| |


 |
| Year : 2014 | Volume
: 8
| Issue : 3 | Page : 76-80 |
|
|
|
|
|
ORIGINAL ARTICLE Long-term functional results and isokinetic strength evaluation after arthroscopic tenotomy of the long head of biceps tendon
Bertram The1, Mike Brutty2, Allan Wang3, Peter T Campbell4, Michael J. C. Halliday4, Timothy R Ackland2
1 Department of Orthopaedic Surgery, Sir Charles Gairdner Hospital, Perth,Australia,
2 School of Sport Science, Exercise and Health, University of Western Australia, Perth, Australia,
3 Department of Orthopaedic Surgery, Sir Charles Gairdner Hospital; School of Sport Science, Exercise and Health, University of Western Australia; Department of Orthopaedic Surgery, Saint John of God Hospitals, Perth, Australia,
4 Department of Orthopaedic Surgery, Saint John of God Hospitals, Perth, Australia,
Correspondence Address:
Bertram The
Molstraat 4a, 3000 Leuven, Belgium
 Source of Support: None, Conflict of Interest: None  | 3 |
DOI: 10.4103/0973-6042.140114

|
|
|
|
| Date of Web Publication | 4-Sep-2014 |
 Abstract Abstract | | |
Introduction: The objective of this study is to evaluate the biomechanical function of the upper arm after arthroscopic long head of biceps (LHB) tenotomy at long-term follow-up.
Materials and methods: Twenty-five male subjects ranging from 30 to 63 years old were evaluated at a mean follow-up of 7.0 years after tenotomy. Bilateral isokinetic testing was performed to obtain peak torque values, as well as total work done throughout the full range of elbow flexion and supination.
Results: Magnetic resonance imaging scans revealed nine unrecognized LHB ruptures in the contralateral arm, leaving 16 subjects to complete the testing protocol. The mean quickDASH score was 8.1 (standard error [SE] 2.5). The mean oxford elbow score was 97.9 (SE 1.6). The tenotomy arm recorded a decrease in peak flexion torque of 7.0% (confidence interval [CI] 1.2-12.8), and a decrease in the peak supination torque of 9.1% (CI 1.8-16.4) relative to the contralateral arm. The total work carried out through the full range of joint motion was reduced in elbow flexion by 5.1% (CI −1.3-11.4) and in forearm supination by 5.7% (CI-2.4-13.9).
Discussion: Maximum strength in elbow flexion and forearm supination is significantly reduced compared with the contralateral arm. However, this impairment is partially compensated for by relatively greater strength sustained through the latter stages of joint motion. This results in comparable total work measurements between the tenotomised and contralateral side, potentially accounting for ongoing high levels of patient satisfaction and clinical function in the long term after LHB tenotomy.
Level of Evidence IV: Case series without comparison group.
Keywords: Biceps tenotomy, isokinetic strength, long-term
How to cite this article:
The B, Brutty M, Wang A, Campbell PT, Halliday MJ, Ackland TR. Long-term functional results and isokinetic strength evaluation after arthroscopic tenotomy of the long head of biceps tendon. Int J Shoulder Surg 2014;8:76-80 |
How to cite this URL:
The B, Brutty M, Wang A, Campbell PT, Halliday MJ, Ackland TR. Long-term functional results and isokinetic strength evaluation after arthroscopic tenotomy of the long head of biceps tendon. Int J Shoulder Surg [serial online] 2014 [cited 2016 Aug 23];8:76-80. Available from: http://www.internationalshoulderjournal.org/text.asp?2014/8/3/76/140114 |
| Introduction | |  |
Pathology of the long head of biceps (LHB) is a common source of shoulder pain. [1],[2],[3] Arthroscopic tenotomy is commonly performed although this may lead to distal migration of the biceps muscle causing a cosmetic Popeye deformity, aching arm pain, and concerns for impaired muscle function during elbow flexion or forearm supination activity. Duff and Campbell [4] using a hand held dynamometer, reported no objective difference in strength at short term follow-up after LHB tenotomy, although 15% of patients reported a subjective sense of significant weakness. Shank et al. [5] using Cybex isokinetic strength testing of 17 patients at a minimum of 6 months after arthroscopic LHB tenotomy, reported no flexion or supination strength loss relative to a group of patients with biceps tenodesis. However, long term studies of the strength changes following LHB tenotomy are lacking. Mariani et al.[6] evaluated spontaneous LHB rupture at a mean of 4.6 years after injury and reported a loss of elbow flexion strength of 8%, and supination strength of 21%. Further biomechanical parameters of muscle function were not evaluated including total work done throughout the full range of joint motion. If arthroscopic tenotomy of LHB is to be a recommended treatment option, then more extensive biomechanical evaluation of biceps function is required and at long-term follow-up from surgery, especially in the younger patient who needs to remain physically active.
