|
 
 |
| CASE REPORT |
|
| Year : 2014 | Volume
: 9
| Issue : 1 | Page : 47-50 |
|
Breast abscess complicting prolactinoma
F Uduma1, M Motah2
1 Department of Radiology, Faculty of Clinical Sciences, College of Health Sciences, University of Uyo, Nigeria; Polyclinic Bonanjo, Douala, Cameroon
2 Neuro-Surgical Unit, University of Douala; Polyclinic Bonanjo, Douala, Cameroon
| Date of Web Publication | 15-May-2014 |
Correspondence Address:
F Uduma
Department of Radiology, Faculty of Clinical Sciences, College of Health Sciences, University of Uyo, Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/9783-1230.132560

Prolactinoma is an intra-sellar benign adenoma. It could be micro- or macro-adenoma. The commoner micro-adenoma is an endocrine active. The distant effect of Prolactinaemia is on reproductive system and breast as seen in our Para-2 45 year old woman with pituitary micro adenoma, dense breasts and right breast abscess. Keywords: Abscess, Breast, Pituitary gland, Prolactinoma
How to cite this article:
Uduma F, Motah M. Breast abscess complicting prolactinoma. J Med Investig Pract 2014;9:47-50 |
| Introduction | |  |
Hyper prolactinaemia is elevated level of serum prolactin. Its aetiologies include neoplasm of adenohypophysis. Adenohypophysis or anterior lobe of pituitary gland is a complex gland composed of several cell types that are responsible for the production of many hormones. Neoplasm of this adenohypophysis are common tumors that exhibit a wide range of biological behavior in terms of hormonal and proliferative activities, [1] One of these tumors of the pituitary gland which is important in our context is prolactin-producing adenoma or lactotroph adenomas or prolactinoma. [2] Pituitary adenomas are classified as micro-adenomas or macro-adenomas. Micro-adenoma is defined as adenohypophyseal tumors smaller than 10mm in size and they usually present because of endocrine dysfunctions. While macro-adenomas are larger than 10mm in size and usually present due to symptoms of an intra-cranial mass or hormonal excess syndrome. [3] Prolactinomas are the commonest type of micro adenomas. [1],[3] Pituitary micro adenomas detected using computed tomography (CT) and magnetic resonance imaging (MRI) is between 3.7-37% cases while autopsy prevalence is 1.4-27%. [3] Some previous studies show high frequency of prolactinoma as high as 53% of pituitary micro-adenoma. [4]
Clinical presentations of prolactinomas include oligomenhorhea, amenorrhea and galactorrhea. Diagnostic work-up of prolactinoma includes MRI with 80-85% of pituitary microadenoma (PA) visible on just unenhanced T1W images. Treatment of prolactinoma is geared towards resolving prolactinaemic symptoms and reducing tumor size. This has been achieved by medical management using drugs like dopaminergic agonist. [5]
| Aim | | |
To present a case of prolactinoma in a woman with irregular menses, galactorhea and right breast abscess
| Case Report | | |
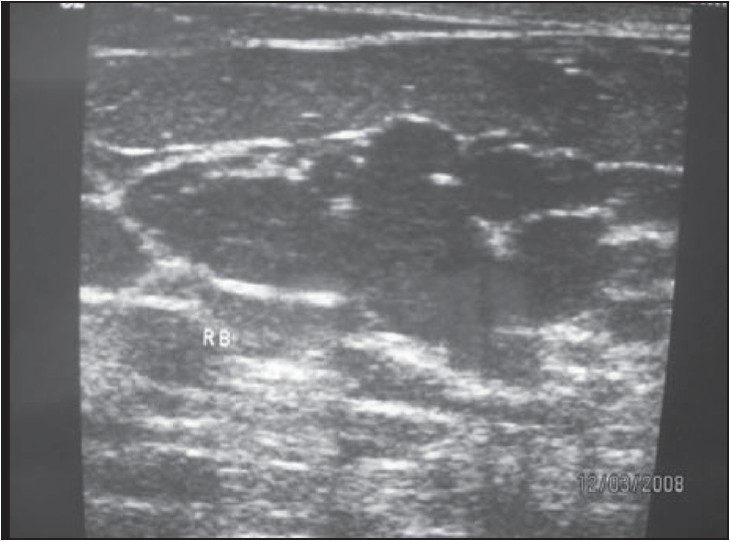
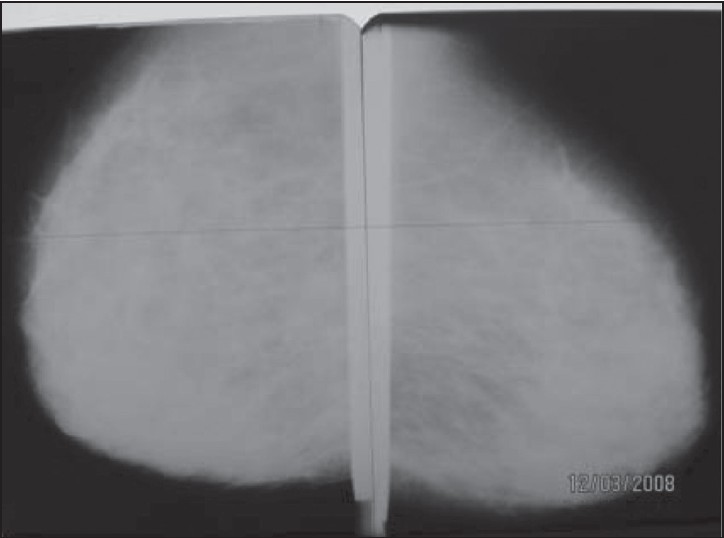
