|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 10
| Issue : 1 | Page : 16-19 |
|
Critically ill obstetric admissions into a tertiary hospital's intensive care unit
AA Fawole1, BO Bolaji2, OO Oyedepo2, AS Adeniran2
1 Department of Obstetrics and Gynaecology, University of Ilorin Teaching Hospital, University of Ilorin, Ilorin, Nigeria
2 Department of Anaesthesia, University of Ilorin Teaching Hospital, University of Ilorin, Ilorin, Nigeria
| Date of Web Publication | 4-Nov-2015 |
Correspondence Address:
Dr. A S Adeniran
Department of Obstetrics and Gynaecology, University of Ilorin, PMB 1515, Ilorin
Nigeria
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/9783-1230.169060

Background: Intensive Care Unit (ICU) management is a critical care and may be lifesaving in critically ill obstetric patients, but mortality remains high in low-resource countries. Objective: To review obstetric admissions into a tertiary hospital ICU. Design: Retrospective descriptive study. Setting: The ICU of the University of Ilorin Teaching Hospital, Ilorin, Nigeria. Subjects: Women admitted to the ICU during pregnancy or within 42 days of the end of the pregnancy. Materials and Methods: A list of all eligible participants was compiled, the case files were retrieved and relevant data extracted; the results were presented in tables and percentages. Results: Obstetric patients constituted 12.3% of the total ICU admissions and 0.84% of all deliveries with 45.6% mortality; the mean age was 29.2 ± 5.4 years (range 18–42 years), mean parity was 2.0 ± 1.5 (range 0–6), 15 (28.8%) had no formal education, 39 (75.0%) were of low social class, 22 (42.3%) had no antenatal care, 41 (78.9%) were admitted for obstetric reason, and postpartum hemorrhage was the most common indication for admission (19 [36.5%]). In all, 44 (84.6%) were admitted postpartum, 45 (86.5%) had organ dysfunction at ICU admission, 36 (69.2%) had mechanical ventilation while the most common drug administered were antibiotics. Conclusion: Obstetric patients are important intensive care users, but maternal mortality remains high among them in low-resource countries despite the care received. Keywords: Critically ill, intensive care unit, obstetric admissions
How to cite this article:
Fawole A A, Bolaji B O, Oyedepo O O, Adeniran A S. Critically ill obstetric admissions into a tertiary hospital's intensive care unit. J Med Investig Pract 2015;10:16-9 |
How to cite this URL:
Fawole A A, Bolaji B O, Oyedepo O O, Adeniran A S. Critically ill obstetric admissions into a tertiary hospital's intensive care unit. J Med Investig Pract [serial online] 2015 [cited 2018 Aug 17];10:16-9. Available from: http://www.jomip.org/text.asp?2015/10/1/16/169060 |
| Introduction | |  |
Management of critically ill obstetric patients is important in improving maternal health (MDG-5) by reducing maternal mortality from these illnesses. The profile of admission of critically ill obstetric patients has been shown to be similar worldwide;[1] however, there is a clear division in the mortality with rates of 0–9.4%[2],[3] from developed compared to 33–52% in low-resource countries.[4],[5],[6],[7] This wide gap is due to a combination of clinical and economic factors with illiteracy, poverty, lack of awareness about health complications, and social/behavioral factors [8] in low-resource countries while well-equipped labor wards, evidence-based practice, and effective insurance schemes have reduced mortality and improved outcome in developed countries. Available data from Nigeria and Kenya reported high mortality with obstetric hemorrhage, complications of severe preeclampsia/eclampsia, multiple organ failure, late presentation, and lack of antenatal care as major determinants of mortality among critically ill women.[4],[5],[6],[7]
It has, therefore, become necessary to gather data on the outcome of the critical care in low-resource countries to more clearly define the profile and identify areas for improvement; this was the aim of this review.
| Materials and Methods | | |
The study was a retrospective descriptive study of critically ill obstetric patients admitted to the Intensive Care Unit (ICU) of the University of Ilorin Teaching Hospital, Ilorin, Nigeria from January 2010 to June 2013. The ICU is a multispecialized four bedded unit with facilities for multimodal parameter monitoring and functioning mechanical ventilators. It receives patients from all medical and surgical units in the hospital as well as referrals from other centers within and outside the state.
