|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2014 | Volume
: 9
| Issue : 1 | Page : 27-30 |
|
Survey of hepatitis B and C Infection in an unselected population of members of a sports club in Aba, Abia State, Nigeria
U Onwuchekwa1, LN Chigbu2, UM Nwosu3, O Uchefuna1
1 Department of Internal Medicine, College of Medicine and Health Sciences, Abia State University Teaching Hospital, Uturu, Abia, Nigeria
2 Department of Pathology, College of Medicine and Health Sciences, Abia State University Teaching Hospital, Uturu, Abia, Nigeria
3 Department of Nursing Sciences, College of Medicine and Health Sciences, Abia State University Teaching Hospital, Uturu, Abia, Nigeria
| Date of Web Publication | 15-May-2014 |
Correspondence Address:
L N Chigbu
Department of Pathology, College of Medicine and Health Sciences, Abia State University Teaching Hospital, Uturu, Abia
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/9783-1230.132555

Background: Member of Aba Spots club including some of the family members were screened for the prevalence of Hepatitis B and C infection. Testing members of the Aba Spots club along with their family members is a strategy to identify undiagnosed hepatitis B and C virus infections in Aba, Nigeria. We also assessed how the social life of members of Aba Spots Club may influence the acquisition of Hepatitis B and C infections. Materials and Methods: Demorgraphic information of members was collected as blood samples were analyzed for each member using commercially procured test strips. Proportions of those tested for Hepatitis B and C infections were determined. Results: Among the 470 members, 211; comprising 139 club members and 72 family members, were accessible for Hepatitis B and C infection survey. Prevalence of Hepatitis B and C infection was 3(1.4%) and that of Hepatitis C was 2 (0.95%), with an overall prevalence of 5 (2.4%). No past results of infection and immunization were noted among the subjects. Conclusion: This study offers opportunity to capture, identify and educate infected and unaffected members of the society on the health hazards associated with Hepatitis B and C infections. Those with known positive hepatitis status also received treatment and those considered susceptible were educated on how to initiate preventive action (e.g. vaccination). Keywords: Hepatitis B and C, Survey
How to cite this article:
Onwuchekwa U, Chigbu L N, Nwosu U M, Uchefuna O. Survey of hepatitis B and C Infection in an unselected population of members of a sports club in Aba, Abia State, Nigeria. J Med Investig Pract 2014;9:27-30 |
How to cite this URL:
Onwuchekwa U, Chigbu L N, Nwosu U M, Uchefuna O. Survey of hepatitis B and C Infection in an unselected population of members of a sports club in Aba, Abia State, Nigeria. J Med Investig Pract [serial online] 2014 [cited 2018 Aug 24];9:27-30. Available from: http://www.jomip.org/text.asp?2014/9/1/27/132555 |
| Introduction | |  |
Hepatitis B Virus (HBV) and Hepatitis C Virus (HCV) have been found to be the most important causes of chronic liver disease such as liver cirrhosis, and liver cancer ultimately resulting in premature death. [1]
Hepatitis B Virus infection is a major disease of mankind. It is more prevalent in the developing countries, as available human and material resources were effectively applied to control the spread of HBV in the developed world. [2] Worldwide serological evidence of past or present infection with HBV found the infection in about 2 billion people. Of this number, 350-400 million are chronically infected and this results in about 1 million deaths annually. [3],[4]
In Nigeria, most infections occur in childhood (vertical and horizontal transmission). About 70-90% of vertical infections will result in a chronic infection compared with 20-50% of early childhood infections (horizontal) which will progress to the chronic stage. [5] In contrast, when transmission occurs in adolescents or adults, only 1-3% will progress to the chronic infection unless if the individual is immuno compromised. [5]
Nigeria is an area of high endemicity for HBV, with over 70% of the population showing evidence of past infection with the virus. About 7.3-24% of the population has serological evidence of current infection (average 13.7%). Going by the 2006 national census, this translates to 19 million Nigerians being currently infected and about 5 million of these will die of the consequences of this infection. [5]
The WHO [6] puts the average worldwide prevalence of HCV infection at 3.1%, with Africa recording the highest prevalence rate of 5.3%. Other regions of the world have lower rates - Americas 1.7%, Eastern Mediterranean 4.6%, Europe 1.03%, South East Asia 2.15% and Western Pacific 3.9%. In Africa, the following prevalence rates have been reported in the various countries - Gabon, 22%, Malawi, 16.5%, Madagascar, 3.3%, Ghana 5.4%, Burkina Faso 4.9% and Guinea 1.1%.
