|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2013 | Volume
: 1
| Issue : 2 | Page : 45-51 |
|
Assessment of anteroposterior and transverse first premolar extraction changes using palatal rugae and comparative analysis with lateral cephalogram in Angle's Class I and II patients: An institutional retrospective study
Supriya Nambiar, Subraya Mogra, Surendra Shetty, Siddarth Shetty
Department of Orthodontics and Dentofacial Orthopedics, Manipal College of Dental Sciences, Mangalore, India
| Date of Web Publication | 7-Aug-2013 |
Correspondence Address:
Supriya Nambiar
Department of Orthodontics and Dentofacial Orthopedics, Manipal College of Dental Sciences, Mangalore - 575 001, Karnataka
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.116284

Introduction: The most common method of resolving substantial tooth size-arch length discrepancies (TSALD) is extraction of premolars followed by space closure that involves distal movement of anterior teeth, mesial movement of posterior teeth, or a combination of both. The palate is an important area to describe change during premolar extractions, especially the palatal rugae due to their supposed uniqueness and overall stability The aim of this study was to measure changes in the positions of the incisors and molars, relative to the palatal rugae, and the changes in arch width relative to the mid palatine raphe. Materials and Methods: It was a retrospective study of 90 treated cases, 30 cases each of three different types of malocclusion from the Department of Orthodontics, Manipal College of Dental Sciences, and Manipal University. Measurements from the dental study models were compared to the values obtained from the lateral cephalograms after digitizing with View box software. Arch width changes were also assessed. Conclusion: First premolar extraction spaces were used up approximately 50% by anterior retraction and buccal segment advancement, respectively. Retraction of teeth measured from the study models was comparable to that on the lateral cephalogram. So superimposition of progressive study models can be used to assess antero posterior tooth movements as with maxillary cephalometric superimpositions. Keywords: Dental models, palatal rugae, superimposition, tooth movements
How to cite this article:
Nambiar S, Mogra S, Shetty S, Shetty S. Assessment of anteroposterior and transverse first premolar extraction changes using palatal rugae and comparative analysis with lateral cephalogram in Angle's Class I and II patients: An institutional retrospective study. J Orthod Res 2013;1:45-51 |
How to cite this URL:
Nambiar S, Mogra S, Shetty S, Shetty S. Assessment of anteroposterior and transverse first premolar extraction changes using palatal rugae and comparative analysis with lateral cephalogram in Angle's Class I and II patients: An institutional retrospective study. J Orthod Res [serial online] 2013 [cited 2017 Apr 4];1:45-51. Available from: http://www.jorthodr.org/text.asp?2013/1/2/45/116284 |
| Introduction | |  |
Tooth size-arch length discrepancy (TSALD) is one of the most common problems encountered in orthodontic clinical practice. The methods of correction of this malocclusion are by the reduction of tooth material in the form of extractions of certain specified teeth, most commonly the premolars. Post extraction, the alignment of the teeth properly in the antero posterior position becomes an essential aspect of space closure, keeping in mind the anchorage requirements and the final position of the incisors and molars. Depending on the treatment objectives and anchorage requirements, this may involve distal movement of anterior teeth, mesial movement of posterior teeth, or a combination of both. Also, it is an undeniable fact that some of the extraction space will be lost during retraction of the anterior teeth because of the inadvertent mesial movement of the posterior teeth that form the anchorage unit.
Since its inception, cephalometrics, have advanced and is used widely in orthodontic practice and research institutions. Cephalometric superimpositions are the only reliable method to determine whether orthodontic space closure has been performed according to planned anchorage requirements. Assessment of the post extraction anterior teeth retraction can be done by superimposing the pre and post treatment cephalograms. Some disadvantages of cephalometric radiographs like technique sensitivity, overlap of bilateral structures make it imperative occasionally to combine data derived from both cephalometric analysis and measurements on the dental models for the study of orthodontic treatment changes. Also, due to inherent errors in cephalometric radiographs, it becomes imperative to combine data derived from both cephalometric analysis and measurements on dental models for treatment assessment. The alternative method of assessment of dental changes involves the use of dental study models. Plaster models have been used for orthodontic records for many decades. Dental models provide a three dimensional view and their superimposition helps in appreciating longitudinal dento alveolar changes. The superimposition of dental casts might be a useful method to study longitudinal dentoalveolar changes related to dentofacial growth or orthodontic therapy as it provides a distinct picture of structural changes that occurs during the process. [1] However, superimposition of dental casts requires stable reference points on the surface of the model.
