|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2014 | Volume
: 9
| Issue : 2 | Page : 70-73 |
|
Scaling up the practice of sanitary refuse disposal in Aba, South Eastern Nigeria
UM Nwosu1, RA Eke2, KA Uwakwe3
1 Department of Nursing Sciences, Abia State University Teaching Hospital, Aba, Abia State, Nigeria
2 Department of Public Health Medicine, Abia State University Teaching Hospital, Aba, Abia State, Nigeria
3 Department of Community Medicine, Imo State University Teaching Hospital, Umuna Orlu, Imo State, Nigeria
| Date of Web Publication | 19-Aug-2014 |
Correspondence Address:
U M Nwosu
21A, Park Road, P.O. Box 3309 Aba, Abia State
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/9783-1230.139166

Background: Scaling up the practice of sanitary refuse disposal is currently a challenge facing Abia State Environmental Protection Agency in Aba. Objectives: The objective was to identify factors contributing to low level practice of sanitary refuse disposal in Aba and to determine the effects of health promotion intervention in addressing these factors. Design: A prospective, interventional study. Setting: Aba North and South Local Government Areas in Aba. Materials and Methods: Interventional study was carried out in two randomly selected communities in Aba March 2013 to September 2013. Sample size of 443 persons was systematically selected for the study. Instrument for data collection was questionnaire. Chi-square and McNemar statistic were used in testing for statistical significance. Results: Factors contributing to low level practice of sanitary refuse disposal in Aba were broadly categorized into four: Ignorance, inadequate sanitary refuse bins at homes and collection centers, poor attitude toward sanitation, delay in refuse evacuation. Conclusion: Health promotion intervention increased the practice of sanitary refuse disposal by 62% and is hereby recommended as a veritable tool for scaling up the practice of sanitary refuse disposal in urban areas. Keywords: Aba, Nigeria, Sanitary refuse disposal, Scaling up
How to cite this article:
Nwosu U M, Eke R A, Uwakwe K A. Scaling up the practice of sanitary refuse disposal in Aba, South Eastern Nigeria. J Med Investig Pract 2014;9:70-3 |
How to cite this URL:
Nwosu U M, Eke R A, Uwakwe K A. Scaling up the practice of sanitary refuse disposal in Aba, South Eastern Nigeria. J Med Investig Pract [serial online] 2014 [cited 2018 Aug 24];9:70-3. Available from: http://www.jomip.org/text.asp?2014/9/2/70/139166 |
| Introduction | |  |
Solid wastes or refuse can be described as substances produced by man that are normally in the solid state and discarded as unwanted. [1],[2],[3] In Aba, sources of refuse generation include homes, markets, industries, and institutions. Refuse consists of organic and inorganic materials of which some are toxic and hazardous. [3],[4],[5],[6],[7],[8] Refuse needs to be sanitarily disposed; otherwise, it becomes a source of disaster and infectious diseases. [9] Indiscriminate disposal of refuse could also lead to fire outbreaks, vehicular accidents, injuries, and eutrophication of rivers. A common feature of most cities in Nigeria and other developing countries is indiscriminate dumping of refuse along major roads, streets, markets, and open spaces. [10]
In Aba, the rate of refuse generation per day appears to be greater than the rate of evacuation to final disposal site, hence mammoth refuse heaps litter the town unattended to for days. The attendant offensive odor from the putrefying refuse heaps that proliferate the city is a source of worry to both residents and visitors. [11] Health risks associated with unsanitary dumping of refuse indiscriminately is enormous and calls for urgent redress.
The purpose of this study is to determine factors contributing to low level practice of sanitary refuse disposal (SRD) in Aba and apply health promotion intervention (HPI) to address these factors so as to scale up the practice of SRD.
| Materials and methods | | |
An interventional study was conducted in Aba from March 2013 to September 2013. Two communities, Ogbor and Ndiegoro were randomly selected from Aba North and Aba South Local Government Areas respectively for the survey. A sample size of 443 persons was systematically selected from a population of 4,443 households enumerated for the study. Instrument for data collection was a pretested interviewer-administered questionnaire. Data were analyzed quantitatively before and after intervention and compared. Chi-square and McNemar statistic were used in testing for statistical significance.
