|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2013 | Volume
: 1
| Issue : 1 | Page : 15-19 |
|
Knowledge and perception of mother to child transmission of human immunodeficiency virus among South Eastern Nigerian pregnant women
Joseph C Umeobika, Ifeanyichukwu U Ezebialu, Cyril T Ezenyeaku, Lawrence C Ikeako
Department of Obstetrics and Gynecology, Anambra State University Teaching Hospital, Awka, Nigeria
| Date of Acceptance | 19-Apr-2013 |
| Date of Web Publication | 16-Aug-2013 |
Correspondence Address:
Joseph C Umeobika
Department of Obstetrics and Gynecology, Anambra State University Teaching Hospital, Awka
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |

Context: The success of prevention of mother to child transmission (PMTCT) of human immunodeficiency virus (HIV) requires the cooperation of the mother. The level of cooperation may depend on the extent of knowledge of pregnant women on HIV/acquired immunodeficiency syndrome (AIDS), its mode of transmission to the child and ways of preventing it. Aim: The aim of this study was to evaluate the knowledge and perception of mother to child transmission (MTCT) of HIV among pregnant women receiving antenatal care in a university teaching hospital in South Eastern Nigeria. Settings and Design : This is a cross-sectional study in a teaching hospital. Subjects and Methods: A cross-sectional survey of 396 antenatal attendees, using a pre-tested, and interviewer administered questionnaires. Statistical Analysis Used: Data were analyzed using the Epi Info statistical software and presented as percentages and tables. Results: All the respondents were aware of HIV/AIDS. The main sources of information were health workers (72.7%), radio (62.6%) and television (55.5%). Majority (94.9%) were aware that HIV can co-exist with pregnancy, but only 73.4% were aware of MTCT. Breast feeding (75.7%), transplacental (56.2%), and vaginal delivery (36.6%) were the main identified routes of transmission to the child. Some respondents (21%) however believe that cesarean section has a higher rate of vertical transmission relative to vaginal delivery. Giving the mother antiretroviral drugs (81.7%) and avoiding breast feeding (49%) were the major preventive ways identified by respondents. Some however believe that mixed feeding is one of the modes of preventing MTCT of HIV/AIDS. Conclusion: The awareness and knowledge of HIV/AIDS in the study population is high, but the knowledge and perceptions of PMTCT, is comparatively low. Keywords: Antenatal attendees, human immunodeficiency virus/acquired immunodeficiency syndrome, knowledge, mother to child transmission
How to cite this article:
Umeobika JC, Ezebialu IU, Ezenyeaku CT, Ikeako LC. Knowledge and perception of mother to child transmission of human immunodeficiency virus among South Eastern Nigerian pregnant women. J HIV Hum Reprod 2013;1:15-9 |
How to cite this URL:
Umeobika JC, Ezebialu IU, Ezenyeaku CT, Ikeako LC. Knowledge and perception of mother to child transmission of human immunodeficiency virus among South Eastern Nigerian pregnant women. J HIV Hum Reprod [serial online] 2013 [cited 2017 Apr 5];1:15-9. Available from: http://www.j-hhr.org/text.asp?2013/1/1/15/116536 |
| Introduction | |  |
Human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) pandemic remains a major public health problem of our time that requires a priority attention. Although the first case of this disease was reported in Nigeria in 1986. [1] It was until 1991 that the first attempt was made to assess the Nigerian HIV/AIDS situation. The prevalence of HIV in Nigeria has increased over time from 1.8% in 1991 to a peak of 5.8% in 2001. [2] By the beginning of 2009, it was estimated that there were 2.95 million Nigerians living with HIV. [3] Nearly, 80% of all transmissions are from heterosexual sexual intercourse, about 10% are from mother to child transmission (MTCT) while another 10% is from infected blood and unsterilized sharps. [4] Each year, about 75,000 babies are born with HIV in Nigeria. [5] In 2007 the number of children living with HIV was estimated at 220,000. [6] This has however risen to 360,000 as at 2010. [7] Over 90% of this childhood infection is acquired by MTCT. [8] Without intervention the transmission rate can be as high as 20-30%, but with appropriate intervention this risk can be reduced to about 1%. [9]