However, a pilot study done in Nigerian adults and children gave an average seroprevalence of 8%. [8] While a study of adult blood donors in Nigeria reported a prevalence rate of 12.3%. Another study in Ibadan, Nigeria conducted amongst doctors and dentists reported prevalence of 11%. [10]
Acute hepatitis C is symptomatic in a minority of cases and usually runs a mild clinical course, with only - third or fewer of patients being jaundiced and many are completely asymptomatic. [11] The disease is rarely culminant but this has been reported to occur. [12] Chronic HCV infection is defined as the presence of HCV for longer than 6 months. [13] Most patients with HCV infection appear to have mild to moderate histological disease. [14]
The liver disease caused by both Hepatitis B and C is silent and unrecognized. The impact is often underestimated by both the sufferers and the healthcare professionals. Consequently most patients present very late with advanced liver cirrhosis and cancer. [5]
Cirrhosis of the liver may develop in as many as 15-20% of infected patients. Factors that accelerate disease progression include ingestion of alcohol, coexisting human immunodeficiency virus or HBV infection, male gender and older age. [15]
There is high alcohol consumption amongst most members of Aba sports Club, the screening for hepatitis B and C Virus infection was conducted as preventive measure against liver cirrhosis and cancer of the liver; because of the additive effect of ingestion of alcohol and coexistent HBV/HVC infection. This study is therefore aimed at accessing the prevalence of Hepatitis B and C Viruses among members of a Sports Club in Aba and those of their family members.
| Materials and Methods | | |
Accessible members of a Sports Club in Aba, Nigeria and their family members, in all 211, were surveyed for the prevalence of Hepatitis B and C virus infections. After due counseling and informed consent was obtained, participants completed a structured questionnaire, containing such information as; sex, age, marital status, past medical and immunization histories.
Hepatitis-B surface antigen and hepatitis-C Antigen were detected in participants' serum specimen using Diaspot one step hepatitis B and C test strip, manufactured in USA, RO15624-04. Two (2.0ml) milliliters of venous blood was collected using sterile syringes and needles from the participants and transferred into a clean anticoagulant free 5ml test-tube and allowed to clot, centrifuged and the serum separated.
Using the pipette provided in the kit, about .75mL (3 drops) of serum specimen was put on the specimen pads of the 2 test strips, one for HBS-Ag and the other for HCV-Ag, already at room temperature, and allowed for 15 minutes for the serum specimen to react with the anti-HBs-Ag and HCV-Ag antibodies conjugated particles. The mixture further migrated upward on this membrane chromatographically by capillary action to react with the anti-HBS-Ag and HCV-Ag antibodies on the membrane and generate a colored line. The presence of this colored line in the test region indicated a positive result. While its absence is indicated a negative result. A colored line which developed in the control line region served as a procedural control.
| Results | | |
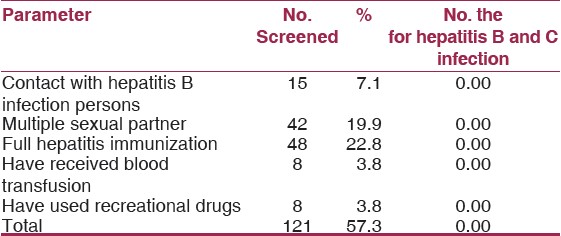
Among the 470 members of Aba Spots Club, 211 subjects comprising 139 club members and 72 family members were accessible for the Hepatitis B and C virus infection survey. Out of the 211 studied population 15 (7.1%) reported having contact with hepatitis infected persons, 42 (19.9%) indicated having had multiple sexual partner, while 48 (22.8%) reported having received full hepatitis immunization. As well, 8 (3.8%) indicated having received blood transfusion as well as recreational drug in their lifetime [Table 1]. No subjects with the above mentioned demographic characteristics gave positive result for either hepatitis B or C virus infection [Table 1].
The age of recruited subjects ranged from 2 years and 64 years, with a mean age of 34.4 years. Among 211 tested, 5 (2.4%) of both infections; hepatitis-B infection (1.43%) and Hepatitis C infection; 2 (0.95%) were detected. Age groups 14-19 and 44-49 years old, 32-37 year old, yielded these infection cases; 2 (6.9%), 2 (40.0% and 1 (4.5%) respectively, with 14-19 year old and 32-37 years yielding one person each that had the dual infections of hepatitis B and C virus. The 44-49 year old had only a case of hepatitis B - virus infection to make up 5 (20.4%) cases of hepatitis infection detected in the survey [Table 2].
Considering the prevalence of hepatitis B and C infection in relation to the sexes, two (2.4%) Hepatitis B and only one (1.2%) hepatitis C infection cases were from female subjects, and only one of the hepatitis B and C infection cases came from male subjects [Table 3]. A case of the dual infections was detected from a 15 year old school girl, household member of club member, while the other dual infection came from a male member of the club.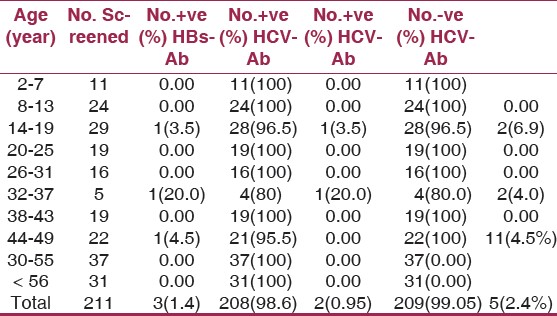 | Table 2: Relation between the age distribution and HBs – Ag and HCV-Ag antibody positive
Click here to view |
| Discussion | | |
Hepatitis B and C viruses (HBV and HCV) cause significant morbidity and mortality worldwide. With the rise in alcohol consumption among members of social clubs, many people in the society stand the risk of Hepatitis B and C virus infection.
