|
 
 |
|
CASE REPORT |
|
|
|
| Year : 2013 | Volume
: 19
| Issue : 2 | Page : 262-265 |
| |
Derivative chromosome 11 in a child resulting from a complex rearrangement involving chromosomes 3, 6 and 11 in father: Significance of parental karyotyping
Prabhat Ranjan, Kundanbala Desai, Shailaja Gada Saxena
Department of Molecular Medicine, Reliance Life Sciences, Navi Mumbai, India
| Date of Web Publication | 5-Aug-2013 |
Correspondence Address:
Shailaja Gada Saxena
Molecular Medicine, Reliance Life Sciences, R-282, DALC, TTC Area of MIDC, Thane Belapur Road, Rabale - 400 701, Navi Mumbai
India
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/0971-6866.116105

 Abstract Abstract | | |
The presence of derivative chromosome in a child with phenotypic features necessitates the need of parental karyotyping to ascertain the exact amount of loss or gain of the genetic material. The aim of this study was to emphasize the importance of parental karyotyping. Cytogenetic evaluation of the proband and his father were carried out at Laboratory. Cytogenetic analysis was performed on phytohemagglutinin stimulated cultures. The derivative chromosome 11 in proband was ascertained to have additional material from chromosome 6p arising from complex chromosomal rearrangement in the father. Karyotyping is the basic, cost-effective preliminary investigation in a child with mental subnormality or congenital anomalies.
Keywords: Balanced translocations, complex chromosomal rearrangement, derivative chromosome, genetic counseling, intellectual disability, karyotyping
How to cite this article:
Ranjan P, Desai K, Saxena SG. Derivative chromosome 11 in a child resulting from a complex rearrangement involving chromosomes 3, 6 and 11 in father: Significance of parental karyotyping. Indian J Hum Genet 2013;19:262-5 |
How to cite this URL:
Ranjan P, Desai K, Saxena SG. Derivative chromosome 11 in a child resulting from a complex rearrangement involving chromosomes 3, 6 and 11 in father: Significance of parental karyotyping. Indian J Hum Genet [serial online] 2013 [cited 2016 May 24];19:262-5. Available from: http://www.ijhg.com/text.asp?2013/19/2/262/116105 |
| Introduction | |  |
Chromosomal rearrangements, balanced or unbalanced are caused by the exchange of chromosomal segments between two or more non-homologous chromosomes with minimum two breakpoints. Structural rearrangements, detected using conventional cytogenetic analysis occur in approximately, 0.5% of new-born infants. [1] Balanced rearrangements are often not associated with any phenotypic abnormalities and may remain undetected through multiple generations and come to light due to reproductive problems including infertility, recurrent spontaneous abortions, stillbirths or child with congenital anomalies, dysmorphic features or mental retardation, attributed to meiotic events resulting in production of abnormal gametes. [2] Certain rearrangements, apparently balanced at the microscopic level, include deletions, duplications, insertions and/or inversions at the molecular level and these cases are clinically presented with subtle physical deformities, autism, and intellectual disability. [3] Unbalanced rearrangements are associated with phenotypic features due to loss or gain of chromosomal material in form of partial monosomy and partial trisomy. These rearrangements can cause disease by physically disrupting genes or altering their regulatory environment. Derivative chromosomes are structurally rearranged chromosome generated by a rearrangement involving two or more chromosomes or rarely by multiple rearrangements within a single chromosome. It is important to ascertain the origin of these derivative chromosomes to know the exact amount of loss or gain of the genetic material. In certain cases, the structural chromosomal rearrangements involve at least three breakpoints and involve the exchange of genetic material between two or more chromosomes and these are termed as complex chromosomal rearrangements (CCRs).
Hereby, we present a case of a child with history of mental retardation and convulsion, having a derivative chromosome 11 with presence of additional chromosomal material of unknown origin identified on conventional karyotyping.
| Case Report | | |
The proband, a 3-year-old, morphologically normal male child born from full-term normal delivery to a phenotypically normal couple presented with a clinical history of mental retardation with convulsion, and was referred for cytogenetic analysis. The couple had a history of two first-trimester spontaneous abortions. However, there was no prior family history of congenital anomalies or other inherited disorders. The abortuses from earlier pregnancies were not subjected to cytogenetic analyses. Cytogenetic analysis was carried out on phytohemagglutinin stimulated peripheral blood lymphocytes, cultured in Roswell Park Memorial Institute (RPMI) 1640 medium, using modified standard protocol. [4] Twenty G-banded metaphases were analyzed using Cytovision software, and designated as per ISCN (2009) nomenclature at 550 bands per haploid genome.
