|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2014 | Volume
: 9
| Issue : 3 | Page : 120-125 |
|
Prevalence of hearing impairment amongst primary school children in Port-Harcourt, Rivers State: Implication for strengthening of school health programme in Nigeria
I Nduka1, EJ Aitafo2, EC Nduka3
1 Department of Community Medicine, Abia State University Teaching Hospital, Aba, Nigeria
2 Department of Pediatrics, Braithwaite Memorial Hospital, Port Harcourt, Rivers State, Nigeria
3 Department of Obstetrics and Gynaecology, Federal Medical Centre, Umuahia, Abia State, Nigeria
| Date of Web Publication | 15-Nov-2014 |
Correspondence Address:
I Nduka
Department of Community Medicine, Abia State University Uturu, Abia State
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/9783-1230.144774

Introduction: Hearing impairment is the most frequent sensory deficit in humans with a higher prevalence in developing countries. Materials and Methods: Hearing assessment was carried out in lower primary school children in Port Harcourt City (PHC) between January 10th and May 21, 2010. A total of 802 school children were selected by multistage sampling technique, consisting of 405 (50.5%) males and 397 (49.5%) females. Screening for hearing impairment was done using pure tone audiometry after an otoscopic examination. The prevalence of hearing impairment was found to be 29.4%. Result: Hearing impairment was significantly more prevalent (32.8%) among children in the older age group (11-13 years) than in children 5-7 years of age (24.2%). Most (58.9%) of the children had slight hearing impairment (16-25 dB HL). Unilateral hearing loss was seen in 54.1% of the children while 45.9% had bilateral hearing loss. Conclusion /Recommendation: The study revealed that hearing impairment is common among primary school children in PHC. We therefore recommend that routine hearing screening should be part of the school health program at school entry for primary school pupils, for early detection and treatment of hearing impairment to enhance total development of the child and maximize academic performance. Keywords: Hearing impairment, Nigeria, Prevalence, Primary school children
How to cite this article:
Nduka I, Aitafo E J, Nduka E C. Prevalence of hearing impairment amongst primary school children in Port-Harcourt, Rivers State: Implication for strengthening of school health programme in Nigeria. J Med Investig Pract 2014;9:120-5 |
How to cite this URL:
Nduka I, Aitafo E J, Nduka E C. Prevalence of hearing impairment amongst primary school children in Port-Harcourt, Rivers State: Implication for strengthening of school health programme in Nigeria. J Med Investig Pract [serial online] 2014 [cited 2018 Aug 24];9:120-5. Available from: http://www.jomip.org/text.asp?2014/9/3/120/144774 |
| Introduction | |  |
Hearing loss is the most frequent sensory deficit in human populations affecting over 250 million people in the world, [1],[2] with at least two-thirds residing in developing countries. [3] In developed countries, including the USA, the prevalence of hearing loss among school children was found to be between 0.05% and 0.7%, with a higher prevalence seen amongst African-American children. [2] Studies done in Africa have shown that between 2% (South Africa) [2] and 25.6% (Egypt) [4] of school children have varying degrees of hearing impairment. A study done amongst school entrants in Lagos; Nigeria showed a prevalence of 13.9%. [5]
Hearing loss may result from disorders affecting the inner ear or cochlea (sensory loss), the auditory nerve (neural loss), or the middle ear and/or outer ear (conductive loss). Mixed hearing loss (MHL) may develop if conductive hearing loss (CHL) co-exist with sensory hearing loss. [6],[7] According to the World Health Organization, hearing loss could be classified by the hearing threshold level using audiometry, as the average of four frequencies - 0.5, 1, 2, and 4 kHz in the better ear. [8] The amount or degree of hearing loss may range from slight (16-25 dB HL), mild (26-40 dB HL), moderate (41-70 dB HL), severe (71-95 dB HL), to profound (>95 dB HL). [2],[5] Hearing loss has been found to be either congenital (genetic or non-genetic) or acquired. Significant hearing loss is present in 1-6/1000 newborns. [7] However, some congenital hearing loss may not become evident until later in childhood.