In June 2001, the United Nations General Assembly Special Session (UNGASS) resolved to reduce the proportion of infants infected with HIV by 20% by 2005 and 50% by 2010. [10] In line with this, the national AIDS policy had a goal of reducing the transmission of HIV through MTCT by 50% by the year 2010 and to increase access to HIV counseling and testing (HCT) services by 50% by the same year. [8] This led to the production of the national prevention of mother to child transmission (PMTCT) guideline in 2001 August. This became operational in July 2002 with a total of six centers in the country. [11] Subsequently, the number of sites kept rising as the burden of patients become heavier on the existing facilities. ANSUTH, Awka is one of the existing centers in the South East of Nigeria. Despite all these efforts to strengthen PMTCT interventions, only 5.3% of HIV positive women were receiving antiretroviral (ARV) drugs to reduce the risk of MTCT as at 2007. By 2009 the figure however rose to 22%, which is still below the universal access targets aiming at 80% coverage. [12] This has however dropped to 11% in 2011. [13]
From the foregoing, it is clear that the number of children living with HIV is increasing. This rise in the number of children born with HIV could partly be due to poor knowledge, attitude, and negative perception about HIV and PMTCT among pregnant women. This study was designed to assess the level of knowledge of HIV and PMTCT among women. Information obtained from it will influence the education and counseling of the patients and the community. This will ultimately influence the patient's compliance to PMTCT program thereby reducing the number of children born with HIV in the society.
| Subjects and Methods | | |
The study population included consenting consecutive pregnant women receiving antenatal care services at Anambra State University Teaching Hospital, Awka between May 2012 and August 2012. The study was approved by the Ethical Committee of ANSUTH, Awka. ANSUTH is a tertiary health facility recently upgraded from a secondary health facility. It serves as a referral center for the state and environs. Antenatal clinics are held 4 days of the week with Wednesday being the booking clinic. The average attendance is between 50-80 persons per day with about 30 new patients per week. About 784 patients attended antenatal within the study period. The potential participants in the study received information on the scope and objectives of the study and consenting women were enrolled. A total of 396 women were interviewed using the structured pre-tested researcher administered questionnaires. The sample size was calculated based on an assumed proportion of 50% knowledge of PMTCT using the formula: N = z 2 pq/d 2 (z = Standard normal deviation at 95% confidence interval = 1.96, P = Proportion in the target population estimated to have knowledge of HIV and PMTCT = 0.50, q = 1, P = 0.5 and d = Precision limit = 0.05).
The questionnaire was pre-tested among 30 patients attending the postnatal clinic for clarity, completeness, and average time to complete it. Following this, some amendments were made before the study was commenced. The questionnaire sought information on socio-demographic characteristics, knowledge, and perception of HIV/AIDS, sources of information, knowledge on MTCT of HIV and HIV counseling and testing. The data were coded and analyzed using the Epi Info software version 3.5.4 (Center for Disease Control). Chi-square was used for the test of association between variables and P value <0.05 was considered significant at 95% confidence interval.
