|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2013 | Volume
: 1
| Issue : 2 | Page : 58-63 |
|
Adherence to antiretroviral therapy among people living with human immunodeficiency virus/acquired immunodeficiency syndrome in a tertiary health facility in South Eastern Nigeria
Ugochukwu U Onyeonoro1, Uzo E Ebenebe2, Christian C Ibeh2, Uche N Nwamoh1, Andrew U Ukegbu1, Obiageli F Emelumadu2
1 Department of Community Medicine, Federal Medical Center, Umuahia, Abia State, Nigeria
2 Department of Community Medicine, Nnamdi Azikiwe University, Newi Campus, Nigeria
| Date of Acceptance | 09-Nov-2013 |
| Date of Web Publication | 6-Feb-2014 |
Correspondence Address:
Ugochukwu U Onyeonoro
Department of Community Medicine, Federal Medical Centre, Umuahia, Abia State
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-9157 .126631

Introduction: This study was carried out among people living with human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) receiving antiretroviral therapy (ART) in a tertiary health facility in Nigeria and it is aimed at determining practice of adherence among these patients. Materials and Methods: A total of 282 HIV positive patients receiving ART in Nnamdi Azikiwe University Teaching Hospital, Nnewi were selected by systematic random sampling technique and using a semi-structured, interviewer administered questionnaire, responses were elicited from them on knowledge and perception of ART and adherence. Practice of adherence was determined by self-report. Findings were analyzed using Statistical Package for the Social Sciences version 17 (IBM Corp, Chicago Illinois, USA). Results: Most of the respondents were females (66.3%) and their mean age of the respondents was 36.63 8.56 years. Most of the respondents have good knowledge of ART and adherence, even though most of them (64.2%) thought that ART cures HIV/AIDS. Most patients still considered HIV/AIDS as a serious illness (78.0%). Only about half of them (50.7%) were of the opinion that ART reduces the risk of HIV transmission. However, the general perception of adherence was good. The mean level of adherence was 97.8%, however, about 86% of them attained optimal adherence level. Conclusion: The study revealed fairly good knowledge and perception of ART and adherence among the patients. The level of ART adherence was also high; however there is a need to address some gaps in knowledge identified as part of measures aimed at improving adherence in the long run. Keywords: Counseling, knowledge, Nigeria, perception, transmission
How to cite this article:
Onyeonoro UU, Ebenebe UE, Ibeh CC, Nwamoh UN, Ukegbu AU, Emelumadu OF. Adherence to antiretroviral therapy among people living with human immunodeficiency virus/acquired immunodeficiency syndrome in a tertiary health facility in South Eastern Nigeria. J HIV Hum Reprod 2013;1:58-63 |
How to cite this URL:
Onyeonoro UU, Ebenebe UE, Ibeh CC, Nwamoh UN, Ukegbu AU, Emelumadu OF. Adherence to antiretroviral therapy among people living with human immunodeficiency virus/acquired immunodeficiency syndrome in a tertiary health facility in South Eastern Nigeria. J HIV Hum Reprod [serial online] 2013 [cited 2017 Jan 21];1:58-63. Available from: http://www.j-hhr.org/text.asp?2013/1/2/58/126631 |
| Introduction | |  |
Since the discovery of the first case of acquired immunodeficiency syndrome (AIDS) in Nigeria in 1986, the human immunodeficiency virus/AIDS (HIV/AIDS) prevalence rate initially rose from 1.8% in 1988 to peak at 5.8% in 2005, but thereafter there has been a consistent decline in prevalence since then to 4.1% in 2010. [1] As at 2011, a total of 3.1 million people are living HIV/AIDS in the country, with about 1.5 million of them requiring anti-retroviral therapy (ART). [2] HIV/AIDS pandemic has far-reaching, health, social, political, cultural and economic implications which no doubt impacts negatively on the development of countries affected by it. These include increased mortality and morbidity, reduced life expectancy, increased poverty due to loss of family income for food, shelter, clothing and education, increased cost of health care, increased pressure on health resources, disruption of family and social structures, workforce depletion and reduced productivity. [3],[4],[5]
