| |


 |
| Year : 2011 | Volume
: 5
| Issue : 1 | Page : 1-8 |
|
|
|
|
|
REVIEW ARTICLE Sprengel's deformity of the shoulder: Current perspectives in management
Aditya Sai Kadavkolan, Deepak N Bhatia, Bibhas DasGupta, Pradeep B Bhosale
Department of Orthopaedic Surgery, Seth GS Medical College & King Edward VII Memorial Hospital, Parel, Mumbai, India
Correspondence Address:
Deepak N Bhatia
Department of Orthopaedic Surgery,Seth GS Medical College & King Edward VII Memorial Hospital, Parel, Mumbai - 400 012
India
 Source of Support: None, Conflict of Interest: None  | 3 |
DOI: 10.4103/0973-6042.80459

|
|
|
|
| Date of Web Publication | 6-May-2011 |
 Abstract Abstract | | |
Sprengel's deformity or congenital elevation of scapula is a complex deformity of the pectoral girdle, and results in symptomatic cosmetic and functional disability. Several studies have attempted to analyze the three-dimensional aspects of this deformity; optimal methodologies of quantification and surgical correction techniques have been debated since the condition was first described. This article presents a concise review of the exact pathoanatomy, clinical presentation, imaging techniques, and surgical procedures described in the management of this condition.
Keywords: Congenital anomaly, shoulder, Sprengel′s deformity
How to cite this article:
Kadavkolan AS, Bhatia DN, DasGupta B, Bhosale PB. Sprengel's deformity of the shoulder: Current perspectives in management. Int J Shoulder Surg 2011;5:1-8 |
| Introduction | |  |
Congenital elevation of the scapula or 'Sprengel's shoulder' is an anomaly of the shoulder girdle that is associated with abnormal descent, and altered position and anatomy of the scapula. The deformity is usually associated with muscle hypoplasia or atrophy, and a combination of these factors results in disfigurement and functional limitation of the shoulder. [1] The earliest description of this condition was reported in 1863 by Eulenberg; he reported three cases of hochgradige dislocation der scapula and described its association with dorsal scoliosis. Subsequent cases were described in 1880, 1883, and a method of surgical correction was suggested in 1888. [2] In 1891, Sprengel drew attention to this deformity, which he described as angeborene verschiebung des schulterblattesnachoben, and advocated a plausible theory for the existence of this deformity.
| Developmental, Normal and Pathological Anatomy | | |
The scapula develops embryologically along with the upper limb; it appears during the fifth week in the upper dorsal / lower cervical region with the arm bud and descends up to the final anatomical position of one of the second-to-eighth dorsal vertebrae by 12 weeks of gestation. [2],[3],[4],[5] The horizontal diameter, measured at the base of the spine of the scapula, is less than the vertical diameter. Broca suggested a "scapular index" to describe the relationship between the horizontal and the vertical lengths of the scapula; this was represented by a formula (100× breadth/length) and calculated to be approximately between 63 and 71. [2] Similarly, others have used a "subscapular angle," a "supraspinous angle" and an "infraspinous angle" to describe deviation from the normal. [2]
The trapezius inserts along the medial border of the scapula and resists the upward-directed forces of the levator scapulae and the rhomboids; it has been reported to be atrophied in cases of acquired elevation of the scapula. [2] The other muscles acting on the scapula are pectoralis major, rhomboids, levator scapulae, serratus anterior and latissimus dorsi; varying degrees of involvement of these muscles may be seen in congenital elevation of the scapula.