An area in which it is important to describe change during premolar extractions is the palate, especially the palatal rugae. Palatal rugae, also called plicae palatinae transversae or Rugae palatinae, refer to the ridges on the anterior part of the palatal mucosa. It is seen on either side of the median palatal raphe, behind the incisive papilla and are widely present in mammals. Rugae patterns have been studied for various purposes, published reports being mainly in the fields of Anthropology, Comparative Anatomy, Genetics, Forensic Odontology, Prosthodontics, and Orthodontics.
Palatine rugae are irregular, asymmetric ridges of mucous membrane extending laterally from the incisive papilla and the anterior part of the median palatal raphe. There are approximately four rugae on each side of the palate. Slightly more rugae are found in males and on the left side in both genders. Generally, there is no bilateral asymmetry in the number of primary rugae or in their angulation from the midline. The first (anterior) ruga contacts the median palatal raphe, while the rest have their origins lateral to it. Along with the teeth and tongue, rugae take part in mastication by helping to sense, hold and mash the food. Although important changes were observed in their lateral edges after orthodontic treatment with premolar extractions, the median edges of the rugae are considered to be stable and the supposed uniqueness and overall stability of palatal rugae suggest their use as a stable landmark for assessment of degree of tooth movement during treatment. [2],[3],[4]
Therefore, the aim of this study was to measure changes in the positions of incisors and molars relative to the palatal rugae on the dental study models and compares it with the anteroposterior tooth movements elicited from the lateral cephalogram in response to orthodontic treatment. Another objective was to define the amount of the extraction space that was used to retract the anterior teeth and reduce overjet and compare it to the amount of space taken up by buccal segment advancement. The changes in position of the central incisor and permanent first molar relative to the medial point of third palatal rugae as a stable reference point show how the space was used in resolving the malocclusion. The objective was also to evaluate the reliability and validity of using palatal rugae as a stable landmark for the assessment of anteroposterior tooth movements. Another important objective was also to measure changes in arch width relative to mid palatine raphe following first bicuspid extraction space closure.
| Materials and Methods | | |
This was a retrospective investigation in which patient records were observed at two different times. The sample consisted of 90 treated cases from the Department of Orthodontics, Manipal College of Dental Sciences, Manipal University. These included 30 cases each of three different types of malocclusion. They are Angle's class I bimaxillary protrusion malocclusion, Angle's class I crowding malocclusion, and Angle's class II division 1 malocclusion. The age at the time of initial records ranged from 14 years to 30 years.
In the present study the following inclusion criteria were considered:
- Cases which underwent maxillary 1 st premolar extraction as part of orthodontic treatment and with complete case records.
Exclusion criteria:
- Poor quality of radiographs.
- Patients who underwent palatal expansion or orthognathic surgery.
- Extractions done for other reasons before the start of orthodontic treatment.
Records consisted of pre-treatment and post-treatment maxillary study casts and lateral cephalometric radiographs for each subject where landmarks were identified. Each study model pretreatment and posttreatment was photographed with a Olympus SP-510UZ 7.1 Mega pixels,10x zoom (Olympus Corporation, Japan) digital camera in the macromode for reducing any vertical distance errors. The macromode of the camera settings helps to standardize the object - camera distance. The pictures of the dental casts were then digitized by using the View box software version 3.1.13, dhal software, Greece, to assess the magnification factor and to eliminate errors arising due to measurement. The images of the models that were saved and loaded on View box VERSION 3.1.13, a freeware had an overall magnification error of 0 to 5% which was corrected by the same software. Moreover, it was less than 7% magnification of the cephalograms that were used in this study and less than 10% magnification error that was associated with many photocopiers or scanners.
