|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2013 | Volume
: 1
| Issue : 2 | Page : 54-57 |
|
Asymptomatic bacteriuria in HIV positive individuals in a tertiary care hospital
Asima Banu, Ramachandran Jyothi
Department of Microbiology, Bangalore Medical College and Research Institute, Bangalore, Karnataka, India
| Date of Acceptance | 24-Jun-2013 |
| Date of Web Publication | 6-Feb-2014 |
Correspondence Address:
Asima Banu
34/1 Sree Ram Mandir Road, Basavangudi, Bangalore 560 004, Karnataka
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-9157 .126630

Aims: To determine the prevalence, bacterial profile and antimicrobial susceptibility of asymptomatic bacteriuria in Human Immunodeficiency Virus (HIV) positive individuals. Materials and Methods: Urine from 300 HIV positive individuals were collected and cultured on cysteine lactose electrolyte deficient (CLED) agar and identified using standard techniques. Modified Kirby Bauer disc diffusion test was done according to Central Laboratory Standards Institute (CLSI) guidelines for antimicrobial sensitivity testing of the isolates. Results were compiled and statistically analyzed. Results: Of the 300 patients, 211 (70.3%) showed no growth, 77 (25.7%) had insignificant bacteriuria with a colony count of <10 5 CFU/ml and 12 (4.0%) had significant bacteriuria with colony count >10 5 CFU/ml without any signs or symptoms of urinary tract infections. The bacteriuria was significantly more in females (83.3%) than males (16.7%) with a P value of < 0.001. Eight (66.7%) cases of significant bacteriuria occurred in patients who were not on cotrimoxazole prophylaxis whereas 4 (33.3%) cases occurred in those who were on cotrimoxazole prophylaxis for at least one year. Conclusion: The incidence of asymptomatic bacteriuria was relatively less as compared to other studies and no correlation was found with CD4 counts, although evaluation with a larger study population needs to be undertaken. Keywords: Asymptomatic bacteriuria, HIV/AIDS, urinary tract infection
How to cite this article:
Banu A, Jyothi R. Asymptomatic bacteriuria in HIV positive individuals in a tertiary care hospital. J HIV Hum Reprod 2013;1:54-7 |
How to cite this URL:
Banu A, Jyothi R. Asymptomatic bacteriuria in HIV positive individuals in a tertiary care hospital. J HIV Hum Reprod [serial online] 2013 [cited 2017 Jan 13];1:54-7. Available from: http://www.j-hhr.org/text.asp?2013/1/2/54/126630 |
| Introduction | |  |
Asymptomatic bacteriuria or asymptomatic urinary infection is the isolation of a specified quantitative count of bacteria in an appropriately collected urine specimen obtained from a person without symptoms or signs referable to urinary infection. [1] Asymptomatic bacteriuria is a microbiological diagnosis wherein the usual quantitative definition is more than or equal to 10 5 CFU/ml in 2 consecutive urine specimens. In human immunodeficiency virus (HIV) infection, co-morbidity with other organisms is common. [2] Some studies have indicated that the risk of bacteriuria and urinary tract infections (UTI) may be increased in HIV-infected patients and is inversely related to CD4 lymphocyte counts. [3]
With the number of people living with HIV/AIDS (PLHA) in India, estimated a 23.9 million (19.3-30.4 million) in 2009, [4] there is no data regarding the occurrence of asymptomatic bacteriuria among this group in our country. Since NACO guidelines advocate the use of cotrimoxazole prophylaxis for all HIV positive cases, it is difficult for the physicians to treat urinary symptoms. This study was therefore carried out to determine the prevalence, bacterial profile, and antimicrobial susceptibility of asymptomatic bacteriuria in HIV positive individuals.
| Materials and Methods | | |
This study was carried out in the department of Microbiology of a tertiary care referral hospital attached to a medical college over a period of 3 months from October 2012 to December 2012. Institutional ethical clearance was obtained and informed consent was taken from each patient before being included in the study and permission was obtained to publish this data.
A total of 300 HIV positive patients aged between 1 to 70 years who were on antiretroviral therapy (ART) were included in the study as cases. Diabetics and pregnant women were excluded from the study. Controls were not included due to ethical considerations. Patients were duly counseled regarding the research purpose of this study and each was issued one sterile universal container for collection of mid-stream clean catch urine sample. Other details regarding the personal details, history of UTI, antibiotics taken and history of any opportunistic infection were taken from each case. Women whose urine sample yielded growth were asked to provide another early morning clean catch mid-stream urine sample for confirmation as per Infectious Diseases Society of America (IDSA) guidelines [1] whereas in case of men, a second sample was collected to confirm the findings of culture as there are no clear guidelines for HIV positive patients.