Our hypothesis is that in this higher demand patient cohort, good clinical function persists with no loss of biceps strength as assessed by isokinetic dynamometry in the long term following surgery.
| Materials and methods | | |
The study protocol was approved by the Institutional Human Ethics Committee.
Male patients who had undergone an arthroscopic LHB tenotomy between the ages of 30 and 65 more than 4 years previously were identified. We excluded more elderly male patients and female patients who are less likely to be engaged in manual labor or heavy sports than working age men, and who are less likely to be symptomatic from a tenotomy of the LHB. Furthermore, we excluded patients who had neurological conditions, elbow or wrist pathology documented on either side, or who were unable to undergo magnetic resonance imaging (MRI) scans. This resulted in an initial study sample of 25 male patients of which nine were excluded after establishing a contralateral spontaneous (LHB tendon [LHBT]) tear, leaving 16 males with a mean age of 49 years old (range: 30-63).
All subjects fulfilling the inclusion criteria were assessed clinically for the presence of a Popeye muscle deformity. The quickDASH and oxford elbow score evaluating pain and function were completed.
A screening MRI was performed bilaterally using a Siemens Avanto 1.5T scanner (Siemens Medical Solutions, Erlangen, Germany). Patients were positioned supine in the scanner and arms placed alongside the body in neutral rotation. Limited scans were performed of both arms simultaneously. T1 axial weighted images were evaluated for the presence or absence of an intact LHB in the contralateral arm. Subjects who lacked an intact LHB in the contralateral arm due to a previous unrecognised spontaneous rupture were further excluded from the study.
Strength test
We performed strength measurements using a Biodex systems three device (Biodex Medical Systems, Shirley, NY, USA) on both the LHB tenotomy and contralateral arm. Isokinetic flexion and supination strength were measured at 120°/s through the full range of elbow joint flexion, then forearm supination.
The Biodex machine and patient positioning is shown in [Figure 1]. The starting position for the flexion protocol is in full extension (0°), with the forearm in 90° of supination. For the supination tests the starting position was in 90° pronation with the elbow in 90° flexion and the arm resting at the side. | Figure 1: The setup for the strength tests using the Biodex machine is shown
Click here to view |
Four trials of concentric motion were performed, and the mean values were used for analysis. The peak torque value for both flexion and supination were recorded. In addition, the total work done through the full range of joint motion (which is the area under the curve, after plotting torque values throughout the entire angular motion) was recorded. Values of the LHBT tenotomy arm were compared with the contralateral arm [Figure 2]. Wittstein et al.[7] has demonstrated that the dominant and nondominant upper extremity have equivalent peak torque for both flexion and forearm supination. The normal contralateral arm can therefore be used as a control for isokinetic evaluation of biceps function, without adjusting results for hand dominance.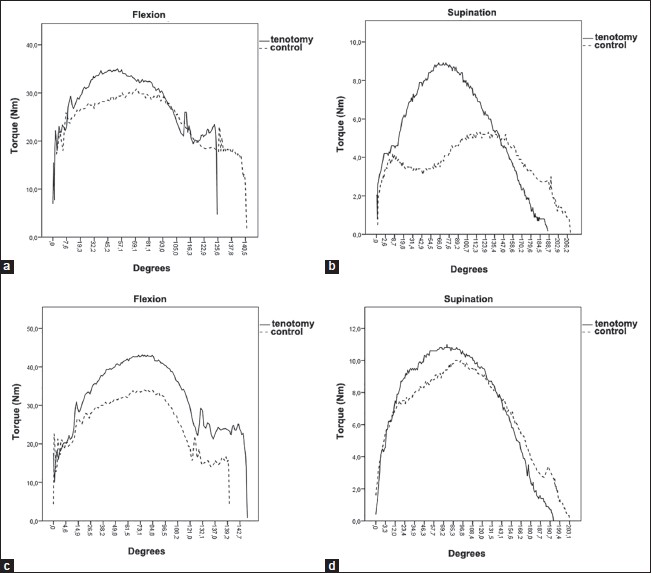 | Figure 2: Torque curves of two patients with marked strength of loss are displayed. Loss of torque can be seen in the early range of motion for all graphs. The first patient shows successful "catching-up" for both flexion (a) and supination (b) in the second half of the graph with partial compensation in the end range, where his tenotomised side shows higher torque values than the contralateral side. The second patient shows similar characteristics for supination (d), but not for fl exion (c)
Click here to view |
Statistical analysis
Differences between LHB tenotomy and contralateral arm in peak torque, work done through range of motion, and maximum power generated, were analysed and absolute values, and percentage differences between sides with 95% confidence intervals (CI) were recorded. Both the CI as well as P values are reported. All analyses were performed using SPSS (IBM SPSS statistics 20.0, Chicago, Illinois, USA).