Few years ago someone living with HIV/AIDS had little hope of survival. HIV infection brought a steady inexorable decline towards the complete destruction of the immune system and death. However, the advent of antiretrovirals (ARVs) has brought about a significant change in the perception of HIV/AIDS. [6] Although, they cannot cure HIV/AIDS, ARVs have dramatically reduced mortality and morbidity, prolonged lives and improved quality of life of many people living with HIV/AIDS (PLHIV/AIDS). [6],[7],[8] In most countries world-wide including Nigeria, the numbers of new AIDS diagnosis and deaths have fallen substantially during the past few years. The trend is primarily due to increased use of potent anti-HIV drugs. [9] The goal of therapy is full suppression of viral replication below the detectable level by the most sensitive assay available, increase in CD4 cell count and improvement in quality of life. There have been also associated immunological restorations, a slowing of disease progression, durable therapeutic responses, improvement in quality of life and prevention of emergence of drug resistance. However, one major limitation of the current available therapies is incomplete normalization of the immune system and complete eradication of the virus are unlikely. The persistence of latent HIV is particularly problematic and suggests lifelong treatment may be necessary. [10]
Adherence to medication is a significant determinant of the outcome ART therapy and has been defined as the extent to which a person currently takes prescribed medication. [11],[12] Non-adherence or poor adherence to medication is often characterized by increased morbidity, premature death and economic loss. Furthermore, it results in rapid disease progression, development of complications, low quality of life and increase the cost of care both direct and indirect, increased risk of treatment failure, emergence of drug resistance, loss of therapeutic options which threatens already achieved success in HIV control. Adherence to highly active ART medication invariably results in improved individual (patient's) well-being, reduced cost of care, increased patient's safety, reduced risk of HIV transmission and strengthens the health system. [12] Adherence rate of less than 95% have been found to be associated with in poor treatment outcome and studies have reported satisfactory ART adherence among HIV positive patients in sub Saharan Africa. [13] Nigeria launched a nationwide ART program in 2002 as part of World Health Organization "3 Χ 5" initiative, with initial funding by the Federal Government. In 2005, the ART program was scaled up with funding from President's Emergency Plan for AIDS Relief Program. The resulted in rapid expansion of ART services through the establishment of additional ART centers and increased capacity of care providers to treat HIV/AIDS resulting in increased access to ART. Despite increasing access to ART services in Nigeria not many studies have been done to ascertain the level of adherence in most of the centers. Also, it has been reported that increased access to ART do not always result in satisfactory level of adherence. [13] This study therefore is aimed at determining perception and practice of adherence among patients on ART at Nnamdi Azikiwe University Teaching Hospital, Nnewi.
| Materials and Methods | | |
This was a cross-sectional descriptive study, carried out in Nnamdi Azikiwe University Teaching Hospital, Nnewi. The center provides comprehensive ART services and these services are provided by an integrated multidisciplinary team drawn from Medicine, Hematology, Community Medicine, Obstetrics and Gynecology, Counselors, Social Welfare, Nursing, Pharmacy and Laboratory services. The center was one of the first ART sites established by Federal Government of Nigeria in mid-2002. Being the first ART center in south east Nigeria, it receives clients from Anambra State and other adjoining states. In addition patients from other parts of the country and beyond who often visit the state for business activities also utilize the ART services. The study was carried out between March, 2006 and January, 2007, as at which about 3000 patients were assessing ART services.
Sample size was based on the expected proportion of adherence to ART among PLHIV based on a previous study, [14] with relative precision of 5% and confidence interval of 95%. The initial calculated sample size was 255, but after adjusting for 90% response rate the estimated sample became 285.
However, a total of 282 patients aged ≥18 years, who had received ART for at least 3 months and who were on the first line regimen (two nucleoside reverse transcriptase inhibitor and one non-nucleoside reverse transcriptase inhibitor) only were selected using systematic random sampling method. From the list of patients attending the ARV Clinic obtained from Medical Records Department and based on average daily clinic attendance of 100 patients/day a total of 20 eligible patients were recruited per clinic day using systematic random sampling method using a sampling fraction of 1:5. The first patient was randomly selected; thereafter every other fifth eligible patient was selected each until the sample size was completed.