| Results | | |
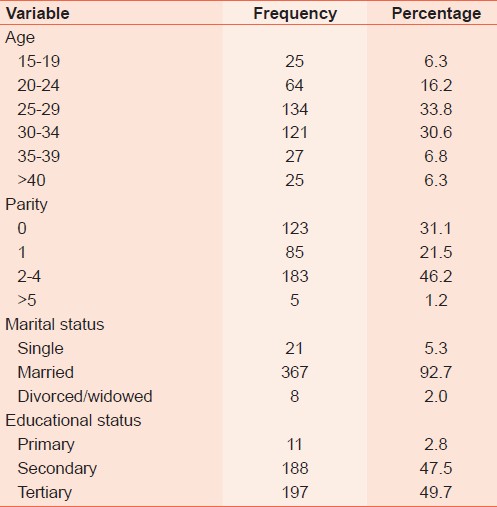
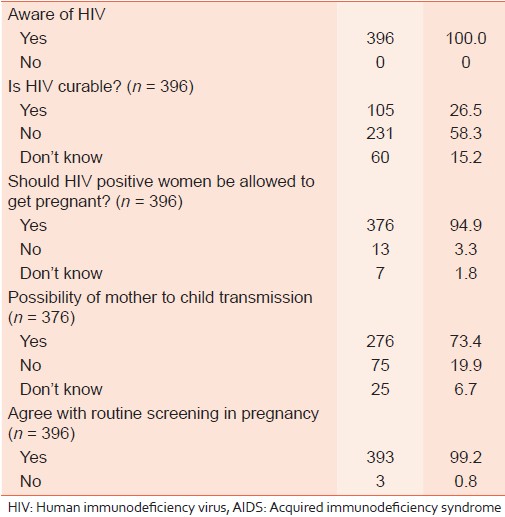
The mean age of the respondents was 29 6 years while the mean parity was 2 1. Majority 367 (92.7%) were married. All the respondents had formal education. One hundred and ninety-seven (49.7%) had tertiary education, 188 (47.5%) had secondary education and 11 (2.8%) had primary education. The socio-demographic profiles of the respondents are shown in [Table 1]. All the respondents had prior knowledge of HIV/AIDS and 26.5% (n = 105) felt that HIV was curable. Regarding the routes of transmission of HIV/AIDS, 352 (88.9%) identified sexual intercourse while 320 (80.8%) and 284 (71.7%) identified blood transfusion and sharing of sharp objects respectively. Saliva and mosquito bites were identified as possible routes of transmission by 76 (19.2%) and 32(8.1%) respondents respectively. The sources of information on HIV are shown in [Figure 1].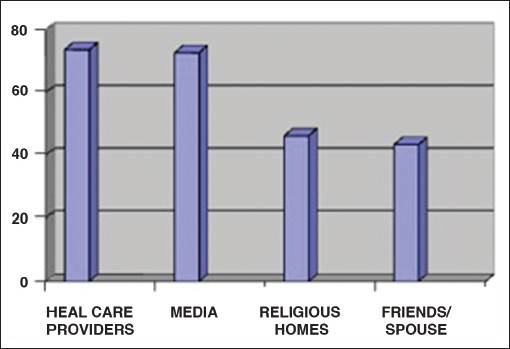 | Figure 1: Sources of information on human immunodeficiency virus in percentage (n = 396). *The total percentage is more than 100 because some respondents had multiple sources
Click here to view |
A total of 376 (94.9%) respondents agreed that women who are HIV positive should be allowed to become pregnant if they choose to whereas 73.4% (n = 276) were aware of MTCT of HIV. Again 91.2% (n = 361) were aware of interventions for the PMTCT of HIV. A total of 393 (99.2%) respondents agreed with a policy of screening for HIV in pregnancy, whereas 3 (0.8%) felt it was not necessary. On the issue of disclosing a positive result to the family members, 269 (67.9%) would like to inform their family members while 127 (32.1%) would not. These are depicted in [Table 2].
| Discussion | | |
Assessment of the level of awareness of HIV/AIDS in this study showed that all the respondents were aware of the disease. This is encouraging and may be attributed to the high level of education of the study population. Similar high level of awareness has been reported at Onitsha [14] and Nnewi [15] in Nigeria and Addis Ababa [16] in Ethiopia. With this high level of awareness one would have expected a low prevalence of HIV/AIDS in pregnant women. This however is not so going by the 2010 sentinel survey with prevalence of 4.1% in which pregnant women were the participants. [17] This implies that awareness is not the only factor influencing HIV/AIDS spread. Risk perception and other factors may have strong roles to play in this, hence the need for further studies.
Health workers, radio, television, and churches were the major sources of their information. A reasonable number of them also got their information from newspapers and posters. This possibly has to do with their level of education since the majority of them can read printed materials. This finding is quite unlike those observed in Lagos [18] and Nnewi [15] Nigeria where the information from health workers, newspapers, and posters were low. This study population with high education level is also likely to go to proper health facilities when they are sick; hence, the higher information from health workers. This is very encouraging and these communication outlets should be reinforced and modified to accommodate other information on HIV/AIDS apart from mere awareness creation. It is amazing that a reasonable number (26.5%) of respondents believe that HIV/AIDS is curable despite their level of education. It is true that with adequate ARV treatment the viral load can be reduced to a very low level, but this does not translate to complete cure of the disease. This is a wrong belief that needs urgent attention if the dream of HIV/AIDS elimination is to be realized. This is one of the aspects the health workers and other communication outlets should include in their awareness campaign on HIV/AIDS.
