|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2014 | Volume
: 9
| Issue : 3 | Page : 116-119 |
|
Pattern of temporomandibular pain dysfunction syndrome in a Nigerian population
Osawe Felix Omoregie, Mercy Okoh
Department of Oral Pathology and Oral Medicine, University of Benin Teaching Hospital, Benin City, Nigeria
| Date of Web Publication | 15-Nov-2014 |
Correspondence Address:
Mercy Okoh
Department of Oral Pathology and Oral Medicine, University of Benin Teaching Hospital, Benin City
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/9783-1230.144773

Background: Temporomandibular joint pain dysfunction syndrome (TMJPDS) is the commonest disorder of the joint. Objective: This study aims to determine the prevalence, the clinical profile and the response to medical treatment by patients suffering from TMJPDS in a Nigerian population.
Materials and Methods: A retrospective review of the clinical records of all patients seen in Oral Medicine Clinic, University of Benin Teaching Hospital, Benin City, Nigeria. The age, gender, trigger factors, sites, medications and follow up visits of the patients selected were analyzed. Results: There were 24 (8.4%) cases of TMJPDS among the 287 patients seen during the period under review. There was no gender predilection; the mean age was 43 + 1.7 years and the peak age group was the 5 th decade of life (n = 6, 25.0%). Left sided TMJPDS was the most frequent presentation (n = 13, 54.2%) and chewing was the commonest trigger factor (n = 10, 41.6%). Most patient were placed on diazepam (n = 18, 75.0%) combined with paracetamol (n = 7, 29.2%) or norgesic (n = 5, 20.8%) or cataflam (n = 3, 12.5%) or Ibuprofen (n = 1, 4.2%). Early response to medical treatment was observed within 3 weeks (n = 14, 58.3%), especially among the patients suffering from left sided TMJPDS (n = 10, 41.7%) (P = 0.005). Conclusion: This study showed a low prevalence of TMJPDS and a predilection of TMJPDS for the left side among adult patients. Preliminary findings suggest that diazepam combined with analgesic were effective medical treatment for TMJPDS. Keywords: Medical treatment, Orofacial pain, Temporomandibular joint
How to cite this article:
Omoregie OF, Okoh M. Pattern of temporomandibular pain dysfunction syndrome in a Nigerian population. J Med Investig Pract 2014;9:116-9 |
How to cite this URL:
Omoregie OF, Okoh M. Pattern of temporomandibular pain dysfunction syndrome in a Nigerian population. J Med Investig Pract [serial online] 2014 [cited 2018 Aug 24];9:116-9. Available from: http://www.jomip.org/text.asp?2014/9/3/116/144773 |
| Introduction | |  |
Temporomandibular joint pain dysfunction syndrome (TMJPDS) is the commonest disorder of the joint. [1] The pain is dull and unilateral, centered in the temple, above and behind the eye, in and around the ear. The pain may be associated with instability of the temporo-mandibular joint (TMJ), crepitus, or clicking with movement of the jaw. [2] Clinical signs include tenderness of the masticatory muscles, the ear canal or the joint itself, restricted opening of the jaw or lateral deviation on opening, and a normal neurological examination. [2]
Temporomandibular joint symptoms are relatively common, occurring in 10-25% of the population; only about 5% of people with symptoms will seek treatment. [3] Temporomandibular disorders may occur at any age, but are more common in women and in early adulthood. [3],[4] A relatively higher prevalence of TMJPDS is reported among Nigerians compared to Western societies. [5] Most subjects in a Nigerian study presented with mild symptoms and signs of TMJPDS, [5] while 5-10% among 75% of US population with TMJ symptoms and signs are diagnosed with TMJPDS. [6]
The condition is currently being managed by nonsurgical and surgical approaches. [7],[8],[9] Initial care is, usually, with conservative treatment, which is effective in most cases. Psychological aspects of pain management are important, [10] as with other chronic pain and somatization disorders. Surgical intervention is often indicated for long standing cases and in some selected cases, where there is structural pathology not responding to conservative treatment. [11]
The nonsurgical approach in the management of TMJPDS involves the non-drug treatment [ 4],[12] such as explanation and reassurance, adequate rest, self-care (soft diet, avoiding wide yawning, singing, chewing gum, moist heat and massage of masticatory muscle, use of relaxation techniques, identifying and reducing life stresses). Others non-surgical treatments are use of occlusal splints (bite guards for patients with malocclusion or bruxism), [13],[14] acupuncture, [15] psychosocial support and psychotherapy, [10] behavioural techniques (postural training, biofeedback and proprioceptive retraining), [16],[17] and drug treatment [12] such as analgesics (non-steroidal anti-inflammatory drugs [NSAIDs]), muscle relaxants (benzodiazepines), and antidepressants (tricyclic antidepressants) especially in patients with psychiatric disorder. [18]
There is dearth of literature on studies that evaluate medical treatment of TMJPDS in our environment. This study aims to determine the prevalence, the clinical profile and the response to medical treatment by patients suffering from TMJPDS in a Nigerian population.