Health promotion intervention activities involved massive community awareness campaign program about health implications of indiscriminate refuse disposal, carried out in the community council hall, market square and primary school. Sanitary refuse bins were distributed to participants at affordable price. Central collection bins that were formerly open were now covered with thick water proof or tarpaulin and the number doubled so as to avoid dumping refuse on the ground and roadsides. Environmental health officers were deployed to ensure regular house-to-house refuse collection and proper dumping inside the bulky bins and not on the ground, gutters/water ways, roadsides, streets and inside Aba River. They were to apprehend defaulters and ensure compliance. At the end of 3 months of interventional activities postintervention questionnaire was administered. Both pre- and post-intervention data generated were analyzed and compared.
| Results | | |
The results of the sociodemographic and economic characteristic of respondents in [Table 1] shows that majority of respondents were within the age bracket of 35-44 years. About 40% had no formal education, whereas the majority of the respondents were traders. About 80% of them lived below N60,000.00/month.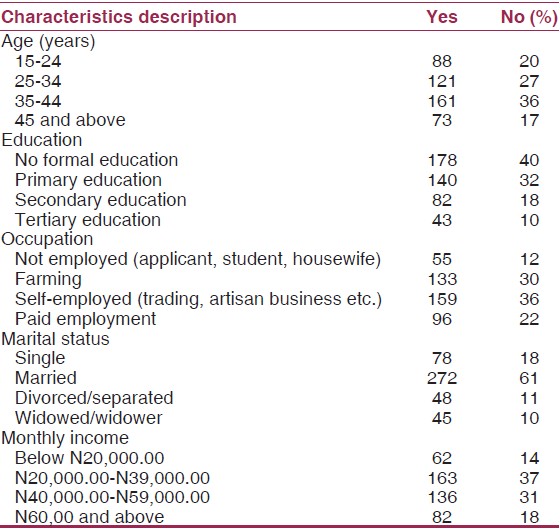 | Table 1: Sociodemographic and economic characteristics of respondents (n=443)
Click here to view |
Before intervention, 12% of the respondents knew the health implications of unsanitary refuse disposal, but after intervention 80% were knowledgeable, giving an increase of 68%. Further analysis using McNemar test statistic yielded 1.7420 an indication that this finding was significant [Table 2].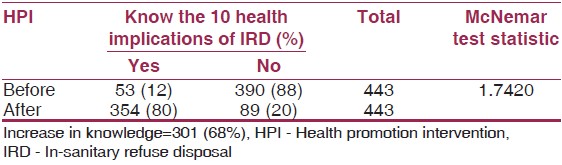 | Table 2: Knowledge of health implications of IRD: Before and after HPI (n=443)
Click here to view |
[Table 3] shows that before intervention 10% of respondents practiced SRD, after intervention, 72% practiced it giving an increase of 62%. McNemar test statistic yielded 0.4629, which is highly significant.
[Table 4] shows influence of knowledge of health implications of unsanitary refuse disposal on the practice of SRD. Before intervention, 10% of those who knew the health implication of unsanitary refuse disposal practiced SRD, whilst those who did not know the health implications of unsanitary refuse disposal did not practice SRD. After intervention, 80% of respondents knew about health implication of unsanitary refuse disposal, but only 72% practiced SRD. The null hypothesis that knowledge of health implication of unsanitary refuse disposal does not influence the practice of SRD was rejected at alpha level of 0.05; we then concluded that knowledge unsanitary disposal influenced the practice of SRD. The result also showed that as knowledge of unsanitary refuse disposal increases, practice of SRD increased [Table 4]. | Table 4: Influence of knowledge of health implications of IRD on practice of SRD (n=443)
Click here to view |
Four broad factors or reasons were identified contributing to low level practice of SRD, in Aba. These were ignorance, inadequate sanitary refuse bins at homes and collection centers, poor attitude toward sanitation, delay in refuse evacuation [Table 5]. A critical look at [Table 5] shows that factors/reasons, which contributed to low level practice of SRD before HPI were drastically reduced after intervention, while factors that promotes SRD were highly increased in number after intervention [Table 5].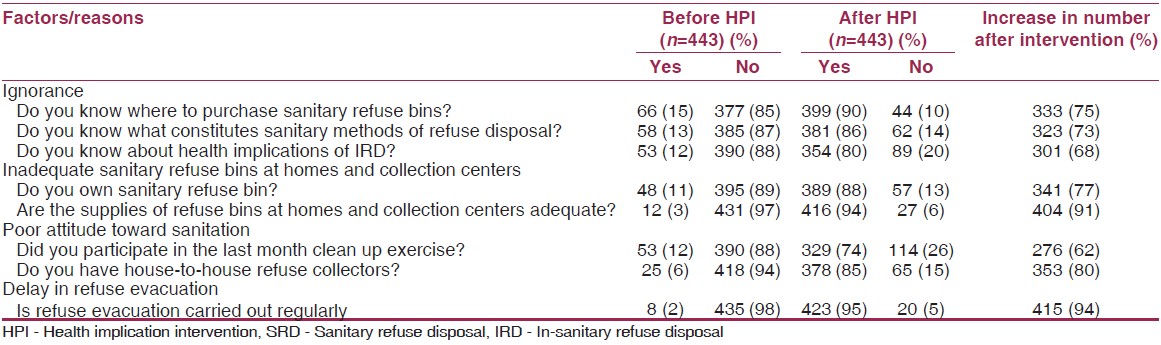 | Table 5: Identified factors/reasons contributing to low level practice of SRD
Click here to view |
| Discussion | | |