The responses also showed that sexual intercourse is the most common route of transmission (88.9%) followed by transmission through blood transfusion and sharing of sharp objects. This agrees with findings in Nnewi, [15] Lagos [18] and Addis Ababa. [16] The above knowledge did not outweigh the fact that some of the respondents indicated that saliva and mosquito bites could be possible modes of transmission/spread of HIV/AIDS. This emphasizes the existence of poor understanding of the mode of transmission among other factors that drive the spread of this disease in Nigeria. A high proportion of the respondents (94.9%) agree that HIV can co-exist with pregnancy, but only 73.4% know of possibility of PMTCT. This gap of 21.5% is very significant and will definitely impact negatively on the success of PMTCT. This is similar to the findings from Nnewi survey. [15] The specific knowledge of the routes or modes of transmission to the child is however higher than what was found in Nnewi [15] especially for breastfeeding, placental transfer, and vaginal delivery.
However, it is disturbing that some respondents have the erroneous believe that the child could get HIV through cesarean section (c/s) more than through vaginal delivery. This wrong perception should be corrected as it can lead to refusal of elective c/s when it is necessary for PMTCT. It is known that elective c/s in a pregnant HIV positive woman that did not take ARV drugs appropriately or with high viral load can reduce the risk of transmission by over 50% compared with vaginal delivery. [19] It is also known that prolonged rupture of fetal membrane (PROM) beyond 4 hours before delivery increases the risk of MTCT of HIV. [19] However, in this study only 6.9% are aware that PROM can lead to MTCT. It is thus important that this be included in the health talks at antenatal clinics as some of the HIV positive pregnant women may rupture membranes at home without bothering to present to the health facility until contraction starts. There is also a high acceptance of routine HCT (99.2%) in this study. This is encouraging since HCT is the entry point into PMTCT program and hence the bedrock for its success in any institution.
About 32.1% of the respondents will not be willing to disclose their status to their family members if they test positive to HIV. This class of people will require detailed counseling on feeding options because they cannot adhere to exclusive breast milk supplement (BMS) option. They are most likely to breastfeed their babies in the presence of their family members and continue with BMS later just to maintain the secret. This mixed feeding increases the risk of MTCT. Such patients will benefit from exclusive breast feeding and should be counseled in that direction.
A reasonable proportion (81.7%) are aware that taking ARV drugs during pregnancy can prevent MTCT, but the general knowledge of other methods of PMTCT were below average. This is similar to some extent to the outcome in Nnewi. [15] It is noteworthy that some respondents believe that mixed feeding is a method of PMTCT. This is a wrong impression as mixed feeding increase the risk of MTCT of HIV. [19]
In conclusion, the awareness and knowledge of HIV/AIDS from this study is high, but the knowledge and perceptions of PMTCT is still below expectation if the UNGASS and national PMTCT scale up targets are to be realized. There is a need to study the HIV risk perception among pregnant women and to reinforce the communication outlets to include aspects of HIV/AIDS such as routes of transmission, routes of MTCT, and methods of PMTCT in their awareness campaign. All these will help in the successful implementation of PMCT program in particular and control of HIV/AIDS in general.
| Acknowledgments | | |
Appreciation goes to all the staff of the Department of Obstetrics and Gynecology especially the resident doctors that assisted directly or indirectly in the course of this study.
| References | | |
| 1. | Rukujei AD. Epidemiology of HIV/AIDS in Nigeria. Niger J Med 1998;7:8-10. 
|
| 2. | A Technical report on the 2001 National HIV/Syphilis Sentinel Survey among pregnant women attending Antenatal clinics in Nigeria; Federal Ministry of Health, National AIDS/STD Control Programme; Abuja, Nigeria, 2001.
|
| 3. | Federal Government of Nigeria. National Policy on HIV/AIDS. National Agency for the Control of AIDS, 2009. Available at http://nigeria.unfpa.org/pdf/ntpol.pdf. [Last accessed on 2012 Jul 15].