Semi-quantitative culture of each urine specimen was done on cysteine lactose electrolyte deficient (CLED) agar and incubated aerobically at 37C for 18-24 hours. The bacterial colonies obtained on the CLED agar were counted and identified using standard techniques. [5] Modified Kirby Bauer disc diffusion test was done according to Central Laboratory Standards Institute (CLSI) guidelines for antimicrobial sensitivity testing of the isolates using Ampicillin (10 μg), Cotrimoxazole (1.25/23.75 μg), Nitrofurantoin (300 μg), Norfloxacin (10 μg), Amikacin (30 μg), Ceftizoxime (30 μg), and Tetracycline (30 μg). [6]
| Results | | |
Semi-quantitative culture of urine was done for 300 HIV positive patients with a mean age of 36 years. Of these 173 (57.7%) were males, 125 (41.7%) were females, and 2 (0.7%) were transgender.
[Table 1] shows the results of semi-quantitative culture of the urine samples. 211 (70.3%) showed no growth, 77 (25.7%) had insignificant bacteriuria with a colony count of <10 5 CFU/ml and 12 (4.0%) had significant bacteriuria with colony count >10 5 CFU/ml without any signs or symptoms of UTI.
The organisms isolated in case of significant bacteriuria, as shown in [Table 2], were E. coli in 5 (41.7%) of cases, Staphylococcus aureus in 3 (25.0%), Pseudomonas aeruginosa in 2 (16.7%) cases and Klebsiella pneumonia and coagulase negative Staphylococcus in 1 (8.3%) each.
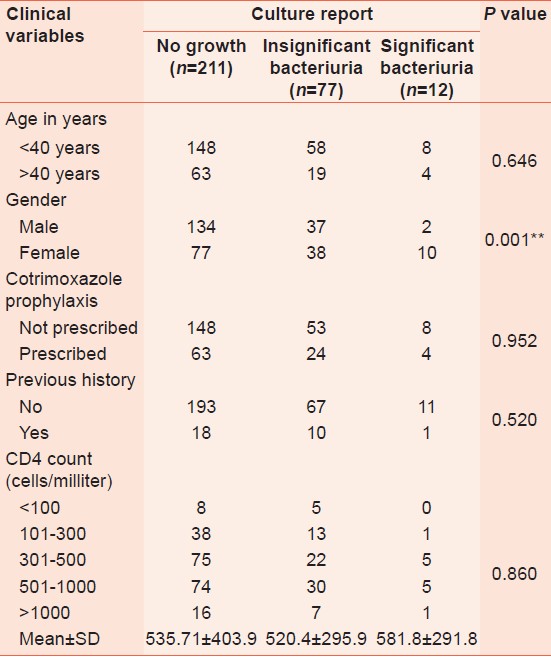
As shown in [Table 3], there was no correlation of bacteriuria with age. Eight (66.7%) cases of significant bacteriuria occurred in the age group <40 years where 4 (33.3%) were detected in >40 years. The bacteriuria was significantly more in females (83.3%) than males (16.7%) with a P value of < 0.001. Eight (66.7%) cases of significant bacteriuria occurred in patients who were not on cotrimoxazole prophylaxis whereas 4 (33.3%) cases occurred in those who were on Cotrimoxazole prophylaxis for at least 1 year. Of the 12 cases that yielded growth, 11 were resistant to cotrimoxazole and ampicillin (91.7%) whereas only one case was sensitive (8.3%). The organisms were sensitive to all the other antibiotics tested. Out of the 11 cases 12 occurred in cases that did not have a history of UTI whereas only 1 had a history of UTI in the past 6 months. When CD4 counts were correlated with the isolation of organisms there was no significant association found.
| Discussion | | |
This study attempts to evaluate the occurrence and prevalence of asymptomatic bacteriuria among HIV positive individuals. In our study, out of 300 HIV positive cases, 12 (4%) showed significant bacteriuria with a colony count of >10 5 CFU/ml. This is in contrast to a study by Inyang-Etoh et al., [7] who found a prevalence of 25.3%, the study by Schowald et al. [8] who found a prevalence of 25% in HIV positive individuals on antiretroviral therapy. However, this prevalence rate is consistent with the findings of Michael et al., [9] who found a rate of 6.3% among adolescents and young adults infected with HIV.