The karyotype of G-banded metaphase of the proband revealed derivative chromosome 11 arising from the presence of additional material of unknown origin on the short arm of chromosome 11 at band 11p15.2. To ascertain the origin of derivative chromosome identified in the child, the parental samples were requested for cytogenetic studies. Mother had an apparently normal karyotype (46,XX) reported earlier. The karyotype of father revealed a CCR involving chromosomes 3, 6, and 11, the breakpoints being 3p22, 6p22.1 and 11p15.2 respectively, with the karyotype representation as 46, XY, t(3;6;11) (p22;p22.1;p15.2) as depicted in [Figure 1]. This was an apparently balanced translocation since the father had no phenotypic features. Hence, the final karyotype of the child was designated as 46,XY,der(11) t(6;11)(p22.1;p15.2)pat, indicating partial trisomy for 6p22.1-pter and monosomy for 11p15.2-pter. The derivative chromosome 11 from father had directly passed to the child, resulting in unbalanced karyotype in child.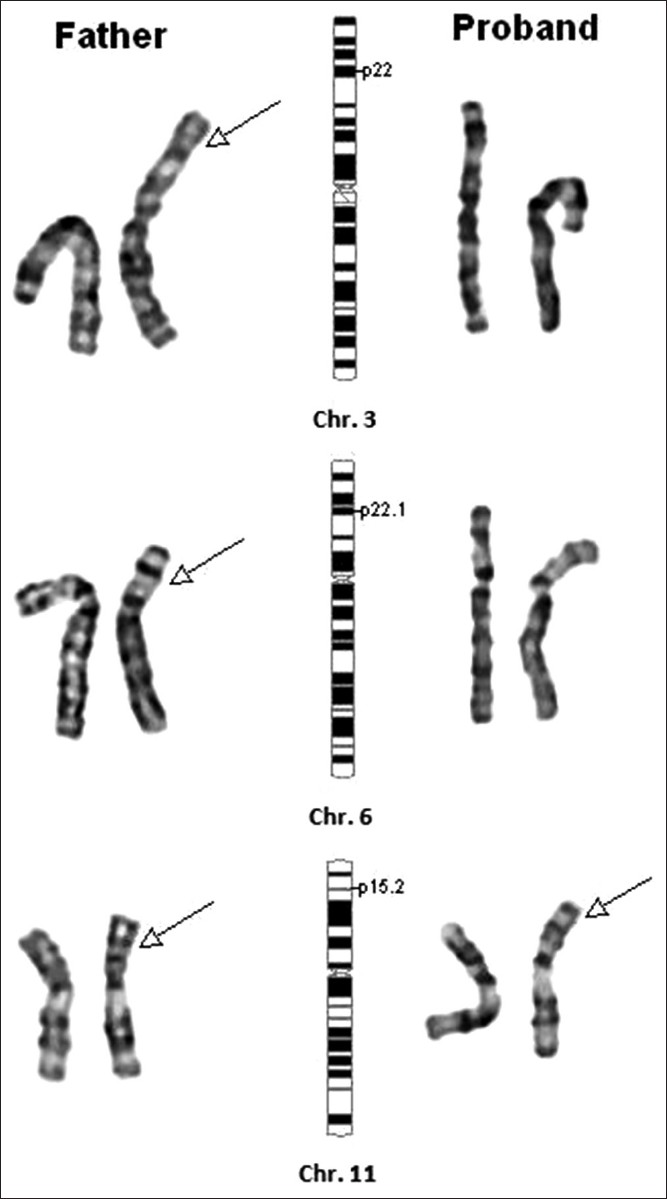 | Figure 1: Partial karyotype of the proband and the father. Father: Translocation of segment on chr. 3 distal to 3p22 onto chr. 6 at band 6p22.1, translocation of the segment on chr. 6 distal to 6p22.1 onto chr. 11 at 11p15.2 and translocation of the segment on chromosome 11 distal to 11q15.2 onto chr. 3 at 3p22. Proband: Direct transmission of derivative chr. 11 containing the segment of chr. 6 from father resulting in unbalanced karyotype - partial 6p22.1 - pter and partial Monosomy 11p15.2-11pter
Click here to view |
| Discussion | | |
Identification of a derivative chromosome in a child with the presence of chromosomal material of unknown origin warrants the need for genetic counseling and parental karyotyping. In the present report, presence of additional chromosomal material on chromosome 11 at 11p15.2 was ascertained to be segment 6p22.1 to pter resulting in partial trisomy of 6p and was transmitted from the father who had a complex apparently balanced translocation involving chromosomes 3, 6 and 11. Despite the increasing understanding of the mechanisms involved in their genesis, CCRs arise as unique, complex events for which the genetic and reproductive counseling of carriers remains a challenge.