Mrs. M G is a 45 year old Para 2 Cameroonian woman with mastalgia, 2 months amenorrhea and milk expression from the breasts on self squeezing. No associated fever nor headache. She was diagnosed as having hyperprolactinaemia 4 years ago. She was placed on bromocriptine which she has been unreligious with. Bilateral mammography done showed bilateral dense breastss in a 45 year old woman,with peri-areolar lactiferous ductal ectasia and breast adenosis as shown in [Figure 3] (BIRADS Lexicon II).Further diagnostic workup with bilateral sonomammoography confirmed BIRADS Lexicon II [Figure 1] and [Figure 2]. The breast show homogenous fibro-glandular pattern with increased anterio-posterior diameter of each fibro-glandular tissue measuring 28mm. Both breasts harbour multiple echo free dilated lactiferous ductules measuring in size 5.2 to 7.8mm in diameter. The right breast also harbor 16 Χ14mm and 11 Χ 10mm echo- rich enhancing cystic masses at 12 o clock and 10 o clock respectively. No associated lymphadenopathy seen. Diagnosis of right breast abscess, lactiferous ductal ectasia and adenosis were made. Though brain CT was un-rewarding, brain MRI was fruitful. However,the detection of intrasellar tumour was only seen in the FLAIR sequence which demonstrated a central hyper intense focus encased by normal pituitary tissue [Figure 4].
The breast abscess was drained. She was sent home on antibiotics and bromocriptine and encouraged to be more judicious with her Bromocriptine therapy and follow-up. | Figure 4: FLAIR brain MRI showing hyper intense intrasellar pituitary mass
Click here to view |
| Discussion | | |
Prolactinoma is a subset of pituitary adenoma. The classification of pituitary adenoma is based on 4 criteria, namely, a) functional, b) radio-anatomical, c) histological, and d) ultra structural. [1],[2],[6]
The functional classification is based on in -vivo hormonal activity, and classified by endocrinologist as hormonal active or inactive. Hormonal active adenomas are prolactinomas, growth hormones adenomas, adreno-corticotrophic hormone (ACTH) producing adenoma associated with Cushing's syndrome or Nelson's syndrome, thyroid stimulating hormone (TSH) producing tumors, and the rare gonadotrophin producing follicle stimulating hormone and /or luteinizing hormone. [1]
This is supported by the ultra structural classification based on electron microscopy. Here there is cytological differentiation of the tumor cells with structure-function correlations into somatotrophs, mammosomatotrophs, lactotrophs, thyrotrophs, corticotrophs and Gonadotrophs. [1]
The histological classification based on Hematoxylin and eosin dyes is into acidophils ( prolactinoma, growth hormones), basophil (ACTH tumor) and chromophobe ( non-active) is now obsolete with chromophobe now known to produce prolactin and growth hormones. [1]
Another useful classification is the radio-anatomic classification into grade 0 to IV. This is a neuro-imaging classification validated by CT and MRI. Grade 0 is normal pituitary appearance. Grade I is micro-adenoma less than 1cm without sellar expansion. It could have 0-10mm supra sellar extension. Grade 2 is macro-adenoma greater than 1cm and may extend above the sella or 10-20mm supra- sellar or elevate the third ventricle. Grade III macro-adenoma with sellar enlargement, invasion of the sellar floor, with 20-30mm supra-sellar extension, occupying the anterior third of the third ventricle. Grade IV are large, invasive tumors with extra sellar extension into cavernous sinus, hypothalamus, bone, cerebrum and larger than 30 mm extension beyond the foramen of Monro. [1],[2],[7]