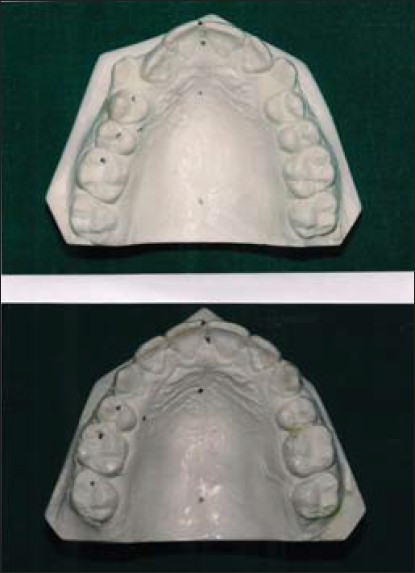
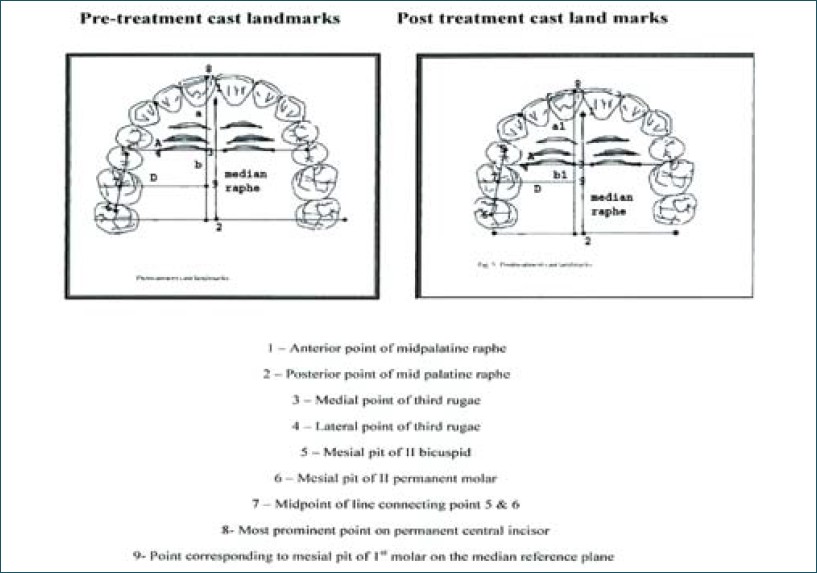
The following landmarks were marked on the cast as shown in [Figure 1], [Figure 2], [Figure 3].
- Rugae were numbered from first to third, with the first being most anterior.
- A median reference line was created by joining the incisive papilla anteriorly and fovea palatinae posteriorly.
- Lines were created medial point of the corresponding ruga on right side and through the incisal edge of right central incisor.
- A line was created perpendicular to the median line through the incisal midpoint.
- Two lines each perpendicular to the median reference line through the mesial pit of 2 nd premolar and mesial pit of first molar the following treatment.
- Movement of central incisor was measured relative to the right rugal point.
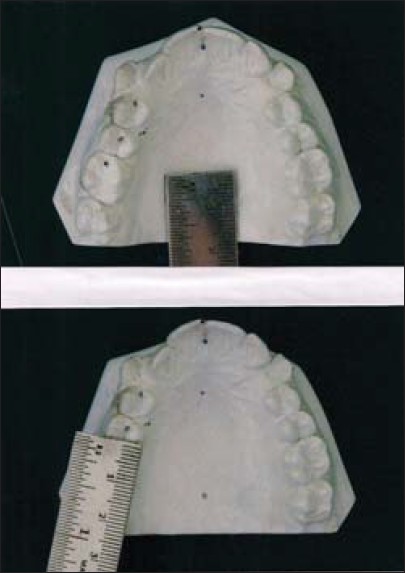
- To eliminate magnification errors arising due to measurements of structures at different vertical levels (such as incisal edges and medial ruga points), two subsequent photographs of each study model with a millimeter ruler at the occlusal level and the level of palatal vault at the 3 rd rugae were loaded into the software to calculate the error to get non erroneous results [Figure 2].
Standard reference planes:
A - Line drawn perpendicular to mid palatine raphe through the medial point of third rugae on the side which is more reliable [Figure 3].
D - Line drawn perpendicular to mid palatine raphe through the mesial pit of permanent 1st molar [Figure 3].
Linear measurements considered:
a and a 1 -Medial point of third rugae to incisal edge of central incisor in pre- and post-treatment casts, respectively [Figure 3].
b and b 1 - Medial point of third rugae to the line D in pre- and post-treatment casts, respectively [Figure 3].