The pathology in Sprengel's deformity probably represents a continuance of the fetal form of the scapula. The smaller deformed scapula has a horizontal diameter that exceeds the vertical diameter; anterior curving of the supraspinous portion with prolongation of the superior medial scapular angle has been described. Other pathoanatomical findings include an omovertebral bar, articulations with the vertebral column; and these may extend from the superomedial scapular angle or the upper third of the medial border of the scapula up to the transverse process of a cervical vertebra (one of the fourth-to-seventh vertebrae). [1],[2],[4],[5],[6],[7],[8],[9],[10],[11] Additionally, costovertebral defects (spina bifida and kyphoscoliosis) and underdevelopment of pectoral girdle bones (clavicle, humerus) and musculature (pectoralis major, trapezius) may coexist. [2],[4],[7]
| Clinical Features | | |
The demographics, clinical presentation, common clinical associations, and differential diagnoses are summarized in [Table 1],[Table 2],[Table 3],[Table 4]. The cosmetic aspect of the deformity has been classified by Cavendish into four grades in an attempt to simplify indications for treatment [Table 5]. [9] The functional aspect of the deformity has been attributed to (a) a forward curvature of the superior angle of the scapula over the apex of the thorax, (b) abutment of the medial scapular border against the spinous processes of adjacent vertebrae and (c) the omovertebral bone [Figure 1]a-b. [10] Syndromes associated with Sprengel's deformity include teratological conditions such as inencephaly (a triad of occipital defect, spina bifida of cervical vertebrae, and fixed retroflexion of the head) and the Klippel-Feil syndrome More Details [Table 6]. [8]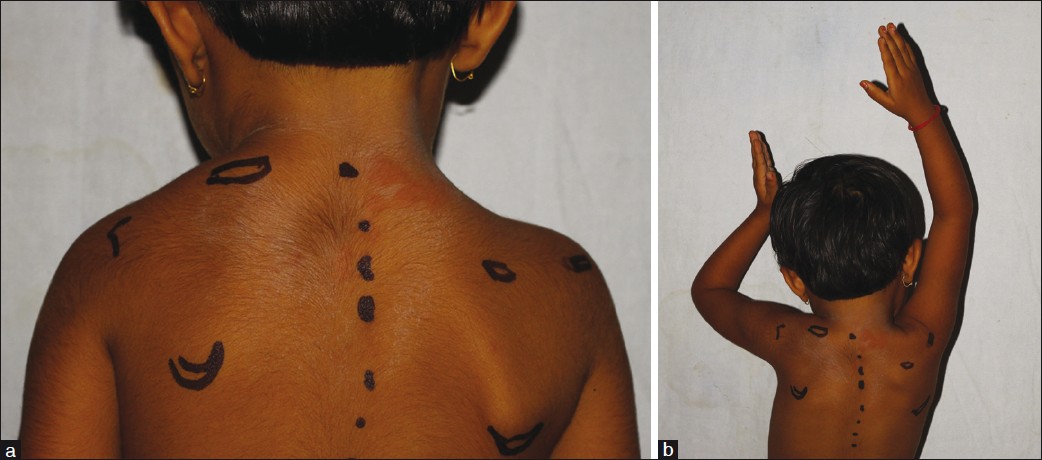 | Figure 1: (a) Cosmetic aspect of Sprengel's deformity is shown. The landmarks show marked elevation of the left scapula as compared with the right; (b) Functional aspect of Sprengel's deformity is shown. Marked restriction of abduction on the left side is seen as compared to the right
Click here to view |
| Imaging | | |
Plain radiographs can be used for assessing the deformity and presence of omovertebral communication, and to note the postoperative correction. Based upon the frontal radiographs and the relation of the superomedial angle to the vertebral column, Rigault proposed a classification to assess the deformity [Table 7]. [12] Woodward described an oblique view to assess the presence of the omovertebral bone between the superomedial angle of the scapula and the vertebral column [Figure 2]. [10] Ahmad described the distances between the inferior and the superomedial angles of the scapula and the spinal column, and the angle of glenoid tilt, to assess the postoperative outcomes [Figure 3]. [13] Cho et al. used three-dimensional CT (3D-CT) to evaluate scapular dysplasia and malpositioning and suggested roles in preoperative planning. These authors described the affected scapulae to be larger than the contralateral ones, and demonstrated a decrease in their height-to-width ratio without a significant difference in glenoid version. Moreover, they found an inverse relationship between scapular rotation and superior displacement [Figure 4],[Figure 5],[Figure 6]. [1] | Figure 2: Oblique radiograph (arrow - omovertebral bar; H - Hypoplastic humerus)
Click here to view |
 | Figure 3: Frontal radiograph of a patient with Sprengel's deformity (Rigault grade III). (X - Line drawn perpendicular to the body axis 'A'; Y - Line joining the superior and inferior edges of the glenoid; O - Angle between lines X and Y; b: distance between the inferior angle of the normal scapula and the spine; b' - Distance between the inferior angle of the affected scapula and the spine; a - The distance between the superior angle of the normal scapula and the spine; a' - Distance between the superior angle of the affected scapula and the spine
Click here to view |
 | Figure 4: CT scan (A) and 3D reconstruction (B, C and D) show the omovertebral connection (thick arrow) arising from the medial border of the scapula and the vertebral column. (B) shows anterior curving of the supraspinous portion of the affected scapula (arrow). (D) shows the convex medial border and the concave lateral border of the affected scapula (multiple arrows)
Click here to view |
 | Figure 5: Superior displacement of the affected scapula is represented as a ratio of A to B. Y represents a line drawn from the center of the glenoid of the abnormal scapula, Z represents a line drawn from the center of the glenoid of the right scapula, both Y and Z are perpendicular to the vertebral axis, and X is the vertical body axis; A is the distance between the points at which the lines intersect the spinal column; B is the vertical height of the normal scapula