| Results | | |
Twenty-five subjects fulfilled the inclusion criteria and agreed to participate in this study. Following screening MRI, nine subjects were noted to have an unrecognized spontaneous LHB rupture on the contralateral arm, and these patients were excluded from the study.
The 16 subjects were evaluated at a mean follow-up of 7 (range: 4-11) years after arthroscopic LHB tenotomy. Surgery was performed for LHB subluxation or partial tear identified at the time of rotator cuff decompression and repair in 89%, or as a treatment for superior labrum, anterior and posterior tear in 11%. All patients had fully completed their rehabilitation program.
At review, patient reported clinical function was good. The mean quickDASH score was 8.1 (standard error [SE] 2.5). The mean oxford elbow score was 97.9 (SE 1.6). None complained of cramping arm pain. Six patients had clinical evidence for a Popeye muscle deformity.
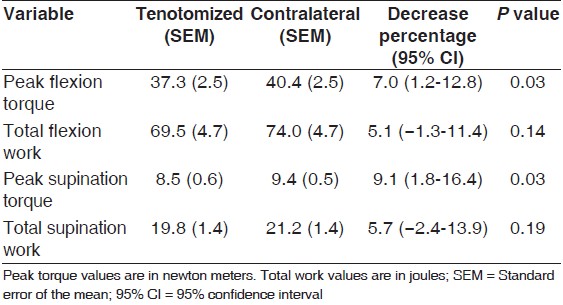
The isokinetic testing results for peak torque and total work done are shown in [Table 1].
Significant strength reductions were noted, with peak flexion torque decreased 7.0%, and peak supination torque decreased by 9.1%, compared with the contralateral arm with a confirmed intact LHBT.
Total work done in flexion and also supination were decreased by approximately 5% compared with the contralateral limb. However, this was not a consistent finding. Patients with more severe relative loss in peak torque displayed a late "catch-up" in strength at higher angles of joint motion [Figure 2]. The LHB tenotomy arm maintained relatively higher levels of torque as the joint approached end range motion. The area under the curve representing total work done through full range of motion, is not significantly different from the contralateral arm in flexion or supination [Table 1]. No differences were found between the group with and the group without a Popeye deformity [Table 2].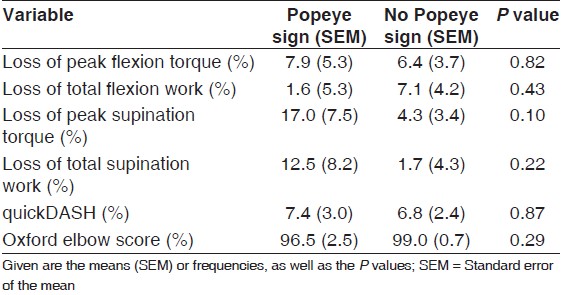 | Table 2: Differences between patients with and without a Popeye deformity are shown
Click here to view |
| Discussion | | |
Recent studies have reported well clinical outcomes and high levels of patient satisfaction in the short term after arthroscopic LHB tenotomy. [4],[6],[8],[9] This study aimed to evaluate biomechanical function of the biceps in the long-term after surgery. Longer term review allows potential compensation of LHB tenotomy to occur by hypertrophy of other muscle groups (e.g., short head of biceps, brachialis, brachioradialis, and supinator muscles). Conversely, potential deterioration in function may occur in the long-term due to progressive biceps atrophy. Mariani et al. [6] evaluating spontaneous rather than surgical LHB deficiency at mean 4.6 years follow-up reported substantial deficits in both elbow flexion and forearm supination strength. If arthroscopic LHB tenotomy is to remain a satisfactory treatment option, then long-term evaluation is necessary, especially in younger patients who wish to remain active and strong in the long-term.
The strengths of this study are that only males of working age who were active in work and sport were evaluated. The mean time from surgery was 7.0 years representing the longest follow-up to the authors' knowledge for arthroscopic LHB tenotomy. Furthermore, a screening MRI scan of the opposite arm was used to confirm the validity of the contralateral arm as a control for biomechanical testing.