The ICU admission register was reviewed, and a list of all eligible women was compiled; the case files were then retrieved from the medical records department of the hospital for analysis.
The inclusion criteria were admission to the ICU during pregnancy or within 42 days of its termination and availability of the case file for review. Exclusion criteria were nonobstetric patients and obstetric patients whose case files were not available for review.
The data obtained included sociodemographic and obstetric parameters, indication and clinical state at ICU admission, the interventions and final outcome of ICU admission. The results were expressed in tables with percentages.
The data for the study was part of the result of an audit of ICU care in the hospital during the study period; institutional ethical approval was obtained before commencement of the study, sponsorship was by the researchers, and there was no conflict of interest in the conduct of the study.
| Results | | |
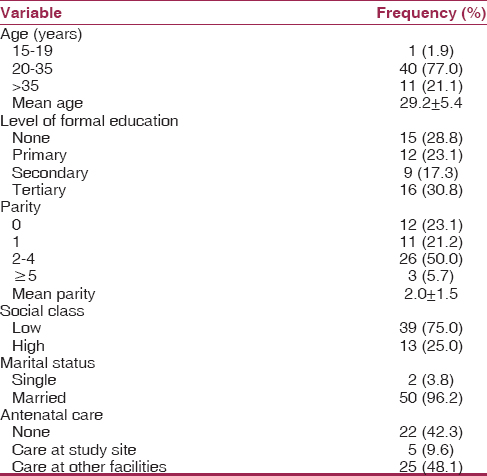
Of the 731 patients admitted to the ICU during the study period, 90 were critically ill obstetric patients constituting 12.3% of ICU admissions and 0.84% (8.4/1000) of total deliveries; there were 41 deaths with mortality of 45.6%. However, 52 case files (57.8% retrieval rate) were available for review and included in subsequent analysis. The mean age was 29.2 ± 5.4 years (range 18–42), mean parity was 2.0 ± 1.5 (range 0–6), 15 (28.8%) had no formal education, 39 (75%) were of low social class, and 22 (42.3%) had no antenatal care [Table 1].
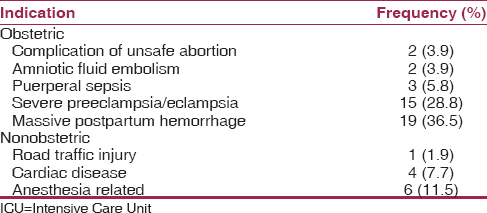
Obstetric indications were responsible for 41 (78.9%) while nonobstetric indications were in 11 (21.1). The two most common obstetric indications were massive postpartum hemorrhage in 19 (36.5%) and complications of severe preeclampsia/eclampsia in 15 (28.8%) while anesthesia related indications occurred in 6 (11.5%) and cardiac diseases in 4 (7.7%) of the women [Table 2].
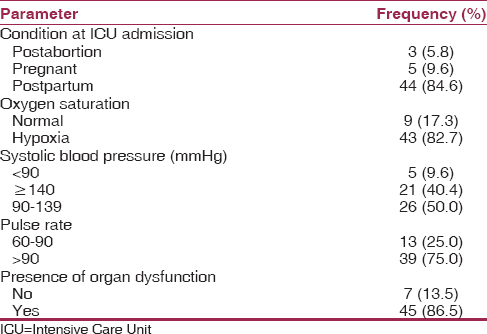
At admission into ICU, 44 (84.6%) were postpartum, 43 (82.7%) had hypoxia, 26 (50.0%) had hypertension, 39 (75.0%) had tachycardia, while 45 (86.5%) had organ dysfunction [Table 3]. Twenty women had (38.5%) vaginal delivery, 29 (55.7%) had abdominal delivery, while 3 (5.8%) were postabortion.
