex hormone secreting tumors, McCune Albright syndrome. However, the bone age is advanced in all these cases and the delayed bone age in our case directed us towards a diagnosis of hypothyroidism. High TSH and Low LH levels in this case with precocious puberty helped us to think of VWGs.
Although there is no definite consensus regarding the precise etiopathogenesis of the disorder, but there is no ambiguity as far as the treatment is concerned. All symptoms subside, the endocrine abnormalities resolve and even the ovarian cysts decrease in size or altogether disappear, with thyroxin replacement, as we witnessed in our case during follow-up. We report this interesting and rare association of hypothyroidism and precocious puberty for the pediatricians to be aware of this condition, which will avoid unnecessary investigations and interventions.
| References | | |
| 1. | Kendle FW. Case of precocious puberty in a female cretin. Br Med J 1905;1:246. 
|
| 2. | Van Wyk JJ, Grumbach MM. Syndrome of precocious menstruation and galactorrhea in juvenile hypothyroidism. An example of hormonal overlap in pituitary feedback. J Pediatr 1960;57:416-35.
|
| 3. | Evers JL, Rolland R. Primary hypothyroidism and ovarian activity evidence for an overlap in the synthesis of pituitary glycoproteins. Case report. Br J Obstet Gynaecol 1981;88:195-202.
|
| 4. | Takeuchi K, Deguchi M, Takeshima Y, Maruo T. A case of multiple ovarian cysts in a prepubertal girl with severe hypothyroidism due to autoimmune thyroiditis. Int J Gynecol Cancer 2004;14:543-5.
|
| 5. | Chattopadhyay A, Kumar V, Marulaiah M. Polycystic ovaries, precocious puberty and acquired hypothyroidism: The Van Wyk and Grumbach syndrome. J Pediatr Surg 2003;38:1390-2.
|
| 6. | Rastogi A, Bhadada SK, Bhansali A. An unusual presentation of a usual disorder: Van Wyk: Grumbach syndrome. Indian Endocrinol Metab 2011;15:141-3.
|
| 7. | Suter SN, Kaplan SL, Aubert ML, Grumbach MM. Plasma prolactin and thyrotropin and the response to thyrotropin-releasing factor in children with primary and hypothalamic hypothyroidism. J Clin Endocrinol Metab 1978;47:1015-20.
|
| 8. | Thomas R, Reid RL. Thyroid disease and reproductive dysfunction: A review. Obstet Gynecol 1987;70:789-98.
|
| 9. | Lt Col TK Jagadhish. Van Wyk Grumbach Syndrome: A Syndrome of Incomplete Isosexual precocity and Juvenile Hypothyroidism. J Assoc Physicians India 2002;58:343-5.
|
[Figure 1], [Figure 2]
|











