| |


 |
| Year : 2016 | Volume
: 10
| Issue : 1 | Page : 41-43 |
|
|
|
|
|
CASE REPORT Early asymptomatic intrathoracic migration of a threaded pin after proximal humeral osteosynthesis
Paola Cerruti1, Tony Mangano2, Marcello Giovale2, Ilaria Repetto1
1 Department of Orthopaedics and Traumatology, University of Genova, School of Medicine, Padiglione 40, Largo Rosanna Benzi 10, Genova, Italy
2 GSL, Albenga Orthopedic Center, Santa Maria di Misericordia Hospital, Viale Martiri Della Foce, Albenga, Italy
Correspondence Address:
Ilaria Repetto
Department of Orthopaedics and Traumatology, University of Genova, School of Medicine, Padiglione 40, Largo Rosanna Benzi 10, 16132 Genova
Italy
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/0973-6042.174520
 |
|
|
|
| Date of Web Publication | 20-Jan-2016 |
 Abstract Abstract | | |
Pinning with metallic wires is a suitable therapeutic option for proximal humeral fractures. Loosening and migration of such devices from this site is uncommon. Despite infrequently occurring, however, the literature reports dramatic and potentially lethal complications related to wires dislocation. A 69-year-old woman underwent closed reduction and fixation of a proximal 3-part humeral fracture by mean of two retrograde Kirschner wires and one anterograde threaded pin. One month after surgery, during a routine follow-up control, it was diagnosed the migration of the threaded pin in the left lung parenchyma. In the meantime, the only symptom the patient complained was an episodic intercostal pain of mild intensity, with referred onset 1 week after surgery. The migrated pin was removed through thoracoscopic approach in the emergency setting, without intra- or post-operative complications. Only a few authors reported similar complications after fixation of proximal humeral fractures. Immediate surgical removal of the device is always mandatory. When considering pinning fixation for shoulder girdle's fractures, orthopedic surgeons should take into account the risk for wire dislocation, and take up adequate precautions during surgery and follow-up control visits.
Keywords: Foreign body migration, Kirschner wire, proximal humeral fracture, thoracoscopy, threaded wire
How to cite this article:
Cerruti P, Mangano T, Giovale M, Repetto I. Early asymptomatic intrathoracic migration of a threaded pin after proximal humeral osteosynthesis. Int J Shoulder Surg 2016;10:41-3 |
| Introduction | |  |
Kirschner wires (K-wires) and threaded wires are widely used devices for fixation of proximal humeral fractures. [1] Cases of metallic wire migration through the thoracic cavity have been described since 1943. [2] A more recent review of the literature has shown intrathoracic migration in 68 patients. [3] To our knowledge, most of the cases described in the literature were diagnosed with substantial delay, when an organ damage had occurred. We report a case of asymptomatic early intrathoracic migration of a percutaneously inserted anterograde threaded wire used in the setting of pinning fixation of a 3-part humeral fracture. Technical errors and risk factors have been analyzed and discussed.
| Case report | | |
A 69-year-old woman was admitted to the emergency department after an accidental fall. She presented with left shoulder pain and functional impairment. Clinical history included essential hypertension and obesity. Traditional X-ray series and computed tomography (CT) scan with three-dimensional reconstruction were performed. Examinations showed a 3-part fracture of the proximal left humerus, accounting to the Neer's classification (AO/ASIF: 11-B2) [Figure 1]a and b]. Two days after patient acceptance to our department, fracture was treated by closed reduction and fixation with two retrograde K-wires and one threaded wire, by mean of a modified " en palmière" technique: The first two wires were retrograde nonthreaded bent wires inserted at the deltoid "V" level, while the latter was an anterograde threaded wire percutaneously introduced to fix the great tuberosity [Figure 1]c