Computer software View box version 3.1.13 - used to measure the following variables:
- Maxillary incisor and maxillary first molar positions relative to medial point of third ruga on the right side, namely pre-treatment (a) and post-treatment casts (a 1 ) for incisors position and pre-treatment (b) and post-treatment casts (b 1 ) for molar position.
- Incisor and maxillary first molar movement was measured by subtracting the post-treatment position from the pre-treatment position relative to the third ruga medial point, namely (a-a 1 ) and (b - b 1 ) for incisors and molars, respectively.
Procedures undertaken on the Lateral Cephalometric radiograph:
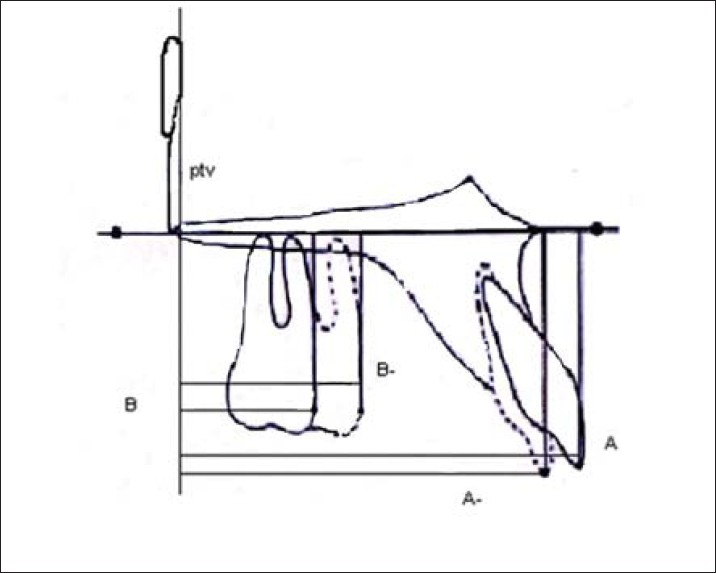
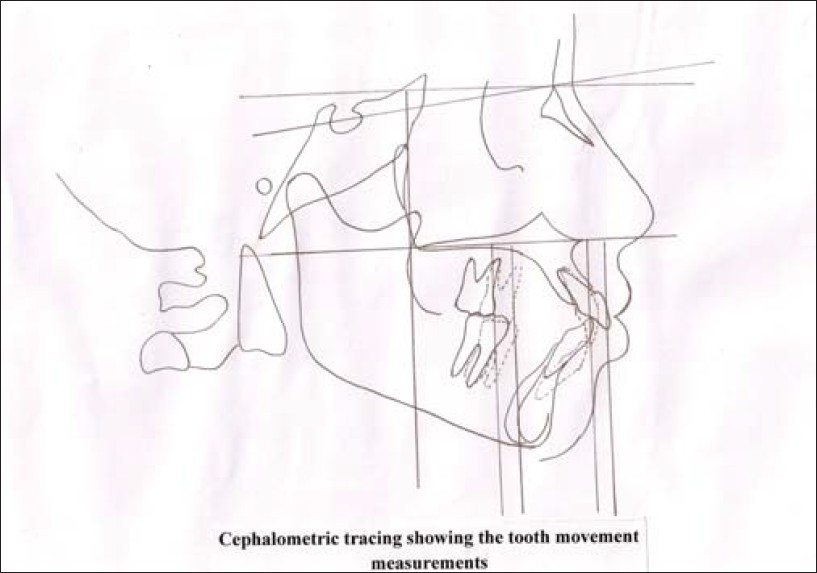
Standardized procedures were used at every stage to avoid errors in radiography or tracing. The tracings included floor of orbit, hard palate, anterior and posterior images of zygomatic process of maxilla, and pterygo maxillary fissure. The maxillary central incisor and maxillary first permanent molar were traced after the pretreatment and posttreatment tracings were superimposed [Figure 4].
Standard reference planes:
- Pterygoid vertical
- Palatal plane
- True horizontal drawn 7 0 to the Sella - Nasion plane
Landmarks considered: [Figure 5]
A and A 1 - Point at which a perpendicular line from palatal plane contacts the incisal edge pretreatment and after orthodontic space closure, respectively.