Early detection of hearing loss in newborns and young children is vital for effective aural rehabilitation and educational intervention. Screening for hearing impairment at school entry has been recommended for early detection and rehabilitation among primary school children in developing countries. [9],[10] However, many children in these countries are missed due to lack of resources and skill among parents and teachers. [11] Thus, some children in lower primary schools have varying degrees of undetected hearing impairment. Hearing loss has been reported to result in speech and language delay, difficulties in parent-child, peer-child, and child-teacher interactions. It leads to poor school performance, low self-esteem and thus poor psycho-social/intellectual development of the child. [12] The adverse impact of hearing impairment on the acquisition of linguistic skills in children and their psycho-social development are well established. [2],[3],[5],[6],[12] Hearing impairment results in the inability to interpret speech sounds, often producing a reduced ability to communicate, delay in language acquisition, economic and educational disadvantages, social isolation and stigmatization. [2],[12] This places some limitations on educational and economic pursuits essential to achieving a good quality of life.
In Nigeria, the prevalence of hearing loss in school pupils is 13.9% constituting 15-18% of hearing loss in the general population in Nigeria. [5] Among the general population, 1/1000 people have one form of hearing loss or the other. [5] Hearing loss unrecognized by parents at home can be detected at pre-entry medical inspection in schools; yet, this activity has been reported to be missing in most schools in Nigeria. [13],[14] The early detection and intervention for disabilities among school children cannot be achieved without a school programme that is well-planned, implemented and evaluated. The National school health policy was established in November/December 2006. The policy has as part of its components; school health services which are designed to examine school children at entry and midway into school. This component of school health is rarely practiced in schools. [3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14],[15] The major factor limiting against the full practice of screening at pre-entry stage is a lack of knowledge among teachers in schools as reported by the study. [16] The strengthening of school health programme will be of paramount benefit in early detection and rehabilitation of school children with hearing loss who were missed at home by their parents and care givers.
This study was, therefore, conducted to determine the prevalence of hearing loss among primary school children in Port-Harcourt, Rivers state Nigeria. The findings of this study will add to existing literature on the need to strengthen the school health policy in Nigeria.
| Materials and methods | | |
Study area
The study was conducted in Port Harcourt City (PHC), the capital of Rivers State of Nigeria. It is located in the South-South geopolitical zone of Nigeria. PHC is one of the 23 local government areas of Rivers State. It is divided into three main school districts: Township, Diobu and Trans Amadi. There are a total of 139 primary schools in PHC; 71 public schools and 68 private schools, [17] giving a public to private school ratio of 1.1:1. Diobu district has the largest number of schools (67 schools-35 public and 32 private) followed by Township (with 52 schools-25 public and 27 private). Trans Amadi has the least, 20 schools with 11 public and 9 private schools.
Study population
The study was conducted among primary school pupils in PHC, Rivers State, Nigeria.
Inclusion criteria
This included schools with no practice of school health services and who have not had a school health medical examination of the pupils in the last 6 months prior to the study period. Only children whose parents gave written consent were allowed to participate in the study.
Exclusion criteria
The special schools for the handicapped were excluded from the study.
Study design
This was a descriptive cross-sectional study to determine the prevalence of hearing loss among school children in Rivers with a view to proffering suggestions towards strengthening the school health programme in Nigeria.
Sampling technique
Using the formula rpq/e/(1.96) 2 (P = 13.9% hearing loss 5 ) for calculating the minimum sample size, 735 was derived.
Multistage sampling technique was used to select pupils for the study. A list of all the primary schools in PHC obtained from the Rivers State Ministry of Education with their student population formed the sample frame.
Stage 1 (Distribution into the three school districts of Port Harcourt City)
The 139 primary schools listed were shared into the 3 school districts of Port Harcourt: Diobu-67, Township-52, and Trans Amadi-20. This translated to a ratio of 3:2.5:1.
Stage 2 (Stratification into public and private schools)
The schools within each district were then further stratified into public and private schools - Diobu district has 35 public and 32 private schools; Township district has 25 public and 27 private schools while Trans Amadi has 11 public and 9 private schools.
Stage 3 (Selection of schools)
Based on the ratio of schools in each district, 6 schools (3 public and 3 private); 5 schools (3 public and 2 private); and 2 schools (1 public and 1 private) were selected by simple random sampling from Diobu, Township, and Trans Amadi districts respectively.
Stage 4 (Selection of pupils)
A total of 13 schools were selected, comprising of 7 public and 6 private schools. At each selected school, one arm was randomly selected from each class of primary 1, 2 and 3 for the study. A total of 40 pupils were selected randomly from each arm in public schools, and 20 pupils from each arm in private schools. This gave a total of 1200 pupils selected for the study.