and d]. Two days after surgery, the patient was discharged from the hospital. One month after surgery, the patient came back for routine clinical and radiographic control, to evaluate the fracture healing and eventually plan the wires removal. In that setting, she referred about global well-being and no pain at the shoulder. X-rays demonstrated the intrathoracic migration of the threaded wire used for tuberosity fixation [Figure 2]a and b]. A complementary CT scan was immediately performed to better show the spatial relationship between the wire and intrathoracic vital organs. It revealed the device was migrated through the fifth intercostal space to the left lung parenchyma, without the signs of pneumothorax, nor bleeding [Figure 2]c and d]. She was extensively interviewed and investigated for any symptom or sign. She only referred about episodic intercostal mild pain that onset 1 week after surgery and was elicited by a cough. Due to low severity of the symptom, it was completely underestimated by the patient. Physical examination, vital parameters, and blood examination resulted normal. The patient was immediately managed by mean of video-assisted thoracoscopic approach to remove the migrated wire from the lung parenchyma. Intraoperatively, a fibrin-coated spot was identified on the lung surface and excised. This allowed the foreign body to be visualized and easily removed [Figure 3]. Neither parenchymal bleeding nor pneumothorax was observed. A chest drain tube was inserted, and antibiotic prophylaxis was administered. The postoperative outcome was free of complications, and the patient was discharged 3 days after surgery with a normal chest radiogram. One month after surgery, the patient underwent new thoracic and left shoulder X-rays, confirming the healing of the shoulder fracture and the absence of radiographically evident sequelae about the lung. A specialist consultation by thoracic surgeons was performed, assessing the complete recovery of lung function without complications or negative outcomes.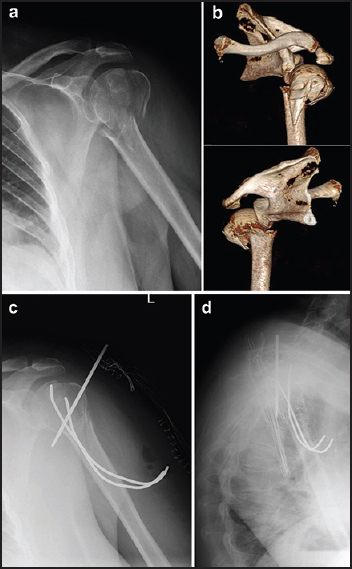 | Figure 1: (a and b) Preoperative X-rays and three-dimensional computed tomography studies demonstrating a 3-part proximal humeral fracture; (c and d) Postoperative X-rays in anteroposterior and transthoracic views
Click here to view |
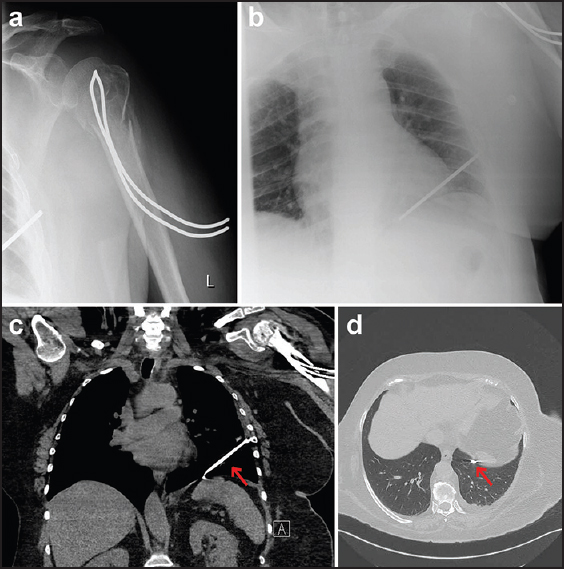 | Figure 2: (a and b) One month follow-up X-ray control showing migration of the anterograde threaded wire; (c and d) Computed tomography study performed to defi ne the relationship between the wire and intrathoracic vital organs, demonstrating the wire close to the diaphragm and posterior and inferior to the left ventricle, without organ damage
Click here to view |
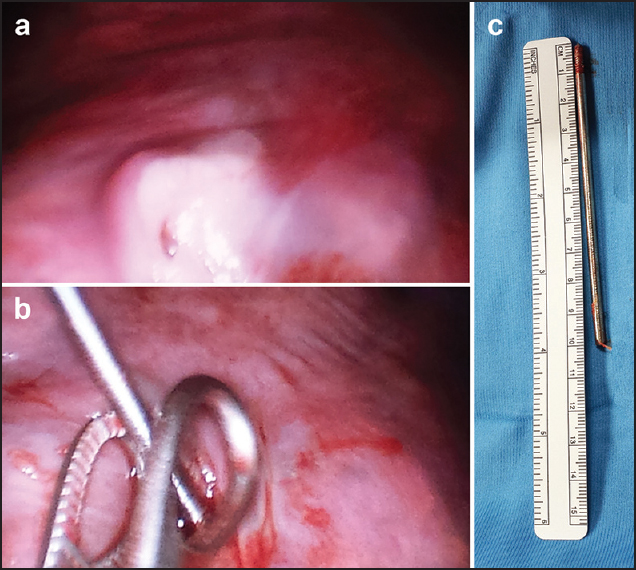 | Figure 3: (a) Fibrin-coated entry point of the wire in the left lung; (b) Thoracoscopic views of the wire removal; (c) The removed wire
Click here to view |
| Discussion | | |
Thecases of metallic wire migration through the thoracic cavity have been described since 1943: Lyons and Rockwood described 49 cases of K-wire migration in 47 patients, reported over 38 years, from 1943 to 1981. [2] A more recent review of the literature has shown intrathoracic migration in 68 patients. [3] Most of these cases dealt with early migrations in which the time between the introduction of the wires and the migration to the thorax varied from 1 to 21 days. [2] Many predisposing or contributing factors to pin dislocation could be identified, such as the breathing movements, the intrathoracic negative pressure, the gravitational force, the regional bony re-absorption, the freedom of shoulder movements, and inadequate wire positioning.However, a unique reproducible causal mechanism has not been described yet. [2],[3],[4],[5] Some authors reported about axillary migration with or without nervous lesions and intrathoracic migration often followed by devastating sequelae such as pneumothorax, hemothorax, lung consolidation, and hemoptysis; others described often fatal cardiac and vascular