B and B 1 - Point at which a perpendicular line from palatal plane contacts the most prominent point of mesial surface of molars pretreatment and after orthodontic space closure, respectively.
Linear measurements considered:
A to PTV - Upper incisor to pterygoid vertical (Pretreatment)
A 1 to PTV - Upper incisor to pterygoid vertical (Post treatment)
B to PTV -Upper molar to pterygoid vertical (Pre treatment)
B 1 to PTV - Upper molar to pterygoid vertical (Post treatment)
The variables measured on the cephalometric radiographs:
- Maxillary incisor and maxillary first molar position relative to pterygoid vertical on pretreatment (aptv) and post-treatment radiographs (a 1 ptv) for incisors and on pretreatment (bptv) and post-treatment casts (b 1 ptv for 1 st molar.
- Incisor and maxillary first molar movement measured by subtracting post-treatment position from pretreatment position relative to third ruga medial point (aptv-a 1 ptv) for incisors and (bptv - b 1 ptv) for 1 st molar.
For analytical purposes, data for male and female were combined and the paired t-test found no statistical significance for measurements on right and left sides. Also the same tests were performed to assess whether a significant difference existed between cast and cephalometric variables along with the correlation test to assess the degree of correlation between cast and cephalometric variables for incisor and molar movement. Line E was used to assess the change in the arch width following extraction space closure.
| Results | | |
During space closure the measurements from the study models showed that the mean incisor movement was 5.87 SD 2.4 mm whereas the mean molar movement observed was 5.04 SD 1.42 mm. The respective measurements obtained from the lateral cephalogram superimposition showed a mean incisor movement of 5.80 SD 2.24 mm and the mean molar movement was 5 SD 1.45 mm [Table 1]. These values give us a picture that first premolar extraction spaces are used up roughly half and half by retraction and buccal segment advancement, respectively, and the measurements obtained from the study models are almost similar to measurements from the lateral cephalogram.
There was more of anterior retraction occurring in the class II division 1 sample in the present study compared to that observed in the class I crowding and bimaxillary protrusion sample [Table 1]. The amount of retraction in the class II division 1 sample ranged about 8 mm in the models and 7.77 mm in the radiograph, in Cl I Bimaxillary protrusion it ranged from 5.33 mm in models and 5.35 mm in radiograph and in Cl I Crowding it ranged around 4.27 mm for both. The amount of anchor loss was found to be higher in Cl I Crowding samples. In the class II division 1 sample ranged about 4.25 mm in the models and 3.89 mm in the radiograph, in Cl I Bimaxillary protrusion it ranged from 5.36 mm in models and 5.42 mm in radiograph and in Cl I Crowding it ranged around 5.52 mm for models and 5.70 mm for the radiograph. The following [Table 1], [Table 2], [Table 3], [Table 4], [Table 5] and [Figure 6], [Figure 7], [Figure 8], [Figure 9] depict the results of this study. | Table 3: One way anova test to compare tooth movements and arch width in study models and cephalograms among class of malocclusions
Click here to view |
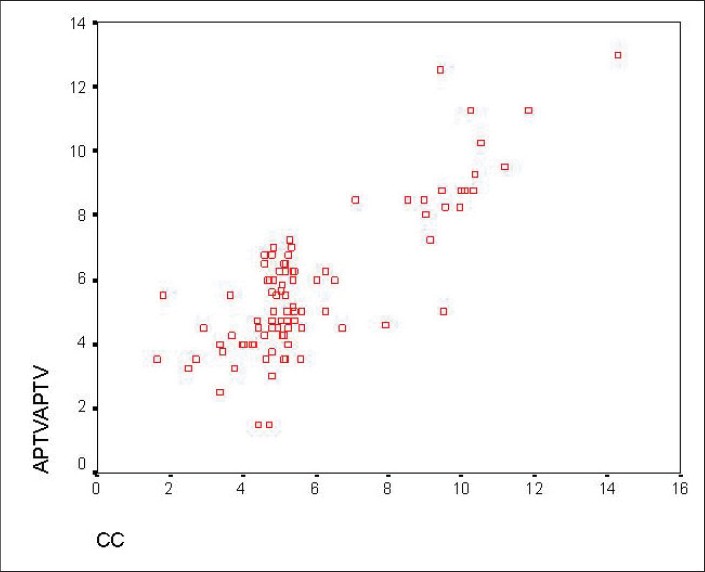 | Figure 7: Scatter plot indicating correlation in incisor tooth movements between cast and cephalometric measurements
Click here to view |
 | Figure 8: Scatter plot indicating correlation in the molar tooth movements between cast and cephalometric measurements
Click here to view |
| Discussion | | |
The magnitude of tooth movements surrounding first premolar extraction sites were used in the present study to determine how the space gained by extraction of four first premolars is used by the orthodontist in resolving patient's malocclusions. Characteristics like anterior or posterior crowding, Class II molar and canine relationships, facial height factors, habits, can all be factors involved in making this decision. [5] The present study depicts how the space created by 1st premolar extraction sites is used to resolve the various malocclusions in an antero posterior direction using palatal rugae as a stable landmark to assess tooth movement.