The findings in [Table 2] and [Table 4] that respondents who were not knowledgeable in health implications of in-sanitary refuse disposal did not practice SRD, is in agreement with earlier report, that knowledge of health impacts associated with improper refuse disposal was an important tool in the right practice of waste management. [10],[11],[12],[13],[14],[15] Knowledge of health implications of unsanitary refuse disposal was positively associated with the practice of SRD. [10],[11] Earlier researchers had reported that individuals' change in attitude and behavior depends on quality of education, information and behavioral communication received. [16],[17],[18],[19]
The findings in [Table 3] that practice of SRD significantly increased from 10% before intervention to 72% after intervention is a clear evidence-based effect of HPI in scaling the practice of SRD. It is also likely that increase in knowledge about public health implications of unsanitary refuse disposal during the campaign, brought about the increase in the practice of SRD. It has also been documented in various research findings that effective sanitary management of domestic wastes starts from ownership of sanitary refuse bins at homes for storage of refuse. [10],[11],[12],[13],[14],[15],[20] HPI, which significantly increased ownership of sanitary refuse bin by 52% [Table 5] has invariably increased the practice of SRD by same margin [Table 3] and [Table 5]. This finding corroborated with the report that ownership of sanitary dust bin in the household was closely associated with the practice of sanitary solid waste disposal. [8],[9],[10],[11]
The findings in [Table 5] that factors such as ignorance about what constituted sanitary methods of refuse disposal, lack of knowledge about public health implications of unsanitary refuse disposal, lack of knowledge about where to buy sanitary refuse bin constituted a barrier to practice of SRD is in agreement with similar works done elsewhere in developing countries. [10],[11],[12],[13],[14],[15],[20] The reason could be as a result of low level of formal education of respondents. About 40% of the respondents had no formal education [Table 1]. The findings that inadequate sanitary refuse bins at homes and collection centers, poor attitude towards sanitation were other factors for low level practice of SRD tallied with other works done elsewhere in Nigeria. [9],[10],[11] These could be as a result of respondents not participating in the monthly, national clean up exercise. These problems were addressed by providing them with refuse bins at a subsidized rate. Lack of genuine community participation and commitment to monthly national clean up exercises was addressed during the HPI activities. The findings that children were saddled with the duty of carting away refuse from homes constituted barriers to SRD. These children viewed the collection centers as distant and sometimes dump the refuse indiscriminately. This barrier was tackled by providing house-to-house refuse collectors. Delay in evacuating refuse from collection centers to final dumping site was another factor militating against SRD. People, who come to dump their refuse into the central collection bulky bin, decide to dump them on the road when the bins were filled and left unattended to by the agency responsible for refuse collection for days. These factors or reasons were addressed during the HPI by providing more bulky bins with cover at the collection centers. The findings that HPI drastically reduced the identified factors or reasons for not practicing SRD to the barest minimum is indicative of the effectiveness of this strategy in scaling up SRD by 62%.
| Conclusion | | |
The practice of SRD before intervention was very low at 10%. It increased to 72%, following intervention, showing a significant increase of about 62%.