Click here to view |
 | Figure 6: Rotational deformity of the affected scapula is represented by the difference between lines Z and Y (X - Vertebral column axis; AB - A line joining the center of the glenoid and the base of scapular spine to the vertebral column axis on the affected side; CD - A line joining the center of the glenoid and the base of scapular spine to the vertebral column on the normal side; Y - Angle between AB and X; Z - angle between CD and X)
Click here to view |
| Treatment | | |
The goal of surgical intervention for Sprengel's deformity is cosmetic and functional improvement; however, the condition is often associated with other anomalies such as torticollis and congenital scoliosis, which limit the amount of correction that can be obtained. Patients with bilateral deformities or grade 1 Cavendish deformity may be observed for progression; patients with grade 4 deformities should be offered a guarded prognosis; and surgery may be avoided in patients with short necks and concomitant grade 4 deformity. [9] Surgical intervention before the age of 2 years is extensive and is technically more difficult. Best results are obtained if surgery is performed below the age of 5 years. [7],[14] Jeannopoulos advised a resection of the superomedial part with omovertebral bone excision as the only procedure in patients above the age of 6 years. [7] Factors to be assessed while evaluating a patient for surgery include severity of the deformity, functional impairment, age, and associated comorbid conditions. [10] Hence surgery is best advisable for a patient between 3 and 8 years of age, and with moderate or severe cosmetic/ functional deformity. The presence of associated congenital anomalies may be contraindications to operation. [10]
The surgical procedures involve a combination of (a) scapular lowering with either the shift of the origin or the insertion of the scapular muscles on the spine/ scapula, (b) resection of the superomedial border and (c) omovertebral bar resection [9],[15] [Table 8]. A clavicular morselization is sometimes recommended as a concomitant deformity of this bone may reduce the correction obtained. [9] Putti's procedure consisted of detachment of the scapular insertion of the rhomboids and trapezius, omovertebral bar resection, followed by lowering the scapula and fixing its inferior angle to a rib at the corrected level. [7] Shrock modified Putti's procedure by suggesting subperiosteal dissection of the musculature and adding an osteotomy of the supraspinous scapular region and the acromial base to facilitate scapular descent. [5] Woodward described a procedure for correction of the deformity, involving distal shift of the origin of the trapezius and the rhomboids on the spine [Figure 7]a-b. This was maintained by placing the scapula in a pocket of the trapezius muscle. Ahmad proposed a modification to the Woodward's procedure, for achieving better abduction and correction of the glenoid tilt; the scapula was anchored to the lower dorsal vertebrae by a stout absorbable suture placed through the superomedial scapula, so as to externally rotate it and cause lateral displacement of the inferior angle, thereby achieving correction of glenoid vara. [16] Green described a technique that involved resection of the prominent superior scapular border and extra-periosteal division of the muscular attachments of scapula to allow the scapula to be displaced inferiorly and muscular reattachment at the newer corrected level at the scapula [Figure 8]. Andrault et al. suggested modifications to Green's procedure; these included (a) dis-insertion of supraspinatus, (b) clavicular osteotomy and (c) a limited release of the serratus anterior to facilitate the descent of the scapula. The authors suggested that the incidence of brachial plexus palsy could be reduced by clavicular osteotomy, and that scapular winging could be prevented by doing only a limited release of serratus anterior from the medial scapular border. [17] | Figure 7: (a) Diagrammatic representation of Woodward's procedure: The origins of trapezius and rhomboids (B) are resected from the spinous processes (A - Omovertebral bar; B - Elevation of trapezius and other scapular musculature; C - Levator scapulae). Inset - Top right shows morselization of the clavicle; 'Cl' and 'Cm' - The lateral end and the medial end of the clavicle, respectively; P - Periosteum sutured over the morselized part; Black arrows - Extent of the morselization; White arrows - Sutured periosteum.; (b) Shaded area indicates extraperiosteal excision of the omovertebral bar and the supraspinous portion of the scapula. The aponeurosis of trapezius and rhomboids (A) are sutured over the scapula in the corrected position