Using a pre-tested, interviewer-administered, semi-structured questionnaire data was collected from patients with the aid of five trained research assistants and responses were elicited from them on socio-demographic characteristics, knowledge of ART, perception of HIV/AIDS and ART and barriers to adherence. Medication adherence was measured using the self-report method, whereas adherence rate was calculated using the formula:

Where number pills taken = number of pills prescribed - number of pills missed over 1 month-period.
Data collected were analyzed using Statistical Package for the Social Sciences version 17, relevant means and standard deviations were calculated and test of significance were carried out using Chi-square test and (P ≤ 0.05) was assumed to be statistically significant.
| Results | | |
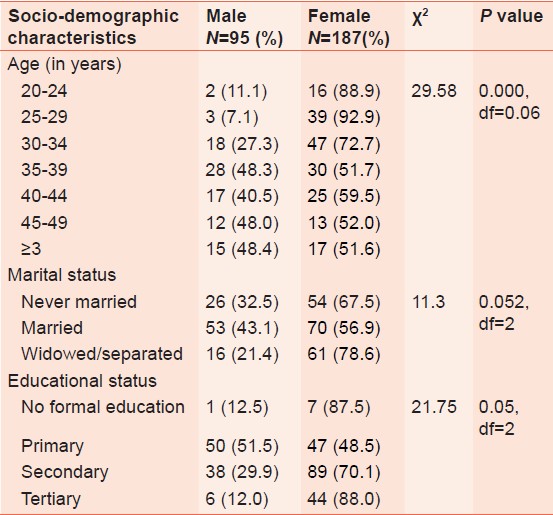
Of the 282 HIV-positive persons studied 187 (66.3%) were females, while the remainder (33.7%) was males. The mean age of the respondents was 36.6 8.6 years, with age group 30-39 years accounting for 44% of all the patients studied.
Majority (43.6%) of them were married, females 53 (43.1%) and males 70 (56.9%). 216 patients (76.6%) resided within the state, those from the neighboring states accounted for about 16% and the remainder was resident in other parts of the country and beyond [Table 1].
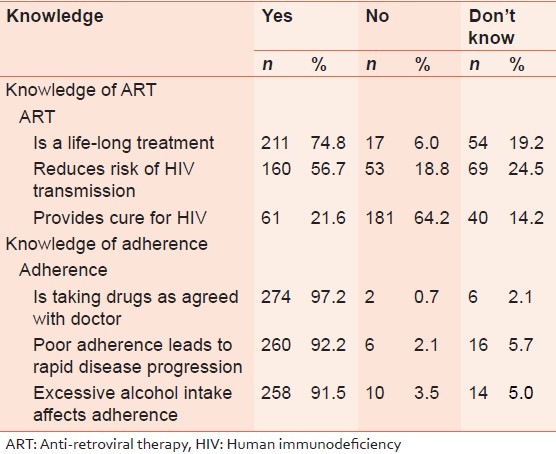
[Table 2] shows that 74.8% of them knew that ART is a life-long treatment and 160 (56.7%) knew that ART reduces the risk of HIV transmission. While about one-fifth (21.6%) of them thought that ART cures AIDS. On the other hand, their knowledge of adherence was quite high, as more than 90% knew that it is taking your drug as agreed with your doctor and poor adherence could lead to worsening of disease condition.