Pituitary tumurigenesis seems to be multi-factorial with molecular genetic alterations providing the initiating event that transforms cells with hormones and or growth factors playing a role in encouraging cell proliferations. Loss of hypothalamic inhibitions is due to systematic neo-arteriogenesis with negligible levels of dopamine allows the pituitary gland to escape the dopaminergic tonic inhibition of the hypothalamus. A second theory is excessive stimulation by a putative prolactin-releasing factor such as Thyroid releasing Hormone (TRH) or Vasoactive intestinal peptide (VIP). Other prolactin stimulating factors include oestrogen, oral contraceptives, and pregnancy. Oral contraceptives has been thought to be responsible for a possible increase in the incidence of lactotrophic adenomas in the late 70s. [1] But when compared to a lot of solid tumours and metastasis, pituitary tumors have reduced micro -vessel density which is an index of angiogenesis. Micro-prolactinoma has even lower micro vessel density than macro-prolactinomas. [4]
The aetiology of prolactinomas could be pituitary micro-adenoma, pituitary macro-adenoma, pituitary hyperplasia, pituitary carcinoma, multiple endocrine neoplasia I-III, Para-neoplastic syndrome, exogenous (drugs), ectopic sites, Oncocytoma. Pituitary carcinoma accounts for only 1-.2% of pituitary tumours. In a review of 95 cases of pituitary carcinomas, 68% were hormone producing, of which the commonest is prolactin producing (26%) and this prolactin producing carcinoma shows the highest systemic metastasis than cranio-spinal metastasis (71%), [2] This pituitary carcinoma are diagnosed with presence of metastasis to remote areas of the central nervous system (CNS) outside the CNS . But this should be differentiated from aggressive benign pituitary adenomas. They are unusually pluri-hormononal adenomas as well as rare lactotrophs adenoma with growth hormone immunoreactivity known as acidophil stem cell adenoma. [1] Oncocytoma of pituitary gland is characterized by an abundance of cytoplasmic mitochondria, hypopituitarism, and/or mild hyperprolactinaemia. [8] Though Pituitary prolactin macroadenoma is non secreting, the large size of the tumor compresses the pituitary stalk and occludes the hypothalamic regulatory control.
Histological assessment has shown prevalence of pituitary adenomas of 22.5-27%. Ezzat et al[1] reported frequency of pituitary adenomas of 14.4% (range1-35%) and 22.5% (range1-40%) in pooled autopsy and radiological series respectively. And of specimens that underwent immune-histochemistry, 25-41% of cells were prolactin positive. [6] Kim et al gave average age of pituitary adenoma of 50 years [5] with female predominance. While other reports showed equal sex incidence with incidence increasing with age. [1] No familial associations except in cases of Multiple endocrine neoplasia. Most pituitary micro-adenomas are clinically asymptomatic. As much as 20% of the normal pituitary glands harbour an incidental mass measuring 3mm or more in diameter. [5] But incidence increased with increasing age such that autopsy analysis of people between 50-60 years showed greater than 30% incidence. [1] The symptomatology of prolactinoma are characteristic. There are oligomenorrhea, amenorrhea, reduced fertility, loss of libido, erectile dysfunction, galactorrhea especially in the oestrogen primed female breast, visual field defects and headaches. If it is macro-adenomatous prolactinoma, invasion and compression of nearby neural and vascular structures leads to headache, hypopituitarism and visual loss. Stretching of the diaphragmatic sellae and adjacent structures transmit sensation through the first branch of trigeminal nerve leading to visual field defects and loss of central visual acuity.