| Materials and methods | | |
Approval to carry out this study was obtained from the Hospital Ethical Committee. A 3-year retrospective review of the clinical records of all patients seen between September 2009 and May 2012, in Oral Medicine Clinic, University of Benin Teaching Hospital, Benin City, Nigeria was performed.
Patients with TMJPDS were selected. The age, gender, trigger factors, sites, medications and follow up visits of the patients selected were analyzed. Evaluation of response to medical treatment was based on subjective (no complaint of pain by patients) and objective (no sign of tenderness elicited by clinician) during follow up period. Pearson's Chi-square correlation was performed for the variables, with confidence level set at 95%, and P < 0.05 was considered significant.
| Results | | |
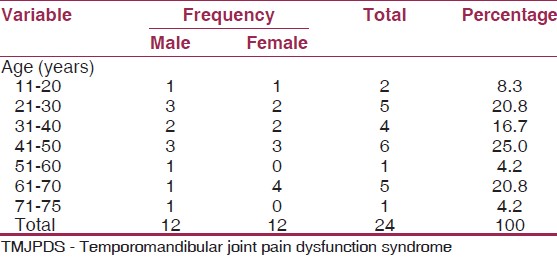
Demographic data of subjects
There were 24 (8.4%) cases of TMJPDS among the 287 patients seen during the period under review. There was no gender predilection; the mean age was 43 + 1.7 years and the peak age group was the 5 th decade of life (n = 6, 25.0%) [Table 1].
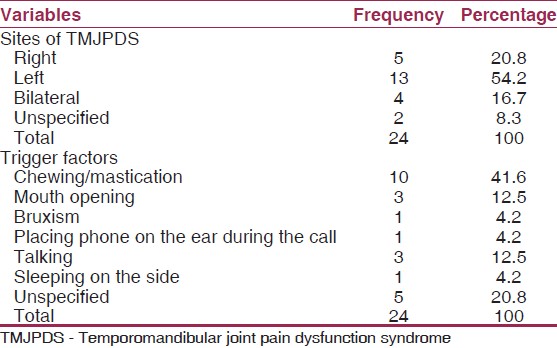
Sites and trigger factors for temporomandibular joint pain dysfunction syndrome
Left sided TMJPDS was the most frequent presentation (n = 13, 54.2%). Chewing/mastication was the commonest trigger factor (n = 10, 41.6%), while 5 (20.8%) cases had no specific trigger factor. Other parafunctional habits associated as trigger factors were bruxism (n = 1, 4.2%) and placing cell phone on the ear during calls (n = 1, 4.2%) [Table 2].
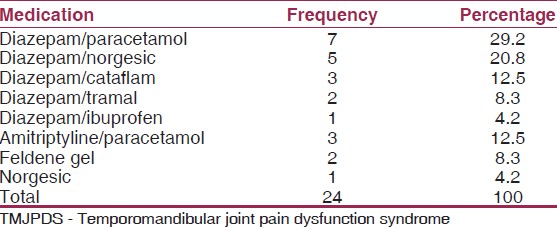
Treatment regimen for patients
Most patients were placed on diazepam, 10 mg nocte daily (n = 18, 75.0%), combined with paracetamol, 1000 mg 8 hourly (n = 7, 29.2%), or norgesic (orphenadrine citrate 25 mg, aspirin 385 mg, and caffeine 30 mg) 8 hourly (n = 5, 20.8%), or cataflam 50 mg 12 hourly (n = 3, 12.5%) or tramal, 100 mg 8 hourly (n = 2, 8.3%) or ibuprofen, 400 mg 12 hourly (n = 1, 4,2%). Amitriptyline, 50 mg nocte was administered to 3 (12.5%) patients who scored high on World Health Organization well-being index and depression scale (1998) [19] [Table 3].