perforation, while in two cases, an intraabdominal migration through diaphragm with or without intestinal perforation was reported. Migration of the metallic wire could be completely asymptomatic, dangerously delaying the diagnosis. Migration could become evident when an important organ lesion has already occurred, and this negatively affects the outcome and survival. Similarly to the case we described, only a few authors reported occasional diagnosis during programmed X-ray controls: The fortuitous finding allowed a prompt management, then preventing further complications to the patient. Of note, several cases of K-wire migration in the literature involved an anterograde pin often used for great tuberosity fixation. In such circumstances, the migration could be facilitated by secondary fragment dislocation, partial bony re-absorption of the humeral head, preexisting poor bone mineral density, and micro-movements are occurring despite the immobilization of the shoulder. All of these factors can dramatically affect the pin stability. In thiscase too, the migration involved the anterograde wire: Despite being a threaded wire, an improper positioning should be taken into account as a contributing factor to the complication to occur. The thread of the wire appeared not properly anchored to the bone, vanishing the significance of the thread itself, and the possibility the wire engaged the inferior fracture line is plausible, with further reduction of hardware stability. Fixation techniques for proximal humeral fractures using metallic wires represent a suitable and minimally invasive therapeutic option, but some precautions should be taken to prevent highly dangerous hardware loosening and migration. First, it is warmly advised bending the extremities of the wires to involve the periosteum, or positioning the wires with percutaneous technique avoiding, if possible, anterograde wire positioning; for tuberosity fixation, the use of a cannulated screw should be considered. During fixation, pins positioning should be accurate and, after pinning, hardware stability should be always checked through dynamic maneuvers. Despite attractive, the use of pinning techniques should be carefully discussed in the setting of complex and comminuted humeral fractures, especially in cases of elder patients with presumably low bone quality and low compliance to the immobilization regimen. Moreover, it is worth submitting patients to close periodic follow-up visits and standard shoulder X-ray controls to detect eventual early migration, also in the absence of clinical signs and symptoms suggestive for complications. If any sign of hardware migration is detected, a thorough radiological and CT study should be made, and the surgical removal should be promptly performed. The surgeon should always keep in mind the imminent risk of devastating organ damages and the reported risk, as well, of displacements of considerable distance in only a few hours after the diagnosis. The video-assisted thoracoscopic approach is a useful solution for retrieving and removing an intrapulmonary migrated pin.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Kapandji A. Osteosynthesis using the "palm-tree" nail technic in fractures of the surgical neck of the humerus. Ann Chir Main 1989;8:39-52.  |
| 2. | Lyons FA, Rockwood CA Jr. Migration of pins used in operations on the shoulder. J Bone Joint Surg Am 1990;72:1262-7. |
| 3. | Calkins CM, Moore EE, Johnson JL, Smith WR. Removal of an intrathoracic migrated fixation pin by thoracoscopy. Ann Thorac Surg 2001;71:368-70. |
| 4. | Freund E, Nachman R, Gips H, Hiss J. Migration of a Kirschner wire used in the fixation of a subcapital humeral fracture, causing cardiac tamponade: Case report and review of literature. Am J Forensic Med Pathol 2007;28:155-6. |
| 5. | Cameliere L, Rosat P, Heyndrickx M, Le Rochais JP, Icard P. Migration of a Kirschner pin from the shoulder to the lung, requiring surgery. Asian Cardiovasc Thorac Ann 2013;21:222-3 |
[Figure 1], [Figure 2], [Figure 3]
|