Ethical consideration
Ethical clearance was obtained from the Ethics Committee of the University of Port Harcourt Teaching Hospital. The Rivers State Ministry of Education and head teachers of the recruited schools were notified, and permission obtained for the study. Consent forms were given to the pupils for parents to indicate interest and permit their children/wards to participate in the study.
Data collection tools and method
Data collection was done by a team of researchers comprising five doctors and a specialist otolaryngologist within four months of same academic school year. The principal researcher was trained on the use of the otoscope and audiometer. The research assistants were in turn trained by the principal investigator who also clearly explained the objectives of the study to the rest of the team. A pilot study was carried out on 20 primary school pupils in another Local Government area (Obio-Akpor). A structured questionnaire was distributed to parents to ascertain medical, social and family status of the children. Consent forms were also given to parents with detailed information of the scope of the study. The pupils whose parents signed the consent form were recruited into the study. The pupils were weighed standing on a portable bathroom scale (Hana scale, model BR-9011) with their shoes off and wearing only their uniforms. The scales were regularly checked for zero adjustments before and after each reading. In taking the height, the subjects were made to stand straight with their shoes off and head held erect such that the external auditory meatus and the lower border of the orbit were in one horizontal plane (Frankfurt plane). The buttocks, shoulder blades, and heels touched the measurement surface with knees and legs together, and arms hanging naturally by the side. A movable triangular headboard was brought against the crown of the head, and the height measurement read off at the maximum inspiration to the nearest centimeter. All measurements were done twice, and the average taken.
After this, every child had a quick ear, nose and throat inspection (using a pen torch and disposable spatula), and otoscopic examination done by the researcher and a senior registrar in the ENT department. Pupils with the presence of wax were re-examined by the senior registrar in the ENT department, and the wax removed immediately in the school. They were seen the following week for audiometry. The ear drums were classified as abnormal if there was the perforation, hyperaemia, retraction or scarring.
The pupils without wax were then taken to a quiet location, mainly the school library or the head teacher's office for audiometry. The ambient noise was measured with a sound level meter and if found to be acceptable (<50 dB) [5],[18] the venue was used. The pre-calibrated pure tone audiometer used (Madsen 1004) had a noise-reducing headset providing extra attenuation of about 25 dB to outside noise thus bringing the ambient noise further within the acceptable range. The tests tones were presented to each child at the various tests frequencies (0.5, 1.0, 2.0 and 4.0 kHz) starting with an intensity level of 40 dB and adjusted upwards or downwards until <15 dB. Each ear was tested separately using the specialized earphones. The child was instructed to listen carefully and raise the appropriate hand or bang the table each time he or she heard the tone. The children were encouraged to view the test as a game to reduce anxiety. A child was considered to have failed the test, and thus be hearing impaired, if he failed to respond to any of the frequencies tested in at least one ear. Such children were then screened again using a special head set for bone conduction. The various tests frequencies were once again presented using the pure tone audiometer. Where both air and bone conduction were abnormal (>15 dB HL) but equal, the child had sensorineural hearing loss. Where bone conduction was normal, but air conduction was ≥ by 15 dB HL, the child had CHL. Where both air and bone conduction were abnormal and unequal, the child had MHL. On the average 12 pupils were examined in a day, with an examination of each pupil lasting approximately 20 min.
Children who failed the audiometric test (i.e. those considered as being hearing impaired) were subsequently referred to the University of Port Harcourt Teaching Hospital to see an Otorhinolaryngologist for further audiological assessment and expert management. Teachers were encouraged to act as constant reminders to the parents of these children.
Data entry and analysis
All data entry and analysis were done using SPSS statistical software version 17.0 (Chicago) [19] and P < 0.05 considered as statistically significant. Data were presented as tables in simple proportions, and comparisons of sub groups carried out with Chi-square test.
| Result | | |
Of the 1200 consent forms given to pupils for their parents, 802 were returned signed, consenting to participate in the study. These pupils were thus recruited into the study. Four hundred and sixty-one (57.5%) were from public schools and 341 (42.5%) of private schools. The mean age of the participants was 8.6 years ± 2.3 years. Majority of the pupils, 554 (69.1%) were of normal weight whereas 20.2% underweight [Table 1] and [Table 2].