Neuro-radiological imaging of prolactinoma are skull radiography, Pneumo-enencephalography, Carotid angiography, Computed tomography (CT), magnetic resonance imaging (MRI). [2] MRI is now considered the modern imaging modality of choice due to its multi-planar nature and good tissue contrast. Slice tissue thickness of 3mm achieves optimal resolution. Sagital MRI clearly depicts anterior and posterior pituitary lobes and stalk while coronal MRI shows relations like cavernous sinus and ventricles. Coronal MRI is the optimal acquisition for identification of pituitary tumor. [2] 80-85% of pituitary tumurs are seen on un-enhanced T1W images, while 33-50% are seen as area of hyper intensity on T2W or FLAIR sequences as in our index Patient. Contrast enhancement is only necessary in a minority of cases. [3] Dynamic MRI with time related administration of Gadolinium DTPA contrast medium and timed image acquisition is used accurately better than normal contrast enhanced MRI to delineate adenomatous nodule from normal adenohypophysis. It is also important to the Surgeons to differentiate macro-adenoma from normal tissue and decide on surgical approach. This dynamic MRI is based on enhancement of infundibulum, posterior pituitary, anterior pituitary and adenoma in that order. The peak contrast enhancement of pituitary adenoma occurring 60-200 seconds usually after the most marked contrast enhancement of the normal pituitary gland. [9] Radiological features shown by pituitary adenoma on dynamic MRI are morphological changes like infundibular displacement, focal gland convexity, sellar floor abnormality and cavernous sinus changes. [9] In our index patient, the persistent galactorrhea and milk stagnation in her breast became a good culture medium for a breast abscess. The high level of fasting serum prolactin she had accounted for her dense breast and adenosis at an age of 45 years.
The first line of standard treatment of prolactinoma is medical using Carbegoline or Bromocriptine, since Pergonal has been banned by United States Food and Drug administration ( USA FDA). [2] This is corrective for micro-adenoma but a pre-surgical treatment for macro-prolactinoma to shrink the mass and ameliorate chiasmatic compression and headache before surgery. [2] Sometimes, quite dramatically , micro-prolactinoma has decreased in size or under complete resolution. [2] Both Bromocriptine and Carbegoline are ergot derived dopamine agonist. But when prolactinomas is resistant to bromocriptine or patient can not tolerate bromocriptine, carbegoline is used and it has achieved >90% success rate ; but it is expensive. [10] But when fertility and safety records for pregnancy are the goals, bromocriptine remains the treatment of choice. [11] The second treatment is surgery using trans-sphenoidal approach. The third approach is radiotherapy.
| Conclusion | | |
Prolactinoma is an adenohypophyseal neoplasm with endocrinopathic effects on the reproductive system and breasts
| References | | |
| 1. | Asa SL, Ezzat S. The cytogenesis and pathogenesis of pituitary adenoma. Endocr Rev 1998;19:798-827. 
|
| 2. | Levy A. Pituitary disease, presentation, diagnosis and management. J Neurol Neurosurg Psychiatry 2004;75:iii41-7.
|
| 3. | Acosta-Gomez MJ, Muros MA, Llamas-Elvira JM, Ramirez A, Ortega S, Sabatel G, et al. The role of Somastatin receptor sctingraphy in patients with Pituitary Adenomas or Post-sugical Recurrent tumours. Br J Radiol 2005;78:110-5.
|
| 4. | Kim JH, Seo JS, Lee BW, Lee SY, Jeon SH, Lee KB. The characteristics of incidental pituitary microadenomas 120 Korea forensic autopsy cases. J Med Sci 2007;22 Suppl:S61-5.
|
| 5. | Shenenberger D. Hyperprolactinoma: Treatment and medication E-medicine. [Last updated on 2009 Aug 12].
|
| 6. | Daly AF, Rixhom M, Adam C, Dempegioti A, Tichomirowa MA, Beckers A. Prevalence of Pituitary Adenoma: A Cross sectional studies in the Province of Liege, Belgium. J Clin Endocrinol Metab 2006;91:4769-75.
|
| 7. | Ezzat S, Asa SL, Couldwell W, T, Barr CE, Dodge WE, Vance ML, et al. The prevalence of pituitary adenomas: A systemic review. Cancer 2004;101:613-9.
|
| 8. | Indrajit IK, Chidambaranathan N, Sunder K, Ahmed I. Value of dynamic MRI Imaging in pituitary adenoma. Neuroradiology 2001;11:185-90.
|
| 9. | Colao A, Di Sarno A, Landi ML, Scavuzzo F, Cappabianca P, Pivonello R, et al. Macro-prolactinoma shrinkage during cabergoline treatment is greater in native patients than in patients pre-treated with other dopamine agonists: A prospective study in 110 patients. J Clin Endocrinol Metab 2000;85:2247-52.
|
| 10. | Schlechte JA. Clinical pratice, prolactinoma. N Engl J Med 2003;340:2035-41.
|
| 11. | Kharlip J, Salvantori R, Yenokyan G, Wand GS. Recurrence of hyperprolactinoma after withdrawal of long term carbagoline therapy. J Clin Endocinol Metab 2009;94:2428-36.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
|










 Search Pubmed for
Search Pubmed for