Click here to view |
 | Figure 8: Diagrammatic representation of Green's procedure. Shaded region indicates the area of resection (omovertebral bar, supraspinous fossa). (A - Dis-inserted trapezius; B - Levator scapula; C - Dis-inserted rhomboids - major and minor)
Click here to view |
Mears described a procedure which involved (a) subperiosteal elevation of the scapular musculature, (b) extraperiosteal resection of the omovertebral bone, (c) supraspinatous fossa osteotomy, (d) release of long head of triceps and a portion of the origin of teres minor from the scapula and (e) resection of the superolateral border of the scapula to gain abduction [Figure 9]. The gain in shoulder abduction is more with this procedure as compared to the others described for Sprengel's deformity. [15],[18] Other procedures described include vertical scapular osteotomy and partial scapulaectomy. Wilkinson et al. described a vertical scapular osteotomy which consisted of a vertical osteotomy, 1 cm from the vertebral edge of the scapula so as to lower the lateral part till both the spines were at the same level. [19] Zhang et al. described a partial scapulaectomy for correction of the scapular deformity; the superior potion of the spine of scapula was osteotomized, and the omovertebral bar was excised. The adequacy of the correction was judged by comparing the superior borders of the two scapulae. [20] | Figure 9: Diagrammatic representation of Mears' procedure. The shaded region represents the area to be osteotomized (A - Reflected trapezius; B - Rhomboids; C - Levator scapulae; T - The detached triceps)
Click here to view |
| Results | | |
A number of procedures have been described for correction of the Sprengel's deformity, and an equally large number of studies have been attempted to assess the outcome [Table 9]. A direct comparison of the results is difficult as various authors have used different techniques for correction and different outcome-assessment measures. The inferior angle, the superior border, the spine or the center of the scapula, all have been used to assess the correction. [10],[11],[20],[21] Gain in range of abduction is comparable and its mean value ranges from 19° to 70° in various studies, with a greater gain seen in patients with a more severe preoperative restriction. [9],[10],[11],[17],[18],[19],[20],[21],[22],[23],[24],[25] Surgical complications described include scar-related complications, brachial plexus palsy, brachial neuritis, winging of the scapula, regeneration of the omovertebral bar, recurrence of the deformity and prominence of the sternoclavicular joint. [9],[10],[11],[15],[16],[17],[18],[19],[20],[21],[22],[23] Current recommendation from studies analyzed include the following: a clavicular osteotomy may be added in severe cases to facilitate scapular descent without causing neurovascular complications [2] ; Woodward's procedure may be avoided in patients with pre-existing scapular winging [3] ; there is no constant correlation of anatomical and cosmetic results with recurrence of the deformity, age of the patient and functional outcome. [7],[10],[17],[21]
| Conclusions | | |
Sprengel's deformity of the shoulder is a dysplasia of the pectoral girdle, resulting in cosmetic and functional disability. The deformity is associated with other congenital anomalies, which often dictate the management and outcome of treatment. Surgical techniques described in literature provide a satisfactory cosmetic and functional outcome, and a low complication rate.
| References | | |
| 1. | Cho TJ, Choi IH, Chung CY, Hwang JK. The Sprengel deformity morphometric analysis using 3D-CT and its clinical relevance.J Bone Joint Surg Br 2000;82:711-8. 
|
| 2. | Horwitz AE. Congenital elevation of the scapula.-Sprengel's deformity.J Bone Joint Surg Am1908;s2-6:260-311.
|
| 3. | Rutherford NC. A contribution to the embryology of the fore-limb skeleton.J Anat physiol 1914;48:355-77.
|
| 4. | Tsirikos AI, McMaster MJ. Congenital anomalies of the ribs and chest wall associated with congenital deformities of the spine.J Bone Joint Surg Am 2005;87:2523-36.
|
| 5. | Robert DS. Congenital elevation of the scapula. J Bone Joint Surg Am 1926;8:207-15.
|
| 6. | Mooney JF 3rd, White DR, Glazier S. Previously unreported structure associated with Sprengel deformity. J Pediatr Orthop 2009;29:26-8.
|
| 7. | Jeannopoulos CL. Congenital elevation of the scapula. J Bone Joint Surg Am 1952;34:883-92.