|
| 4. | Adewole IF, Odutolu O, Sagay AS. Prevention of mother-to-child transmission of HIV. In: Adeyi O, Kanki PJ, Odutolu O, Idoko JA, editors. AIDS in Nigeria, a Nation on the Threshold. Massachusetts: Harvard Center for Population and Development Studies; 2006. p. 349-84.
|
| 5. | WHO, UNAIDS, UNICEF. ′Global HIV/AIDS Response: Epidemic update and health sector progress towards Universal Access′, 2011. Available from: http://www.unaids.org/globalreport/Global_report.htm. [Last accessed on 2012 Jul 15].
|
| 6. | UNAIDS ′Report on the global AIDS epidemic′, 2008. Available from: http://www.unaids.org/en/KnowledgeCentre/HIVData/GlobalReport/2008/2008_Global_report.asp. [Last accessed on 2012 Jul 15].
|
| 7. | UNAIDS. ′UNAIDS report on the global AIDS epidemic′, 2010. Available from: http://www.unaids.org/globalreport/Global_report.htm. [Last accessed on 2012 Jul 20].
|
| 8. | Federal Ministry of Health. National Guidelines on Prevention of Mother to Child Transmission of HIV in Nigeria. Abuja: National AIDS/STI Control Programme (NASCP); 2005.
|
| 9. | Coutsoudis A, Kwaan L, Thomson M. Prevention of vertical transmission of HIV-1 in resource-limited settings. Expert Rev Anti Infect Ther 2010;8:1163-75.
|
| 10. | United Nations General Assembly, Special Session on HIV/AIDS. Declaration of commitment on HIV/AIDS. United Nations June 2001. Available at http://www.unaids.org/en/media/unaids/contentassets/dataimport/publications/irc-pub03/aidsdeclaration_en.pdf. [Last accessed on 2012 Jul 15].
|
| 11. | National Agency for the Control of AIDS. ′National HIV/AIDS response review 2005-09′, 2010. Available from: http://www.naca.gov.ng/index.php/index.php. [Last accessed on 2012 Jul 20].
|
| 12. | WHO, UNAIDS, UNICEF. ′Towards Universal Access: Scaling up priority HIV/AIDS interventions in the health sector′, 2010. Available from: http://www.who.int/hiv/pub/2010progressreport/en/index.html. [Last accessed on 2012 Jul 20].
|
| 13. | Federal Government of Nigeria. National Guidelines on Prevention of Mother to Child Transmission of HIV in Nigeria. Abuja: Federal Ministry of Health; 2011.
|
| 14. | Obiechina NJ, Diwe K, Ikpeze OC. Knowledge, awareness and perception of sexually transmitted diseases (STDs) among Nigerian adolescent girls. J Obstet Gynaecol 2002;22:302-5.
|
| 15. | Igwegbe AO, Ilika AL. Knowledge and perceptions of HIV/AIDS and mother to child transmission among antenatal mothers at Nnamdi Azikiwe University Teaching hospital, Nnewi. Niger J Clin Pract 2005;8:97-101.
[PUBMED]  |
| 16. | Yerdaw M, Nedi T, Enquoselassie F. Assessment of awareness of HIV/AIDS among selected target groups in and around Addis Ababa, Ethiopia. Afr J Reprod Health 2002;6:30-8.
|
| 17. | Federal Government of Nigeria. National HIV sero-Prevalence sentinel survey among pregnant women attending antenatal clinics in Nigeria: Technical Report. Federal Ministry of Health; 2010.
|
| 18. | Ayankogbe OO, Omotola BD, Inem VA, Ahmed OA, Manafa OU. Knowledge, attitudes, beliefs and behavioural practice for creating awareness about HIV/AIDS in Lagos state, Nigeria. Niger Med Pract 2003;44:7-10.
|
| 19. | Federal Ministry of Health, Nigeria. HIV and AIDS division. National Guidelines for Prevention of Mother to Child Transmission of HIV in Nigeria.Abuja, 4 th edition; 2010.
|
[Figure 1]
[Table 1], [Table 2]
|








 Search Pubmed for
Search Pubmed for