Out of 802 pupils screened, 236 (29.4%) had hearing impairment, of which 101 (42.8%) were males and 135 (57.2%) females. Gender-specific hearing impairment, showed that females had a higher prevalence of impaired hearing than the males; 34.0% and 24.9% respectively. This difference was statistically significant P = 0.003. Age group 11-13 years had the highest prevalence, 83 (32.8%) [Table 3] and [Table 4].
Among the public and private schools, the prevalence was higher in public than in the private schools; 139 (58.9%) and 97 (41.1%) respectively. Public schools (30.2%), had a higher prevalence of hearing impairment than private schools, and this difference was not statistically significant χ2 = 0.275, P = 0.328 [Table 5]. The prevalence of hearing loss among children according to nutritional status is shown in [Table 6]. Among pupils of normal weight, 30.3% had hearing impairment whereas 26.5% of the underweight had hearing impairment. The differences observed were not statistically significant χ2 = 2.271, P = 0.437. Majority of the pupils, 139 (958.9%) had slight hearing impairment, 84 (35.6%) mild, 12 (5.1%) moderate and only 1 (0.4%) severe hearing impairment. One hundred and twenty-eight (54.1%) had unilateral hearing loss during 108 (45.9%) bilateral hearing loss [Table 7]. | Table 5: Prevalence of hearing impairment according to school proprietorship
Click here to view |
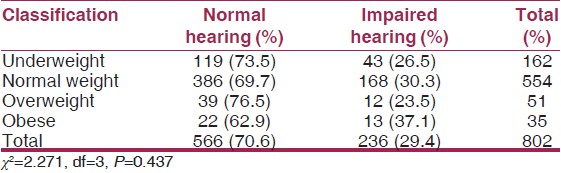 | Table 6: Prevalence of hearing impairment according to nutritional status
Click here to view |
Among the 802 pupils studied, 774 of them (96.5%) had their previous school year's result available. Six hundred and sixty-two pupils (82.5%) passed the school performance test while 112 (14.0%) failed. A higher proportion of pupils with hearing impairment failed the performance test (23.7%) than pupils with normal hearing (9.9%). The observed difference was statistically significant χ2 = 25.109, P = 0.000 [Table 8].{Table 8}
| Discussion | | |
This study showed a prevalence of 29.4% hearing loss among school pupils in PHC, Nigeria. This rate is slightly higher but comparable to a study in Egypt [20] which showed a prevalence of 25.6%. This might be due to the difference in the procedure adopted by the Egyptian study of allowing time for resolution of any transient middle ear infections in the children. A lower prevalence was however reported among pupils in Lagos, Nigeria [5] and in a Malaysian study [21] of 13.9% and 15% respectively. Hearing impairment from this study was most prevalent amongst older children (11-13 years) and least amongst those aged 5-7 years. These differences might be because routine screening that has never been done in these schools at the time the study was conducted led to missed opportunities for early detection and timely intervention. It might also not be unrelated to the school environment exposing children to prolonged loud noise as the schools were located on major roads in the city. Previous studies have documented the risk of developing hearing loss as a result of exposure to excessive noise over a prolonged time. [22],[23] The least hearing impairment prevalence was seen in this study amongst ages 5-7 years can be justified for the same reason of a weak health system and especially that of school health services in the country. [7],[8],[16] Children who are screened for hearing impairment before 14 months of age and received early intervention were found to function at the level of their peers by the time they entered school. [12] In the USA, school aged children are screened at first entry into school, every year from kindergarten through the 3 rd grade, 7 th grade, 11 th grade, entrance into special education, and upon grade repetition. [12] They are also screened upon entry into a new school system. Children who failed the screening tests are promptly referred to an Otorhinolaryngologist or Audiological physician for further assessment. This repeated screening done for children in developed countries can arguably be expensive in developing countries including Nigeria, however, such cultures started and maintained by the Government will go a long way into securing the future of the country and children are the fore front of such development. Early identification and treatment of children with hearing loss has been shown to improve prognosis/outcome. [7],[8] Medical (use of antibiotics and analgesics) and surgical (tympanostomy with ventilator-Gromet insertion and tympanoplasty) treatment remedies have been seen to be of benefit to such children. [24],[25],[26] Some other cases of hearing loss will require hearing aid fittings and speech therapy. Hearing aids can be used to amplify sound to make it clearer and more defined. In limited resource settings as Nigeria, it might be debated on the sustainability of providing hearing aid to hearing impaired children diagnosed on screening which might be a deterrent in promoting screening for hearing defects as screening cannot be conducted without treatment proffered to patients. Most families in Nigeria live below the poverty level [27] and as such if faced with a hearing impaired child cannot cope with the cost of acquiring a hearing aid for the child. As factual as it sounds though, routine school screening done for school children through a well-established school health programme, will diagnose these children and proffer other interventions that will be of profound help in the education of the child. This can include a simple administration of antibiotics to treat any infection that might have resulted in the impaired hearing loss which is transient or even a simple wax removal. As part of the intervention, the children can be given preferential seating positions in the class and started early to getting accustomed with sign language, lip reading and natural gestures. [7],[28] The children with severe hearing loss can also be referred early to special schools of the deaf assuming they cannot fit in the same school like normal children. In well-established school health programme, if such children are identified, there could be some help coming from international agencies and even government of wealthy countries who will assist in the treatment. [12],[26] This is readily not available in Nigeria.