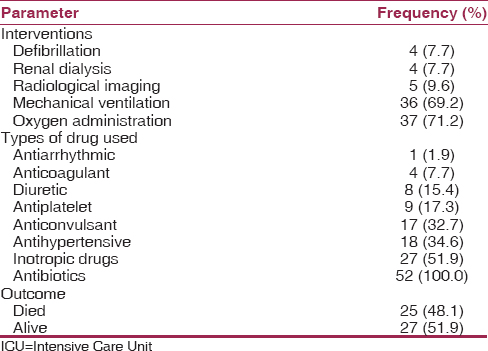
In [Table 4], the most common interventions at the ICU were oxygen administration in 37 (71.2%) and mechanical ventilation in 36 (69.2%), the most common medication used were antibiotics in all the women and inotropic drugs (27 [51.9%]).
| Discussion | | |
Critically ill obstetric patients constituted 12.3% of all ICU admissions in this study; this was higher than reports of 1.25–4.6% from low-resource [4],[5],[6],[9] and 0.38–10% in developed countries.[1],[2],[3],[7],[8],[10],[11],[12],[13],[14],[15],[16] This may be due to the higher frequency of obstetric ICU admission in this center which has the only ICU facility in two states and serves a large proportion of about four other neighboring states; thus suggesting a need for more centers. Critically ill obstetric patients constituted 0.84% of total deliveries; this compares favorably with 0.2–1.4% from low- resource [4],[6],[9] and 0.2–1.54% in developed [3],[7],[8],[10],[14],[15],[16] countries. This shows the similarity in the range of proportion of parturient requiring intensive care irrespective of the country despite the fewer facilities in low-resource countries.
The mean age was similar to reports from other researchers,[2],[6],[7],[9],[13] further emphasizing that these critically ill women were of reproductive age with 44.3% having one or no previous delivery similar to 45–66% by other authors.[6],[9],[15] This raises a concern for adequate intervention to salvage the life of these young women who are also productive members of the population.
There appears to be a relationship between nonantenatal clinic attendance and high mortality rate among critically ill obstetric patients. In this study, 42.3% had no antenatal care with 45.6% mortality compared to 50% nonantenatal care with 41.2% mortality in Ile-Ife, Nigeria [4] and 79.6% nonantenatal care with 52% mortality in Ibadan, Nigeria,[9] in contrast to 0% nonantenatal care and 0% mortality in Canada.[8] This implies that the higher the nonantenatal clinic attendance, the higher the mortality among critically ill obstetric patients.
In this study, most reports by other researchers in both low-resource and developed countries, the two most common obstetric indications for ICU admission in obstetric patients were massive postpartum hemorrhage and complications of preeclampsia/eclampsia.[3],[4],[5],[6],[9],[11],[12],[13],[16],[17] This calls for a higher level of anticipation, birth preparedness, and complication readiness to address postpartum hemorrhage with adequate prophylaxis for those at risk and prompt intervention when it occurs to prevent massive hemorrhage. In addition, preeclampsia remains a disease of theories; greater attention must be dedicated in unraveling the cause, and by extension of an effective prevention of this disorder of pregnancy.
The high rate of cesarean delivery in critically ill obstetric patients is related to the underlying pregnancy complications necessitating emergency delivery as well as complications of the procedure. Thus, the 55.7% rate in this study is similar to the reports of 64%,[18] 76%,[7] and 85%[9] by other researchers.
Previous researchers have reported that majority of critically ill obstetric patients who needed intensive care were in the postpartum period with a range of 63–100%[2],[3],[4],[5],[7],[13],[16] similar to 78.9% in this study. This emphasizes the role of active labor monitoring for all women by skilled birth attendants who can identify complications and institute appropriate treatment or referral promptly before significant morbidity occurs.
The use of mechanical ventilator was employed in the management of 69.2% of patients similar to the reports of 21–63%[5], 9, [16],[17],[18] from other authors. This emphasizes the severity of the illness in these obstetric patients at presentation, the need for adequate equipment for patient care, and the attendant poor outcome when these are not available.
Antibiotics, antihypertensive, anticonvulsant, and inotropic drugs were among the commonly used medications in this study similar to previous reports.[7],[8],[17] The antibiotics are important in preventing infection, the antihypertensive, and anticonvulsants, especially in the management of preeclampsia and eclampsia, while inotropic drugs are useful in cardiac complications.