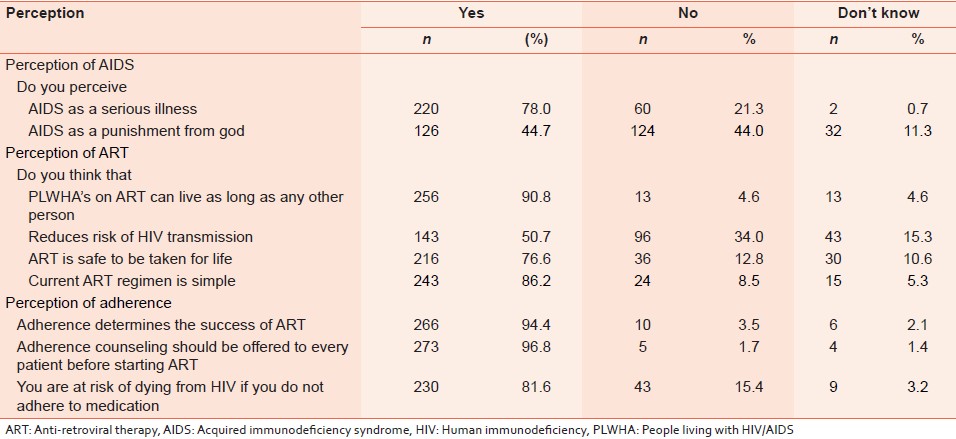
As shown in [Table 3] majority of people living with HIV/AIDS (78%) perceive HIV/AIDS as a serious illness and 44.7% of believe it is punishment from God. About 90% of them believe that individual on ART can live as long non-HIV-infected individuals. About half of them believe that ART reduces the risk of HIV transmission while 76% of felt that ART is safe to be taken for life. In general, their perception of adherence is good, as (94.4%) believe that it determines the success of ART, 97% thought that all patients commencing ART should be counseled and 81.6% thought that non-adherent individuals are at risk of dying.
[Table 4] shows pattern of ART medication adherence among the patients. 185 patients (65.6%) had 100% adherence rate in the last 1 month; however among those that have missed their medication 12.8% had 98.3% adherence rate, while 10.3% had an adherence rate of 86.6% adherence rate. Most of them (85.8%) attained optimal adherence rate of e95%. In general, the mean adherence rate among the patients was 97.9%. A total of 97 (34.4%) patients missed their medication at least once in the last 1 month. Reasons given for missing their medication included; traveled (26%), forgot (21.9%), ran out of medication (21.9%), not able to pay (9.4%), drug reactions and work demands 4.2% respectively. In addition 92 (32.6%) of them used local medication prior to commencement of ART, while 8 (2.9%) continued despite being on ART.
| Discussions | | |
Most of the patients were in reproductive age group which no doubt coincides with the group most commonly infected with HIV/AIDS. There was also disproportionate infection and affectation of women by HIV/AIDS as has been previously reported in earlier studies. They accounted for 65% of the patients studied, as well as the majority of those who have lost their marital relationship either by death or separation of spouses. [13],[14] A relatively greater proportion of females accessing ART may also, be a reflection of differential health seeking behavior of the two sexes, especially in a traditional African setting where women are known to have better care seeking behavior than men. [15] Although, most of the patients were resident in the state, about 25% came from outside the state to access ART. Stigma and discrimination is one of the reasons why some HIV positive patients prefer to access care in localities far from their place of residence, they will not want those close to them to be aware of their sero-status.
Our study revealed high knowledge of ART and adherence among PLHIV assessing care in this facility. Less than 60% of them knew that ART reduces the risk of HIV transmission. This is significant since it provides an opportunity for increasing uptake of prevention of mother-to-child transmission. However, misconception of ART is still common among them, as 21% of PLHIV thought that it is a cure for HIV/AIDS. A study in Soweto, South Africa also reported high knowledge of HIV/AIDS, ART and adherence among PLHIV. [17]
Most of the patients in our study still perceived HIV/AIDS as a serious illness, despite being on ARVs. About 44% of the respondents were of the opinion that the disease is a punishment from God for sin. Even though elsewhere increasing availability of ARVs is one of the factors changing perception of the seriousness of HIV/AIDS, as community members no longer regard the illness as a big threat. [6] In general, their perception of ART with respect to its benefits, safety and efficacy was good and most patients believed that benefits of ART can only be attained through adherence to medication. Knowledge of adherence is high (>90%) and perception of ART adherence was good. The study attempts to highlight that most patients on ART in this facility understood the benefits and implications of adherence and non-adherence to medication respectively. An earlier study in Benin City had reported good knowledge of adherence and its importance among patients using ARVs. [18]
About 35% of the patients had at one time or the other missed their medication in the preceding month for a number of reasons, this differs considerably from the study in Kano and Enugu, [14],[19] where 77% and 75% respectively were found not to be fully adherent to their medications. The mean adherence rate of all the patients was 97.9% and is significantly higher than 73.8% reported in Benin City, Nigeria. [18] Prevalence of optimum adherence among the study population was 85% and is higher compared to the findings of study in Botswana (54%). [20] Although, the level of ART adherence reported among patients in our study is quite commendable, yet there is a need for sustained improvement to ensure the optimization of benefits ART. This finding further buttresses the argument that the earlier fear of non-adherence in sub-Sahara Africans is unfounded. Some factors responsible for the high adherence level reported in our study include provision of free ART services, quality ART adherence counseling and general improvement in quality of HIV services.