This study showed various degrees of impairment; 58.9% had slight hearing impairment (16-25 Dbhl), 5.5% moderate to severe, and none was found to have profound hearing loss. This is similar to a study carried out in Lagos, Nigeria. [5] Coping with normal children is complex which might contribute as part of the reason no child with profound hearing loss was in this study. The children might also be kept at home by their parents since it would be difficult to pay for special schools or for fear of shame which will further increase the low education level in the country as well as affect the child's development. Hearing impairment in this study showed a unilateral loss of 54.1% and 45.9% bilateral hearing loss. This finding is important in any intervention that could be given to a child as the cause of unilateral hearing loss if transient could be relieved by simple medications or procedures to relieve the cause while a child with bilateral hearing loss can be on surveillance for early intervention. A study in Malaysia [22] reported similar findings.
Periodic screening for hearing loss or any other screening is important in any school as seen from the results of this study. The schools that participated in this study did not have any school health activity running and has left some pupils to go unidentified with varying degrees of hearing loss that has also affected their academic performance. The students identified with hearing loss were counselled with their parents and referred for further follow-up at the teaching hospital.
| Conclusion and recommendations | | |
This study, therefore, concludes that the prevalence of hearing loss among pupils in PHC, Rivers state, Nigeria is 29.4%. The study therefore suggests that routine screening be conducted in all schools in Nigeria.
| Study limitations | | |
This study was not without some limitations. The prevalence seen in this study might not be representative of the general population because some parents in these schools did not consent to the study. Since the study involved younger age group, it is also possible there could be bias in the measurement taken. Interpretation of school performance as relating to hearing loss should be taken with caution as other factors could confound the findings. Irrespective of these limitations, the findings from this study cannot be overlooked. Policy makers should be informed on the need to strengthen school health in Nigeria and encourage routine screening as part of schools activities.