Since, the first case of trisomy 6p in 1971, there have been many reports of partial trisomy 6p with the proximal breakpoint ranging from 6p11-6p25 in children, generally secondary to a familial reciprocal translocation with clinical feature such as moderate mental retardation, psychomotor retardation, craniofacial and pigmentary anomalies, hypotrophy, nystagmus, high nasal bridge, small mouth, sacral dimple, and systolic murmur, hydronephrosis, proteinuria, and hyperglycemia. [5],[6] In the present report, the child was morphologically normal and had no other clinical features except mental retardation and convulsions. There are not many reports describing the clinical features associated with monosomy for the distal part of short arm of chromosome 11, though, this region has been demonstrated to be involved with Russell Silver syndrome and Beckwith-Wiedemann syndrome More Details.
| Conclusion | | |
It is imperative to record the description and characterize balanced or unbalanced complex chromosome rearrangements as it would be of importance in counseling and prenatal investigations in future pregnancies. Providing efficient genetic counseling becomes very significant for CCR carriers and should be offered before as well as after the pregnancies. The couples with CCR should also be informed about the possible outcomes of the progeny and the fact that exact risk of malformation is still unknown and that phenotypically normal child can still have a high-risk of reproductive problems. It is too difficult to analyze derivative chromosome carrying one or more than one type of structural chromosomal aberration. As in our case report, the derivative chromosome 11 of male child was unanalyzable and very difficult to identify the source of additional chromosomal material on chromosome 11. This is why parental karyotyping becomes necessity and very relevant in tracing the origin of derivative. In addition, the couple had two first trimmest abortions prior to the birth of this child. Had the products of conception from the earlier pregnancies been analyzed, or the couple had been counseled to do karyotyping analysis before planning subsequent pregnancy, the CCR in the father could have been identified before the birth of this child with the derivative chromosome. Further, molecular level diagnosis is required to ascertain the exact amount and effect of loss due to the loss at genetic level. Several methods such as whole chromosome painting by fluorescent in situ hybridization, comparative genomic hybridization and DNA microarray play a very significant role in identifying the translocation partner and/or ascertaining the exact amount of deviations from normal pattern. These techniques are not readily available for all patients and hence continuing with the parental cytogenetic studies by karyotyping still remains the basic preliminary investigation for all children with mental subnormality or congenital anomalies or for couples with history of infertility, or repeated adverse obstetric outcome like repeated spontaneous abortions or birth of child with congenital anomalies. Karyotyping is an inexpensive technique which gives the complete genomic picture, and should be made a mandatory investigation in couples with repeated abortions or where there has been a birth of child with multiple congenital anomalies. This can help in better patient counseling and thus, better patient management. During reproductive counseling, it is important to explain the recurrence risk to the couples and also offer them the option of in vitro fertilization and pre-implantation genetic diagnosis, which may have a limited role in management of couples with CCRs, due to the high rate of unbalanced gametes and possibility of apparently balanced gametes with functional abnormalities in the offspring of carriers with CCR. The alternative of donor gametes or adoption may also be recommended.
| Acknowledgment | | |
The authors acknowledge the help and support of Reliance Life Sciences, Navi Mumbai.
| References | | |
| 1. | Jacobs PA. The chromosome complement of human gametes. In: Milligan SR, editor. Oxford reviews of reproductive biology. Vol. 14. New York: Oxford University Press; 1992. p. 47-72. 
|
| 2. | Gorski JL, Emanuel BS, Zackai EH, Mennuti M. Complex chromosomal rearrangement and multiple spontaneous abortions. Hum Genet 1986;74:326.
|
| 3. | Sobreira NL, Gnanakkan V, Walsh M, Marosy B, Wohler E, Thomas G, et al. Characterization of complex chromosomal rearrangements by targeted capture and next-generation sequencing. Genome Res 2011;21:1720-7.
|
| 4. | Moorhead PS, Nowell PC, Mellman WJ, Battips DM, Hungerford DA. Chromosome preparations of leukocytes cultured from human peripheral blood. Exp Cell Res 1960;20:613-6.
|
| 5. | Bernheim A, Berger R, Vaugier G, Thieffry JC, Matet Y. Partial trisomy 6p. Hum Genet 1979;48:13-6.
|
| 6. | Giardino D, Finelli P, Caufin D, Gottardi G, Lo Vasco R, Turolla L, et al. Pure 6p22-pter trisomic patient: Refined FISH characterization and genotype-phenotype correlation. Am J Med Genet 2002;108:36-40.
|
[Figure 1]
|