For patients who missed their medications, reasons given include; traveled out of town (26%), forgot (21.1%), ran out of medication (21.1%) not able to pay for ancillary HIV services (9.4%), drug reaction (4.2%), work demands (4.2%) and others (12.5%). Some of the reasons mentioned are patient-related, while others are health system-related and are not different from reasons reported in previous studies done elsewhere. [21],[22],[23] Knowledge of factors that influence adherence is important in the development of interventions to improve adherence. [24] Patient-related factors could be addressed during follow-up counseling services. Health-system-related factors on the hand could be addressed by strengthening monitoring and evaluation and by adopting quality assurance and improvement measures. These are necessary for ensuring the sustenance of the high level of adherence observed among these patients on ART.
Our study had some limitations. Adherence to ART medication was assessed through self-reporting adherence questionnaire rather than using other more objective measures such as electronic pills count, medication events monitoring system, viral load estimation and CD4 cell count. These measures could not be used because our study was a cross sectional study. Secondly, the operational definition for the purpose of this study is limited in scope and did not take into consideration adherence as it relates to timing and relationship to food.
Also, the study did not explore further, factors influencing adherence and non-adherence to ART among the patients, neither did it assess the relationship between knowledge and perception of ART and adherence and adherence level.
| Conclusion | | |
It is should be noted that self-report assessment of medication adherence has often shown very high level of adherence compared to adherence measured by other means such as pill counts, pharmacy records and electronic monitoring. Considering the high burden of HIV/AIDS in the country/and sub Saharan Africa there is a need to sustain the high level of adherence already attained so as to maintain the success of HIV program attained over the years. To achieve this, measures should be taken to identify systematic ways of addressing factors responsible for non-adherence identified in this study and in other studies.
| References | | |
| 1. | FMOH. National HIV Sero-Prevalence Sentinel Survey. Abuja: FMOH; 2010. 
|
| 2. | NACA. Factsheet 2011: Update on the HIV/AIDS Epidemic and Response in Nigeria. Abuja: NACA; 2011.
|
| 3. | Adamson SM, Phiri A. Did maternal mortality ratio increase in Malawi between 1992-1998? Review of Malawi demographic and health surveys and other data sources. Trop Doct 2003;33:182-5.
[PUBMED] |
| 4. | USAID. How does HIV/AIDS Affect African Businesses? HIV/AIDS and Business in Africa. Washington D.C: Social and Systems, Inc./Synergy Project; 2001. p. 3-10.
|
| 5. | CHGA. The Impacts of HIV/AIDS on Families and Communities in Africa. Commission on HIV/AIDS and Governance in Africa. Addis Ababa, Ethiopia: Economic Commission for Africa; 2010. Index No. CHGA-B-I1-0001.
|
| 6. | Atuyambe L, Neema S, Otolok-Tanga E, Wamuyu-Maina G, Kasasa S, Wabwire-Mangen F. The effects of enhanced access to antiretroviral therapy: A qualitative study of community perceptions in Kampala city, Uganda. Afr Health Sci 2008;8:13-9.
|
| 7. | Cloete A, Strebel A, Simbayi L, van Wyk B, Henda N, Nqeketo A. Challenges faced by people living with HIV/AIDS in Cape Town, South Africa: Issues for Group Risk Reduction Interventions. AIDS Res Treat 2010;2010:420270.