Studies by Bailey et al., Peavey et al., and Van Der Linden et al., [2],[3],[4] had evaluated the stability of medial ends of 3rd rugae as a stable landmark to assess these changes and the changes between rugae. However, relationships of rugae to tooth movements had not been assessed and this has been done in this study. Results of this study shows that the mean incisor and molar movements measured on the casts with the medial end of 3rd palatal rugae as the stable reference landmark and on the cephalograms are almost similar. From this study we can also conclude that the extraction spaces are used up roughly half for anterior retraction and posterior segment protraction, respectively, in different malocclusions [Table 1] and [Table 2], [Figure 6]. Also the measurements obtained from the study models are almost similar to measurements from the lateral cephalogram.
Literature evidence have shown that the percentage of space closed by retraction and posterior protraction do differ from case to case. Bar-ziony et al.[6] and Issacson et al.[7] have generally shown more maxillary anterior retraction which is similar to the results that were observed in this study since all of these studies included Class II patients in their samples and not just Class I patients and so more space had to be utilized in them for anterior retraction in order to correct them.
The space requirement for retraction was greater for Class II division 1 followed by class I bimaxillary protrusion and class I crowding. Hoggan and Sadowsky [8] concluded that medial ends of third palatal rugae could be used for assessment of anteroposterior tooth movements. But, it was crucial that current investigation could validate whether medial points of third rugae could be reliably used to assess tooth movements. The findings of present investigation support the use of these landmarks for that purpose.
The present study assessed the correlation between the different tooth movements in the study models and cephalogram [Table 3], [Figure 7] and [Figure 8]. A two-tailed Pearson correlation analysis revealed a correlation between the incisor tooth movements which was significant at 0.01 level [Table 4]. A similar test was performed for the molar tooth movements which were again significant at 0.01 level [Table 5].
The present study also found that for both incisor and molar tooth movements, values were significant substantiating the previous studies. [2],[7],[8],[9],[10] In fact, a larger study sample helped to make the results more reliable. Also, during the study magnification errors were corrected and all landmarks were easily visualized and measured.
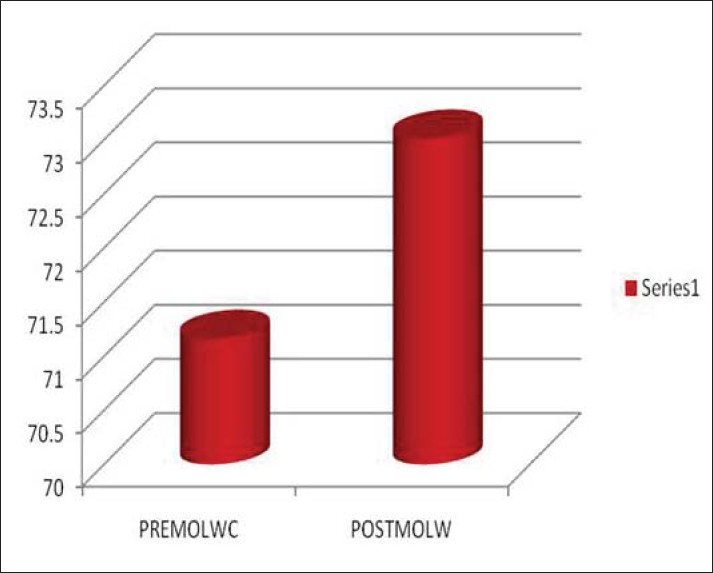
The mean increase in transverse width in molar area ranged from 1.85 mm, which was statistically significant [Table 4] and [Table 5], [Figure 9], whereas it was observed that the change in the transverse dimension in the premolar area was very minor and showed only slight constriction primarily because they had moved mesially to contact the canines that did not change systematically in their transverse positions. These findings did not seem to support the "collapse theory" that suggests that premolar extractions cause a constriction of the arches but rather seems to support the "expansion theory" that purports that canines are retracted into the broader arch diameter where the premolars had been located, except for the fact that it would finally depend on the type of malocclusion. [11],[12]
Limitations of this study are that the various types of malocclusions had been combined and compared and as a result there was no way to calculate the amount of transverse change which was needed in the first place for that particular group of malocclusions. However, the method used here is very simplistic and reliable. This technique is not particularly time consuming and does not require any particular expertise.