Response to treatment
Early response to medical treatment was observed within 3 weeks among most of these patients (n = 14, 58.3%), especially among patients in the 5 th decade of life (n = 4, 16.7%), in males (n = 9, 37.5%), those with mastication as trigger factor (n = 9, 37.5%) and patients suffering from left sided TMJPDS (n = 10, 41.7%) (P = 0.005). The early response in 3 weeks was observed among patients placed on the following medication: Diazepam and norgesic (n = 4, 16.7%), diazepam and paracetamol (n = 3, 12.5%), diazepam and cataflam (n = 3, 12.5%), diazepam and tramal (n = 1, 4.2%), norgesic (n = 1, 4.2%), amitriptyline and paracetamol (n = 1, 4.2%) and feldene gel (n = 1, 4.2%).
| Discussion | | |
Patients with TMJPDS are faced with long-term problems of pain management. Early medical treatment may help to prevent the use of more invasive treatments with harmful potential. [20] This study showed a low prevalence of TMJPDS comparable to what was previously reported in this Centre and among North Americans. [2] In contrast to the previous report of TMJPDS predilection for females between 20 and 40 years, [6] no gender predilection was observed, and the patients were slightly older in this study. This variation in gender predilection may have been influenced by the fewer number patients in this study. Similar to a previous report, [21] unilateral (left sided) TMJPDS was the most frequent presentation, associated with chewing/mastication as the commonest trigger factor. The reason for predilection of TMPDS for the left side is unclear; however, it may be due to patient's preference for a unilateral mastication with the left side of the jaws.
Non-steroidal anti-inflammatory drugs and benzodiazepines are the mainstays of treatment for TMJPDS. [22] Patients eventually may require tricyclics antidepressants, opioids, muscle relaxants, or steroid (intra-articular) therapy for protracted pain syndromes. [8] More than half of the patients in this study, particularly males, those with mastication as the trigger factor and those with left-sided TMJPDS responded well to the combination of NSAIDS and muscle relaxant treatment within 3 weeks of follow up. However, TMJPDS patients are reported to also benefit from gentle stretching or relaxation exercises for the jaw. [16]
Temporomandibular joint pain dysfunction syndrome patients may have a history of stress and pains elsewhere in the body. These patients become symptom-free in response to reassurance and a course of tricyclic antidepressant drug therapy when used as a muscle relaxant and central analgesic. [8] Harris reported, [23] that some patients will benefit from psychiatric help. Some of the patients in this study were diagnosed of clinical depression associated with TMJPDS, following psychological evaluation and were treated with anti-depressant. Similarly, Saheeb and Otakpor [18] reported a higher prevalence of TMJPDS among psychiatric patients compared to control subjects and recommended a multidisciplinary approach in the management of TMJPDS. Furthermore, Vimpari et al. [24] reported a higher prevalence of subjective symptoms of TMJPDS in depressed patients. These findings further emphasize the need for oral medical practitioners to co-manage these patients with mental health experts.
Although, a smaller proportion of TMJPDS patients may have secondary joint disturbances requiring surgery, [11] attempt at conservative management, particularly medical treatment is recommended, before considering invasive therapy. Also, supportive non-invasive treatment may be required before and after surgical treatment. [25] Surgical techniques should be reserved for cases where other therapeutic modalities have failed. The National Institute of Dental and Craniofacial Research recommend that treatments for TMJPDS should not permanently alter the jaw or teeth, but need to be reversible. [26],[27]
| Conclusion | | |
This study showed a low prevalence of TMJPDS and a predilection of TMJPDS for the left side among adult patients. Preliminary findings from this study suggest that benzodiazepines (muscle relaxant and anxiolytic) combined with analgesics (NSAIDS) were effective medical treatment for TMJPDS. Conservative management, particularly medical treatment of TMJPDS is recommended, before considering invasive therapy for unresponsive patients. A multidisciplinary approach involving oral medical practitioners and mental health experts is also recommended in the management of TMJPDS with associated psychiatric symptoms.