There was no correlation of bacteriuria with age. Although 8 cases of significant bacteriuria occurred in the age group <40 years while 4 were detected in >40 years. This could be due to the fact that generally the subjects in older age group were females who had declining sexual activity and so less risk development of bacteriuria. The bacteriuria was significantly more in females than males with a P value of < 0.001. This follows the trend in normal healthy individuals where females are at higher risk of being infected with UTI due to their short, straight urethra. However, this finding is in contrast with the study by Inyang-Etoh et al., [7] and Spence et al., [10] who reported a lower prevalence rate in females.
The most common organism isolated was E. coli in 5 (41.7%) of cases and Staphylococcus aureus in 3 (25%), which is similar to the study by Inyang-Etoh et al., [7] and Awolude et al., [2] However, the study by Michael et al., [9] isolated a high percentage of E. coli (50%) but a very low percentage of Staphylococcus aureus (10%) whereas a study by Widmer et al., [3] found E. coli to be most common (63%) followed by Proteus mirabilis (18%). Of the cases that yielded growth, 11 (91.67%) were resistant to cotrimoxazole which indicates that patients on cotrimoxazole prophylaxis could also be protected from UTI in addition to respiratory infections because of the continuous prophylaxis. However, those patients who were on prophylaxis and developed asymptomatic bacteriuria or UTI should not receive cotrimoxazole as they are most likely to be resistant.
Other studies have found significantly higher incidence of asymptomatic bacteriuria in this group compared to the normal healthy population in spite of cotrimoxazole prophylaxis. However, in our study, we found that cotrimoxazole was useful in the prevention of asymptomatic bacteriuria and possibly UTI. [7]
Evaluation of CD4 counts in our study showed that the significant bacteriuria occurred in cases with CD4 counts between 300-1000 (83.3%) with a mean of 581 as compared to patients with CD4 count less than 300 and above 1000, both of which had an infection rate of 8.33%. There was no significant correlation of CD4 counts with bacteriuria. This is in contrast to studies by Inyang-Etoh et al., [7] Widmer et al., [3] and Awolude et al., [2] all of whom found significant correlation between CD4 counts and occurrence of bacteriuria.
| Conclusion | | |
HIV/AIDS does not predispose an individual to increased incidence of UTI. However, when it occurs, it is caused by the same organisms that usually cause UTI in normal, healthy individuals. Physicians treating these patients should therefore consider asymptomatic bacteriuria as a possible source of infection and periodically monitor for the same.
| References | | |
| 1. | Nicolle E, Bradley S, Colgan R, Rice JC, Schaeffer A, Hooton TM. Infectious disease society of America guidelines for the diagnosis and treatment of asymptomatic bacteriuria in adults. Clin Infect Dis 2005;40:643-54. 
|
| 2. | Awolude OA, Adesina OA, Oladokun A, Mutiu WB, Adewole IF. Asymptomatic bacteriuria among HIV positive pregnant women. Virulence 2010;1:130-3.
[PUBMED] |
| 3. | Widmer TA, Theron G, Grove D. Prevalence and risks of asymptomatic bacteriuria among HIV positive pregnant women. South Afr J Epidemiol Infect 2010;25:28-32.
|
| 4. | WHO. HIV/AIDS. Statistics. Available from: http://www.who.int/gho/countries/ind.pdf. [Last accessed on 2012 Jan 03].
|
| 5. | Crichton PB. Enterobacteriaceae: Escherichia, Klebsiella, Proteus and other genera. In: Collee JG, Fraser AG, Marmion BP, Siminons A, editors. Mackie and McCartney Practical Medical Microbiology. 14 th ed. New York: Churchill Livingston; 1996. p. 361-4.
|
| 6. | Clinical and Laboratory Standards Institutes (CLSI). Analysis and presentation of cumulative antimicrobial susceptibility test data. 3 rd ed. Approved guideline M39-A3. Wayne, PA. CLSI 2009.
|
| 7. | Iyang-Etoh PC, Udofia GC, Alaribe AA, Udonwa NE. Asymptomatic bacteriuria in patients on antiretroviral drug therapy in Calabar. J Med Sci 2009;9:270-5.
|
| 8. | Schonwald S, Beqovac J, Skerk V. Urinary tract infections in HIV disease. Int J Antimicrob Agents 1999;11:309-11.
|
| 9. | Michael IO, Abel O, Ukoh G. Urinary tract infections in adolescent/young adult Nigerians with acquired immunodeficiency disease in Benin city. J Mol Biol Res 2006;5:55-60.
|
| 10. | Spence MR, Harwell TS, Jones K. Asymptomatic bacteriuria in women infected with HIV-1. Int Conf AIDS 1996;11:283.
|
[Table 1], [Table 2], [Table 3]
|









 Search Pubmed for
Search Pubmed for