| Conclusions | | |
- First premolar extraction spaces were used up equally 50% by anterior retraction and buccal segment advancement, respectively.
- The medial end of 3 rd rugae was found to be a stable landmark to assess tooth movement changes in an anteroposterior direction during extraction space closure.
- Measurements obtained from the study models were almost similar to measurements from the lateral cephalogram for teeth movement and so superimposition of progressive study models can be used to assess anteroposterior tooth movements as with maxillary cephalometric superimpositions, thereby providing us with an alternative.
- Anterior retraction is maximum in class II div 1, followed by class I bimaxillary protrusion and class I crowding.
- The overall increase in molar width in the total sample was highly statistically significant but the increase in molar width between the different types of malocclusion and age groups were not significant.
| References | | |
| 1. | Lebret L. Physiologic tooth migration. J Dent Res 1964;43:610-8. 
|
| 2. | Bailey LJ, Esmailnejad A, Almeida MA. Stability of the palatal rugae as landmarks for analysis of dental casts. Angle Orthod 1996;66:73-8.
|
| 3. | Peavy DC, Kendrick GS. The effects of tooth movement on the palatine rugae. J Prosthet Dent 1967;18:536-42.
|
| 4. | Van der Linden FP. Changes in the position of posterior teeth in relation to ruga points. Am J Orthod 1978;74:142-61.
|
| 5. | Thiruvenkatachari B, Al-Abdallah M, Akram NC, Sandler J, O'Brien K. Measuring 3-dimensional tooth movement with a 3-dimensional surface laser scanner. Am J Orthod Dentofacial Orthop 2009;135:480-5.
|
| 6. | Bar-ziony, Ferrer D, Johnson PD, Gibbs CH, Taylor M, McGorray SP, et al. New method to reproducibly examine and quantify spatial orientation of teeth with relation to a fixed structure on orthodontic study models. J Dent Res 1997;77:12-580.
|
| 7. | Isaacson R, Worms FW, Speidel TM. Measurement of tooth movement. Am J Orthod 1976,70:290-303.
|
| 8. | Hoggan BR, Sadowsky C. The use of palatal rugae for the assessment of anteroposterior tooth movements. Am J Orthod 2001;119:482-8.
|
| 9. | Almeida MA, Phillips C, Kula K, Tulloch C. Stability of palatal rugae as landmarks for analysis of dental casts. Angle Orthod 1995;65:43-8.
|
| 10. | Cha BK, Lee JY, Jost-Brinkmann PG, Yoshida N. Analysis of tooth movement in extraction cases using three-dimensional reverse engineering technology. Eur J Orthod 2007;29;325-31.
|
| 11. | Gianelly AA. Arch width after extraction and nonextraction treatment. Am J Orthod Dentofacial Orthop 2003;123:25-8.
|
| 12. | Taner TU, Ciger S, El H, Germeç D, Es A. Evaluation of dental arch width and form changes after orthodontic treatment and retention with a new computerized method. Am J Orthod Dentofacial Orthop 2004;126:464-76.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7], [Figure 8], [Figure 9]
[Table 1], [Table 2], [Table 3], [Table 4], [Table 5]
|










 Search Pubmed for
Search Pubmed for