| References | | |
| 1. | Ozkan F, Cakir Özkan N, Erkorkmaz U. Trigger point injection therapy in the management of myofascial temporomandibular pain. Agri 2011;23:119-25.  |
| 2. | Guralnick W, Kaban LB, Merrill RG. Temporomandibular-joint afflictions. N Engl J Med 1978;299:123-9. |
| 3. | LeResche L. Epidemiology of temporomandibular disorders: Implications for the investigation of etiologic factors. Crit Rev Oral Biol Med 1997;8:291-305. |
| 4. | Dimitroulis G. Temporomandibular disorders: A clinical update. BMJ 1998;317:190-4. |
| 5. | Otuyemi OD, Owotade FJ, Ugboko VI, Ndukwe KC, Olusile OA. Prevalence of signs and symptoms of temporomandibular disorders in young Nigerian adults. J Orthod 2000;27:61-5. |
| 6. | Guardia CF, Egan RA. Temporomandibular Disorders. Available from: http://www.emedicine.medscape.com/article/1143410-overview. [Last updated on 2012 Jan 11; Last accessed on 2012 Aug 16]. |
| 7. | Dionne RA. Pharmacologic treatments for temporomandibular disorders. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1997;83:134-42. |
| 8. | American Academy of Family Physicians. Temporomandibular joint (TMJ) pain. Am Fam Physician 2007;76:1483-4. |
| 9. | Dym H, Israel H. Diagnosis and treatment of temporomandibular disorders. Dent Clin North Am 2012;56:149-61, ix. |
| 10. | Sherman JJ, Turk DC. Nonpharmacologic approaches to the management of myofascial temporomandibular disorders. Curr Pain Headache Rep 2001;5:421-31. |
| 11. | Greenberg SA, Jacobs JS, Bessette RW. Temporomandibular joint dysfunction: Evaluation and treatment. Clin Plast Surg 1989;16:707-24. |
| 12. | Scrivani SJ, Keith DA, Kaban LB. Temporomandibular disorders. N Engl J Med 2008;359:2693-705. |
| 13. | Koh H, Robinson PG. Occlusal adjustment for treating and preventing temporomandibular joint disorders. Cochrane Database Syst Rev 2003:CD003812. |
| 14. | Al-Ani MZ, Davies SJ, Gray RJ, Sloan P, Glenny AM. Stabilisation splint therapy for temporomandibular pain dysfunction syndrome. Cochrane Database Syst Rev 2004:CD002778. |
| 15. | Fink M, Rosted P, Bernateck M, Stiesch-Scholz M, Karst M. Acupuncture in the treatment of painful dysfunction of the temporomandibular joint - A review of the literature. Forsch Komplementmed 2006;13:109-15. |
| 16. | Michelotti A, de Wijer A, Steenks M, Farella M. Home-exercise regimes for the management of non-specific temporomandibular disorders. J Oral Rehabil 2005;32:779-85. |
| 17. | Medlicott MS, Harris SR. A systematic review of the effectiveness of exercise, manual therapy, electrotherapy, relaxation training, and biofeedback in the management of temporomandibular disorder. Phys Ther 2006;86:955-73. |
| 18. | Saheeb BD, Otakpor AN. Co-morbid psychiatric disorders in Nigerian patients suffering temporomandibular joint pain and dysfunction. Niger J Clin Pract 2005;8:23-8. [ PUBMED] |
| 19. | World Health Report: Mastering Depression in Primary Care (Version 2.2). WHO, Regional Office for Europe Psychiatric Research. Frederiksborg General Hospital. The World Health Organization; 1998. |
| 20. | Marbach JJ. Temporomandibular pain and dysfunction syndrome. History, physical examination, and treatment. Rheum Dis Clin North Am 1996;22:477-98. |
| 21. | Saheeb BD. Prevalence of oral and parafunctional habits in Nigerian patients suffering temporomandibular joint pain and dysfunction. J Biomed Sci 2005;4:59-64. |
| 22. | Uyanik JM, Murphy E. Evaluation and management of TMDs, Part 1. History, epidemiology, classification, anatomy, and patient evaluation. Dent Today 2003;22:140-5. |
| 23. | Harris M. Medical versus surgical management of temporomandibular joint pain and dysfunction. Br J Oral Maxillofac Surg 1987;25:113-20. |
| 24. | Vimpari SS, Knuuttila ML, Sakki TK, Kivelä SL. Depressive symptoms associated with symptoms of the temporomandibular joint pain and dysfunction syndrome. Psychosom Med 1995;57:439-44. |
| 25. | Dolwick MF. Temporomandibular joint surgery for internal derangement. Dent Clin North Am 2007;51:195-208, vii. |
| 26. | Lipton JA, Ship JA, Larach-Robinson D. Estimated prevalence and distribution of reported orofacial pain in the United States. J Am Dent Assoc 1993;124:115-21. |
| 27. | National Institutes of Health Technology Assessment Conference Statement. Management of Temporomandibular Disorders. Washington, D.C: Government Printing Office; 1996. |
[Table 1], [Table 2], [Table 3]
|









 Search Pubmed for
Search Pubmed for