[PUBMED] |
| 8. | van Empelen P. What is the Impact of HIV on Families? Copenhagen: WHO Regional Office for Europe (Health Evidence Network Report); 2005. Available from: http://www.euro.who.int/Document/E87762.pdf. [Last accessed on 2011 Dec 01].
|
| 9. | WHO. Scaling up anti-retroviral therapy in resource-limited setting. Guidelines for a Public Health Approach. Geneva: WHO; 2002.
|
| 10. | Simpson RJ Jr, Mendys P. The effects of adherence and persistence on clinical outcomes in patients treated with statins: A systematic review. J Clin Lipidol 2010;4:462-71.
[PUBMED] |
| 11. | Jacobs L. Are your patients taking what you prescribe? A major determinant:-clinician-patient communication. Permanenate Journal 2002;6:23:59-61
|
| 12. | Monjok E, Smesny A, Okokon IB, Mgbere O, Essien EJ. Adherence to antiretroviral therapy in Nigeria: An overview of research studies and implications for policy and practice. HIV AIDS (Auckl) 2010;2:69-76.
[PUBMED] |
| 13. | Charurat M, Oyegunle M, Benjamin R, Habib A, Eze E, Ele P, et al. Patient retention and adherence to antiretrovirals in a large antiretroviral therapy program in Nigeria: A longitudinal analysis for risk factors. PLoS One 2010;5:e10584.
[PUBMED] |
| 14. | Iliyasu Z, Kabir M, Abubakar IS, Babashani M, Zubair ZA. Compliance to antiretroviral therapy among AIDS patients in Aminu Kano Teaching Hospital, Kano, Nigeria. Niger J Med 2005;14:290-4.
[PUBMED] |
| 15. | UNAIDS/WHO. Ithembalabantu "Thembalabantu Clinic Kwazulu-Natal South Africa, First Year Progress Report. UNAIDS/WHO Epidemiological Fact Sheet, South Africa. 2002 Update.Durban, South Africa; 2003.
|
| 16. | Achappa B, Madi D, Bhaskaran U, Ramapuram JT, Rao S, Mahalingam S. Adherence to antiretroviral therapy among people living with HIV. N Am J Med Sci 2013;5:220-3.
[PUBMED] |
| 17. | Nachega JB, Lehman DA, Hlatshwayo D, Mothopeng R, Chaisson RE, Karstaedt AS. HIV/AIDS and antiretroviral treatment knowledge, attitudes, beliefs, and practices in HIV-infected adults in Soweto, South Africa. J Acquir Immune Defic Syndr 2005;38:196-201.
[PUBMED] |
| 18. | Agu KA, Ochei UM, Oparah AC, Onoh OU. Treatment outcomes in patients receiving combination antiretroviral therapy in Central Hospital, Benin City, Nigeria. Trop J Pharm Res 2010;9:1-10.
|
| 19. | Uzochukwu BS, Onwujekwe OE, Onoka AC, Okoli C, Uguru NP, Chukwuogo OI. Determinants of non-adherence to subsidized anti-retroviral treatment in southeast Nigeria. Health Policy Plan 2009;24:189-96.
[PUBMED] |
| 20. | Weiser S, Wolfe W, Bangsberg D, Thior I, Gilbert P, Makhema J, et al. Barriers to antiretroviral adherence for patients living with HIV infection and AIDS in Botswana. J Acquir Immune Defic Syndr 2003;34:281-8.
[PUBMED] |
| 21. | Ware NC, Idoko J, Kaaya S, Biraro IA, Wyatt MA, Agbaji O, et al. Explaining adherence success in sub-Saharan Africa: An ethnographic study. PLoS Med 2009;6:e11.
[PUBMED] |
| 22. | Kip E, Ehlers VJ, van der Wal DM. Patients' adherence to anti-retroviral therapy in Botswana. J Nurs Scholarsh 2009;41:149-57.
[PUBMED] |
| 23. | Curioso WH, Kepka D, Cabello R, Segura P, Kurth AE. Understanding the facilitators and barriers of antiretroviral adherence in Peru: A qualitative study. BMC Public Health 2010;10:13.
[PUBMED] |
| 24. | Abel E, Painter L. Factors that influence adherence to HIV medications: Perceptions of women and health care providers. J Assoc Nurses AIDS Care 2003;14:61-9.
[PUBMED] |
[Table 1], [Table 2], [Table 3], [Table 4]
|








 Search Pubmed for
Search Pubmed for