This study has confirmed that patient reported clinical function remains very good at 7.0 years after arthroscopic LHB tenotomy. However, this study also shows a significant reduction in peak torque for both elbow flexion and forearm supination. If middle aged male subjects are substantially weaker, why is reported clinical function good and patient satisfaction so high? This study shows a relative preservation of the total work done in both elbow flexion and forearm supination through the whole range of joint motion. While the area under the curve is still less in the tenotomy side, the relative loss of work done is reduced via a late "catch-up" where strength is preserved at higher angles of joint motion. Although purely speculative, it might be a result of differences in recruitment characteristics (where the compensatory muscle groups become effective at a slightly later moment throughout the arc of motion). Therefore with tasks employing full joint motion, e.g., using a screw driver with a full supination motion, or sports such as rowing, which require elbow motion from full extension to flexion, the impairment from peak torque loss is partially compensated for, and patients may not recognise a disability.
The major weakness of the study is the small patient numbers. Only 25 eligible patients were identified in the practices of two surgeons and who were available for review at a minimum of 4 years from surgery. Of these, nine patients became ineligible after bilateral screening MRI scans revealed an unrecognised LHB rupture in the contralateral arm. Despite only 16 subjects meeting the inclusion criteria and being available for long-term follow-up, significant deficits were still identified in peak torque of elbow flexion and forearm supination. Increased study numbers may further have allowed identification of biomechanical difference in patients with a prominent Popeye muscle deformity compared to those patients with normal muscle contour.
A further possible weakness is the selection of the patient rated outcome measures to evaluate clinical function. The oxford elbow score is an elbow specific questionnaire and consists of 12 items distributed over three domains : p0 ain, function and social. The quickDASH assesses function of the whole upper extremity. Both these instruments have not been specifically validated for biceps dysfunction. For example, the quickDASH has items such as parasthesia that is unlikely to be relevant to biceps dysfunction. However, the quickDASH is in widespread use for the evaluation of arm and elbow pathology and both questionaires include items that are relevant to biceps function.
| Conclusion | | |
This study reports that at long term follow-up of arthroscopic LHB tenotomy in active male patients of working age, significant reductions in peak elbow flexion and forearm supination strength occurs. However, clinical function remains good, and this paradox may be accounted for by compensatory muscle changes in the upper arm which preserve power and maintain work done through the full range of joint motion.
| References | | |
| 1. | Boileau P, Ahrens PM, Hatzidakis AM. Entrapment of the long head of the biceps tendon: The hourglass biceps - A cause of pain and locking of the shoulder. J Shoulder Elbow Surg 2004;13:249-57.  |
| 2. | Sethi N, Wright R, Yamaguchi K. Disorders of the long head of the biceps tendon. J Shoulder Elbow Surg 1999;8:644-54. |
| 3. | Szabó I, Boileau P, Walch G. The proximal biceps as a pain generator and results of tenotomy. Sports Med Arthrosc 2008;16:180-6. |
| 4. | Duff SJ, Campbell PT. Patient acceptance of long head of biceps brachii tenotomy. J Shoulder Elbow Surg 2012;21:61-5. |
| 5. | Shank JR, Singleton SB, Braun S, Kissenberth MJ, Ramappa A, Ellis H, et al. A comparison of forearm supination and elbow flexion strength in patients with long head of the biceps tenotomy or tenodesis. Arthroscopy 2011;27:9-16. |
| 6. | Mariani EM, Cofield RH, Askew LJ, Li GP, Chao EY. Rupture of the tendon of the long head of the biceps brachii. Surgical versus nonsurgical treatment. Clin Orthop 1988; (228):233-9. |
| 7. | Wittstein J, Queen R, Abbey A, Moorman CT 3 rd . Isokinetic testing of biceps strength and endurance in dominant versus nondominant upper extremities. J Shoulder Elbow Surg 2010;19:874-7. |
| 8. | Deutch SR, Gelineck J, Johannsen HV, Sneppen O. Permanent disabilities in the displaced muscle from rupture of the long head tendon of the biceps. Scand J Med Sci Sports 2005;15:159-62. |
| 9. | Koh KH, Ahn JH, Kim SM, Yoo JC. Treatment of biceps tendon lesions in the setting of rotator cuff tears: Prospective cohort study of tenotomy versus tenodesis. Am J Sports Med 2010;38:1584-90. |
[Figure 1], [Figure 2]
[Table 1], [Table 2]
|