Health promotion intervention is hereby recommended as a proven strategy for scaling up the practice of SRD in Aba and similar urban areas in Nigeria and other developing countries, experiencing indiscriminate dumping of refuse.
| References | | |
| 1. | Obionu CN. Primary Health Care for Developing Countries. Enugu: Ezu Book Publisher; 2007. 
|
| 2. | Lucas AO, Gilles HM. Short Textbook of Public Health Medicines for the Tropics Revised. 4 th ed. Malta: Book Power Publishers; 2007.
|
| 3. | Amadi AN. Modern Environmental Sanitation. Owerri: Nationwide Printers and Publishing Co. Ltd.; 2009.
|
| 4. | World Health Organization (WHO). Poor Sanitation: The Global Magnitude of the Problem. Environ Health News Lett 1997;6:1-2.
|
| 5. | Asonmani-Boteng R, Haight M. Re-using organic solid waste in urban farming in African cities: A challenge for urban planning. Documents 2008;11:14.
|
| 6. | USEPA. Wastes: Non-Hazardous Waste Municipal Solid Waste, 2008. Available from: http://www.epa.ov/waste/nonhaz/minicipal/index.htm. [Last accessed on 2013 Oct 04].
|
| 7. | Waste Info Sheet. Waste Disposal Methods: Advantages and disadvantages; 2009. Available from: file://d./assign/wastediposal/methods.hm. [Last accessed on 2013 Oct 04].
|
| 8. | Wikipedia; Waste Management, 1990. Available from: http://www.en.wikipedia.org/wiki/waste management. [Last accessed on 2013 Oct 06].
|
| 9. | Modebe I, Onyenoro UU, Ezeama N, Ogbuagu CN, Agam NE. Public health implication of household solid waste management in Awka South East Nigeria. Internet J Public Health 2011;1:1-8. [Last accessed on 2013 Oct 04].
|
| 10. | Uwakwe FE, Iwuala MO. Studies on the characteristics and public health implications of Waste Dump Sites in Owerri, Imo State, Nigeria. Int Environ Health Hum Dev 2012;13:1-2.
|
| 11. | Nduka I, Nwosu UM, Eke RA. Studies of solid waste disposal in Aba, Nigeria, with recommendations for a sustainable sanitary solid waste disposal system. Int J Environ Health Hum Dev 2013;14:In Press.
|
| 12. | Nwankwo BO. Solid waste generation and management among traders in Owerri municipal markets, Imo State. J Environ Health 2008;5:58-63.
|
| 13. | Oil, Resource and Allied Investment Limited. The Study of Solid Waste Generation and Management in Owerri Metropolitan City. A Consultancy Service Agreement Report Presented to the Ministry of Petroleum and Environment. Owerri; August 13 th , 2008.
|
| 14. | Boadi KO, Kuitunen M. Environmental and health impacts of household solid waste handling and disposal practices in third world cities: The case of the Accra Metropolitan Area, Ghana. J Environ Health 2005;68:32-6.
|
| 15. | Imoh E, Emmanuel PU. Domestic solid waste management in a rapidly growing Nigerian City of Uyo. J Hum Ecol 2001;36:229-35.
|
| 16. | Albert Bandura Social Learning Theory. Perspectives › Behaviorism, Simply Psychology, 1977. Available from: http://www.simplypsychology.org. [Last accessed on 2013 Oct 09].
|
| 17. | Anonymous. The Health Belief Model (HBM). Home Health Communication. Theory at a Glance: A Guide for Health Promotion Practice, 1997. Available from: http://www.utwente.nl. [Last accessed on 2013 Oct 09].
|
| 18. | Federal Ministry of Health (FMOH). National Health Promotion Policy (NHPP). Abuja: Nigeria; 2006.
|
| 19. | World Health Organization (WHO). Bangkok Declaration on Health Promotion. Geneva; 2005.
|
| 20. | Babayemi JO, Dauda KT. Evaluation of solid waste generation categories and disposal. J Appl Sci Environ Manage 2009;13:83-8.
|
[Table 1], [Table 2], [Table 3], [Table 4], [Table 5]
|









 Search Pubmed for
Search Pubmed for