The prevalence of both hepatitis B and C virus infection in this study is 2.4%; this is low compared with the prevalence rate of 12.3% reported among blood donors in Ibadan, Nigeria. [10] Previous data on the prevalence of Hepatitis B and C virus infection indicated an increase in the incidence of infection among people with increased alcohol consumption, contact with infected family member, multiple sexual partners and having received blood transfusion. [15] Use of recreational drugs is another important risk factor for Hepatitis B and C Virus infections. In this survey, records showed that of the 7.1% and 19.9% subjects reported having contact with the hepatitis infected persons and those who indicated having had multiple sexual partners respectively, none was positive for either Hepatitis B or C virus infection. Also, of the 22.8% reported having received full hepatitis immunization and the 3.8% of those indicated having received blood transfusion in their lifetime; none have positive results for both hepatitis B and C virus infection and either of them. Although the results of the study could not demonstrate causal relationship between these noted subject characteristics among members of Aba Sports Club and some of their family members, these characteristics serving as potent risk factors for both infections should not be ruled out.
The report of the survey did not also link both hepatitis B and C - virus infection to the subjects' differences in age group possibly due to the study population. There is no differences in the prevalence of the infection between the sexes. The 15 year old school girl, who is a family member of a member of the club, who had the dual infections, the infection may not be associated with contact with any of the members of the social club, rather, it may be reasoned that she got the infection possibly from her infected school peers. Based on this report, health practitioners are assisted to provide more appropriate advice on the prevention of the infections in our communities. As well, such individual members of the social club who have been detected positive for the infections received immediate treatment. While those that were screened and the rest of the unscreened members would benefit from HBV and HCV vaccination and also receive advice regarding the mode of transmission and the activities that place them at risk of both infections.
| References | | |
| 1. | Beasley RP. Hepatitis B Virus. The major etiology of hepatocellular carcinoma. Cancer 1988;61:1942-56. 
[PUBMED] |
| 2. | Johnson AO, Sodeinde O, Odeola HA, Ayoola EA. Survey of Hepatitis A and B infection in childhood in Ibadan-Preliminary Study. Niger J Paediatr 1986;13:83-6.
|
| 3. | WHO, Hepatitis B. Available from: http://www.who.inf/inf-fs/en/fact2004.html.
|
| 4. | Geographical Distribution HBV infection. Available from: http://www.cdc.gov//ncidod/disease/hepatitis/slideset/hepb/slide9.html [Last accessed in 2003 May].
|
| 5. | Society for Gastroenterology and Hepatology in Nigeria. Treatment Guidlines for Nigeria. Available from: http://www.soghin.org.
|
| 6. | World Health Organization Hepatitis C WHO fact sheet Bo.164. Available from: http://www.who.int/inffs/en/fact 164.htm [Last accused in 2006 Apr].
|
| 7. | Memon MI, Memon NA. Hepatitis C: An Epidemiological Review. J Viral Hepat 2002;9:84-100.
|
| 8. | Oni AO, Harrison TJ. Genotypes of Hepatitis C virus in Nigeria. J Med Viral 1996;49:178-86.
|
| 9. | Halim NK, Ajayi OI. Risk factors and sero-prevalence of Hepatitis C in Blood donors in Nigeria. East Afr Med J 2000;77:40-2.
|
| 10. | Olubuyide IO, Ola SO, Aliyu B, Dosumu OO, Arotiba JT, Olaleye OA, et al. Hepatitis B and C doctors and dentists in Nigeria. QJM 1997;90:417-22.
|
| 11. | Achara G, Sadovisky R. Hepatitis C. Virus: An overview of Epidemiological factors and National History. Int Med World Rep 2000;15:1-27.
|
| 12. | Farci P, Alter HJ, Shimoda A, Govindarajan S, Cheung LC, Melpolder JC, et al. Hepatitis C virus associated fulmincut Hepatitic failure. N Engl J Med 1996;335:613-34.
|
| 13. | Takahashi M., Yamada G, Miyamoto R, Doi T, Endo H, Tsuji T. Natural History of Chronic Hepatitis C. Am J Gastroenterol 1993;88:240-3.
|
| 14. | Yano M, Kumada H, Kage M, Ikeda K, Shimamatsu K, Inoue O, et al. The Long term Pathological evolution of chronic hepatitis C. Hepatology 1996;23:1334-40.
|
| 15. | Coursaget P, Bourdi C, Kastelly R, Yvonnet B, Rampanarivo Z, Chiron JP, et al. Prevalence of Hepatitis C virus infection in Africa: Anti HCV Antibodies in the general population and in patients suffering from Girhosis or primary liver cell carcuccine. Res Virol 1990;141:449-54.
|
[Table 1], [Table 2], [Table 3]
|









 Search Pubmed for
Search Pubmed for