|
| 8. | Sherk HH, Shut L, Chung S. Iniencephalic deformity of the cervical spine with Klippel-Feil anomalies and congenital elevation of the scapula: Report of three cases. J Bone Joint Surg Am 1974;56:1254-9.
|
| 9. | Cavendish ME: Congenital elevation of the scapula. J Bone Joint Surg Br 1972;54:395-408.
|
| 10. | Carson WG, Lovell WW, Whitesides TE Jr. Congenital elevation of the scapula. Surgical correction by the Woodward procedure. J Bone Joint Surg Am 1981;63:1199-207.
|
| 11. | Joe W. Woodward. Congenital elevation of the scapula: Correction by release and transplantation of muscle origins. J Bone Joint Surg Am 1961;43:219-28.
|
| 12. | Rigault P, Pouliquen JC, Guyonvarch G, Zujovic J. Congenital elevation of the scapula in childhood. Rev Chir Orthop 1976;62:5-26.
|
| 13. | Armitage BM, Wijdicks CA, Tarkin IS, Schroder LK, Marek DJ, Zlowodzki M, et al. Mapping of scapular fractures with three-dimensional computed tomography. J Bone Joint Surg Am 2009;91:2222-8.
|
| 14. | Dino Samartzis, Jean Herman, John P. Lubicky, Francis H. Shen. Sprengel's Deformity in Klippel-Feil Syndrome. Spine 2007;32:E512-6.
|
| 15. | Mears DC. Partial resection of the scapula and a release of the long head of triceps for the management of Sprengel's Deformity. J Pediatr Orthop 2001;21:242-5.
|
| 16. | Ahmad AA. Surgical correction of severe Sprengel deformity to allow greater postoperative range of shoulder abduction. J Pediatr Orthop 2010;30:575-81.
|
| 17. | Andrault G, Salmeron F, Laville JM. Green's surgical procedure in Sprengel's deformity: Cosmetic and functional results. Orthop Traumatol Surg Res 2009;95:330-5.
|
| 18. | Masquijo JJ, Bassini O, Paganini F, Goyeneche R, Miscione H. Congenital Elevation of the Scapula Surgical Treatment With Mears Technique. J Pediatr Orthop 2009;29:269-74.
|
| 19. | Wilkinson JA, Campbell D. Scapular osteotomy for Sprengel's shoulder. J Bone Joint Surg Br 1980;62:486-90.
|
| 20. | Zhang ZM, Zhang J, Lu ML, Cao GL, Dai LY. Partial scapulaectomy for congenital elevation of the scapula. Clin Orthop Relat Res 2006;457:171-5.
|
| 21. | Grogan DP, Stanley EA, Bobechko WP. The Congenital undescended scapula surgical correction by the Woodward procedure. J Bone Joint Surg Br 1983;65:598-605.
|
| 22. | Leibovic SJ, Ehrlich MG, Zaleske DJ. Sprengel deformity. J Bone Joint Surg Am 1990;72:192-7.
|
| 23. | McMurtry I, Bennet GC, Bradish C. Osteotomy for congenital elevation of the scapula (Sprengel's deformity). J Bone Joint Surg Br 2005;87:986-9.
|
| 24. | Hensinger RN, Lang JE, Macewen GD. Klippel-Feil syndrome: A constellation of associated anomalies. J Bone Joint Surg Am 1974;56:1246-53.
|
| 25. | Baba H, Maezawa Y, Furusawa N, Chen Q, Imura S, Tomita K. The cervical spine in the Klippel-Feil syndrome: A report of 57 cases. IntOrthop 1995;19;204-8.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7], [Figure 8], [Figure 9]
[Table 1], [Table 2], [Table 3], [Table 4], [Table 5], [Table 6], [Table 7], [Table 8], [Table 9]
| This article has been cited by | | 1 |
Eight Patients With Multiple Bilateral Thoracic Anomalies: A New Syndrome or Bilateral Polandæs Syndrome? |
|
| Nurettin Yiyit,Turgut Isitmangil,Hasan Saygin | | The Annals of Thoracic Surgery. 2014; 97(5): 1758 | | [Pubmed] | [DOI] | | | 2 |
Sprengel Deformity with Bilateral Huge Omovertebra |
|
| Gi Woon Yoon,So Hak Chung | | Journal of the Korean Orthopaedic Association. 2013; 48(4): 319 | | [Pubmed] | [DOI] | |
|
|
|
|



