| References | | |
| 1. | Karatas E, Kanlikama M, Mumbuc S. Auditory functions in children at schools for the deaf. J Natl Med Assoc 2006;98:204-10.  |
| 2. | Mathers C, Smith A, Cancher M. Global burden of hearing loss in the year 2000. Geneva: WHO; 2003. Available from: http://www.who.int/healthinfo/statistics/bod_hearingloss.pdf. [Last accessed on 2011 Aug 10] |
| 3. | Olusanya BO. Hearing impairment prevention in developing countries: Making things happen. Int J Pediatr Otorhinolaryngol 2000;55:167-71. |
| 4. | Taha AA, Pratt SR, Farahat TM, Abdel-Rasoul GM, Albtanony MA, Elrashiedy AL, et al. Prevalence and risk factors of hearing impairment among primary-school children in Shebin El-kom District, Egypt. Am J Audiol 2010;19:46-60. |
| 5. | Olusanya BO, Okolo AA, Ijaduola GT. The hearing profile of Nigerian school children. Int J Pediatr Otorhinolaryngol 2000;55:173-9. |
| 6. | American Speech-Language Hearing Association. Guidelines for the Audiological Assessment of Children from Birth to 5 Years of Age. Rockville; 2004. Available from: http://www.asha.org/policy/GL2004-00002.htm. [Last accessed on 2011 Aug 10] |
| 7. | Haddad J. Hearing loss. In: Behrman RE, Kliegman RM, Jenson BH, editors. Nelson Textbook of Paediatrics. 17 th ed. Philadelphia: W.B Saunders Company; 2004. p. 2129-35. |
| 8. | Ologe FE, Ernest SK. Screening audiometry in a private primary school in Ilorin. Niger J Paediatr 2002;29:96. |
| 9. | McPherson BD, Holborow CA. School screening for hearing loss in developing countries. Scand Audiol Suppl 1988;28:103-10. |
| 10. | Gell FM, White EM, Newell K, Mackenzie I, Smith A, Thompson S, et al. Practical screening priorities for hearing impairment among children in developing countries. Bull World Health Organ 1992;70:645-55. |
| 11. | Owolawi WD, Eleweke CJ. Benefits of early identification and intervention for hearing loss in children. The rationale for nationwide hearing screening programmes. J Natl Counc Except Child 2000;4:1-2. |
| 12. | New York State Department of Health. Assessment methods for young children with communication disorders. In: Clinical Practice Guidelines: Report of the Recommendations, Communication Disorders, Assessment and Intervention for Young Children. Ch. III. New York; 2006. p. 1-17. http://www.health.state.ny.us/community/infants_children/early_intervention/disorders/ch3_pt5.htm. [Last accessed on 2011 Aug 10] |
| 13. | Ojugo AI. Status of health appraisal services for primary school children in Edo state, Nigeria. Int Electron J Health Educ 2005;8:146-52. |
| 14. | Nwaimo IO. Status of health appraisal services in secondary schools in Owerri education zone, Imo state. J Health Kinesology 2001;2:94-107. |
| 15. | Ogbuji CN. School health services. In: Ezedum CE, editor. School Health Education. Nsukka: Topmost Press; 2003. p. 58-72. |
| 16. | Ofovwe GE, Ofili AN. Knowledge, attitude and practice of school health programme among head teachers of primary schools in Egor Local Government Area of Edo State, Nigeria. Ann Afr Med 2007;6:99-103. [ PUBMED]  |
| 17. | Office of the Permanent secretary, Rivers State Ministry of health. |
| 18. | Dennis JM, Neely JG. Basic hearing tests. Otolaryngol Clin North Am 1991;24:253-76. |
| 19. | SPSS Inc. SPSS Statistics for Windows, Version 17.0. Chicago: SPSS Inc.; 2008. |
| 20. | Mourad MI, Farghaly NF, Mohamed HG. Hearing impairment: Is it a public health problem among primary school pupils in Alexandria? J Egypt Public Health Assoc 1993;68:703-26. |
| 21. | Khairi Md Daud M, Noor RM, Rahman NA, Sidek DS, Mohamad A. The effect of mild hearing loss on academic performance in primary school children. Int J Pediatr Otorhinolaryngol 2010;74:67-70. |
| 22. | Harrison RV. Noise-induced hearing loss in children: A 'less than silent' environmental danger. Paediatr Child Health 2008;13:377-82. |
| 23. | Daniel E. Noise and hearing loss: A review. J Sch Health 2007;77:225-31. |
| 24. | Bamford J, Uus K, Davis A. Screening for hearing loss in childhood: Issues, evidence and current approaches in the UK. J Med Screen 2005;12:119-24. |
| 25. | Adams DA. Management of the hearing impaired child. In: Kerr AG, Adams DA, Micheal J, editors. Scott-Brown's Paediatric Otolaryngology. Cinnamond. 6 th ed., Vol. 6. 1997. p. 178-90. |
| 26. | National Institute on Deafness and other Communicative Disorders. Healthy Hearing 2010. [Last accessed on 2011 Aug 10] |
| 27. | National Population Commission (NPC) and ICF Macro. Nigeria Demographic and Health Survey, 2008: Key findings Calverton, Maryland, USA: NPC and ICF Macro; 2009. |
| 28. | Chan KH. Sensorineural hearing loss in children. Classification and evaluation. Otolaryngol Clin North Am 1994;27:473-86. |
[Table 1], [Table 2], [Table 3], [Table 4], [Table 5], [Table 6], [Table 7]
|









 Search Pubmed for
Search Pubmed for