Maternal mortality in this study was 45.6% similar to 41.2% from Ile-Ife,[4] 52% from Ibadan,[9] and 48% from Enugu [5] all in Nigeria and 33% from Kenya [6] in contrast to 0% mortality from Canada,[8] Australia,[2] and Saudi Arabia.[19] This shows that maternal mortality among critically ill obstetric patients in low-resource countries remains high despite the similarity in the pattern of the illnesses. An explanation may be the few ICUs in low-resource countries and the limited availability of equipment will be needed to appropriately treat the illnesses.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Pollock W, Rose L, Dennis CL. Pregnant and postpartum admissions to the intensive care unit: A systematic review. Intensive Care Med 2010;36:1465-74.  |
| 2. | Sriram S, Robertson MS. Critically ill obstetric patients in Australia: A retrospective audit of 8 years' experience in a tertiary intensive care unit. Crit Care Resusc 2008;10:124. |
| 3. | Al-Suleiman SA, Qutub HO, Rahman J, Rahman MS. Obstetric admissions to the intensive care unit: A 12-year review. Arch Gynecol Obstet 2006;274:4-8. |
| 4. | Faponle AF, Adenekan OT. Obstetric admissions into the intensive care unit in a sub-urban university teachng hospital. Nepal J Obstet Gynaecol 2011;6:33-6. |
| 5. | Okafor UV, Efetie ER, Amucheazi A. Risk factors for maternal deaths in unplanned obstetric admissions to the intensive care unit-lessons for sub-Saharan Africa. Afr J Reprod Health 2011;15:51-4. |
| 6. | Githae F, Mung'ayi V, Stones W. Course and outcome of obstetric patients admitted to a university hospital intensive care unit. East Afr Med J 2011;88:356-60. |
| 7. | Anwari JS, Butt AA, Al-Dar MA. Obstetric admissions to the intensive care unit. Saudi Med J 2004;25:1394-9. |
| 8. | Lapinsky SE, Kruczynski K, Seaward GR, Farine D, Grossman RF. Critical care management of the obstetric patient. Can J Anaesth 1997;44:325-9. |
| 9. | Osinaike B, Amanor-Boadu S, Sanusi A. Obstetric intensive care: A developing country experience. Internet J Anesthesiol 2005;10. |
| 10. | Madan I, Puri I, Jain NJ, Grotegut C, Nelson D, Dandolu V. Characteristics of obstetric intensive care unit admissions in New Jersey. J Matern Fetal Neonatal Med 2009;22:785-90. |
| 11. | Bandeira AR, Rezende CA, Reis ZS, Barbosa AR, Peret FJ, Cabral AC. Epidemiologic profile, survival, and maternal prognosis factors among women at an obstetric intensive care unit. Int J Gynaecol Obstet 2014;124:63-6. |
| 12. | Aldawood A. Clinical characteristics and outcomes of critically ill obstetric patients: A ten-year review. Ann Saudi Med 2011;31:518-22. [ PUBMED]  |
| 13. | Vasquez DN, Estenssoro E, Canales HS, Reina R, Saenz MG, Das Neves AV, et al. Clinical characteristics and outcomes of obstetric patients requiring ICU admission. Chest 2007;131:718-24. |
| 14. | Richa F, Karim N, Yazbeck P. Obstetric admissions to the intensive care unit: An eight-year review. J Med Liban 2008;56:215-9. |
| 15. | Rios FG, Risso-Vázquez A, Alvarez J, Vinzio M, Falbo P, Rondinelli N, et al. Clinical characteristics and outcomes of obstetric patients admitted to the intensive care unit. Int J Gynaecol Obstet 2012;119:136-40. |
| 16. | Ramachandra Bhat PB, Navada MH, Rao SV, Nagarathna G. Evaluation of obstetric admissions to intensive care unit of a tertiary referral center in coastal India. Indian J Crit Care Med 2013;17:34-7. |
| 17. | Quah TC, Chiu JW, Tan KH, Yeo SW, Tan HM. Obstetric admissions to the intensive therapy unit of a tertiary care institution. Ann Acad Med Singapore 2001;30:250-3. |
| 18. | Leung NY, Lau AC, Chan KK, Yan WW. Clinical characteristics and outcomes of obstetric patients admitted to the intensive care unit: A 10-year retrospective review. Hong Kong Med J 2010;16:18-25. |
| 19. | Al-Jabari AS, Al-Meshari AA, Takrouri MS, Seraj MA. Gynecology and obstetrical conditions requiring intensive care admission. Saudi Med J 2001;22:980-3 |
[Table 1], [Table 2], [Table 3], [Table 4]
|









 Search Pubmed for
Search Pubmed for