|
 
 |
| CASE REPORT |
|
| Year : 2014 | Volume
: 2
| Issue : 1 | Page : 38-41 |
|
Interception of a developing Class III malocclusion with facemask therapy
Prathapan Parayaruthottam1, Vincy Antony2, PG Francis2, KM Muhamed Shaloob2, K Jubin Hassan2
1 Department of Orthodontics, Government Dental College, Kozhikode, India
2 Department of Orthodontics and Dentofacial Orthopedics, MES Dental College, Perinthalmanna, Kerala, India
| Date of Web Publication | 29-Jan-2014 |
Correspondence Address:
Prathapan Parayaruthottam
Department of Orthodontics, Government Dental College, Kozhikode, Kerala
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.125925

Developing skeletal Class III malocclusion is one of the most challenging problems for the practicing orthodontists. Whether to start early treatment or wait for growth to be over is an ongoing debate. Interception of mild to moderate cases should be carried out as early as possible before it becomes severe. The protraction facemask has been widely used in the interception of developing Class III malocclusion with maxillary deficiencies. We present a patient with a developing skeletal Class III malocclusion with maxillary deficiency for whom a protraction facemask was given and there was successful interception of the skeletal malocclusion. Keywords: Class III malocclusion, maxillary deficiency, protraction facemask
How to cite this article:
Parayaruthottam P, Antony V, Francis P G, Muhamed Shaloob K M, Hassan K J. Interception of a developing Class III malocclusion with facemask therapy. J Orthod Res 2014;2:38-41 |
How to cite this URL:
Parayaruthottam P, Antony V, Francis P G, Muhamed Shaloob K M, Hassan K J. Interception of a developing Class III malocclusion with facemask therapy. J Orthod Res [serial online] 2014 [cited 2018 Mar 30];2:38-41. Available from: http://www.jorthodr.org/text.asp?2014/2/1/38/125925 |
| Introduction | |  |
Skeletal Class III malocclusion can be manifested as maxillary deficiency, mandibular prognathism or a combination of both. "To or not to" intervene is a common dilemma faced by orthodontists and pediatric dentists when confronted with a developing Class III malocclusion. The etiology of Class III malocclusion is believed to be mainly hereditary, but environmental factors such as habits and mouth breathing may also play a role. [1],[2] The prevalence of Class III malocclusion varies among different ethnic groups. The incidence in Caucasians ranges between 1% and 4%. [3] The frequency of Class III malocclusions is higher in Asians (4-14%) due to a large percentage of patients with maxillary deficiency. [4]
In Class III malocclusions, the discrepancy between the maxilla and the mandible is expressed in many ways. According to Guyer et al., 57% of Class III patients with either a normal or prognathic mandible showed a deficiency in the maxilla. [5] From this, it can be deduced that the frequency of appearance of maxillary deficiency is more than mandibular prognathism in such cases. Protraction facemask therapy has been advocated in the treatment of Class III patients with maxillary deficiency. [6],[7]
| Case Report | | |
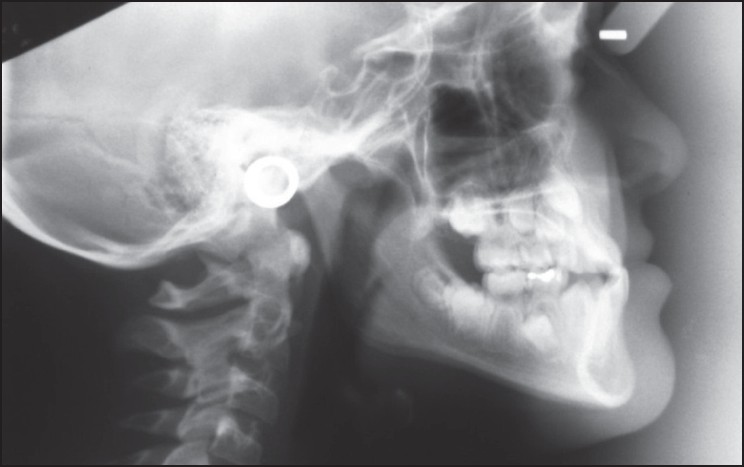
This was a case report of a 9-year-old girl patient who was admitted to the clinic with the complaint of her lower jaw being in front. The pre-treatment records showed that the patient had normal vertical proportions, a straight profile and good facial symmetry [Figure 1]. The cephalometric evaluation confirmed a Class III skeletal relationship with maxillary deficiency [Figure 2]. Intraorally there was reverse over jet [Figure 3].
Treatment Objectives
Early Class III treatment creates an environment in which more favorable dentofacial growth can occur. Treatment objectives include: [8]
- Prevention of progressive irreversible soft tissue or bony changes - Class III malocclusion is often accompanied with an anterior crossbite. Uncorrected anterior crossbite may lead to abnormal wear of the lower incisors and dental compensation of mandibular incisors. This leads to thinning of the labial alveolar plate and/or gingival recession. [9]
- Improvement of skeletal discrepancie - Early orthopedic treatment using facemask or chin cup therapy improves the skeletal relationship, which in turn minimizes excessive dental compensation such as overclosure of the mandible and retroclination of the mandibular incisors.
- Improvement of occlusal function - Class III malocclusion with an anterior crossbite is often accompanied by a functional shift. Early orthopedic treatment may help in eliminating centric occlusion/centric relation (CO/CR) discrepancies and avoid adverse growth.
- Reducing the complexity of phase II comprehensive treatment - In mild and moderate Class III patients, early orthodontic or orthopedic treatment may eliminate the necessity for orthognathic surgery treatment. Early correction of the transverse dimension and maximizing the growth potential of the maxilla may minimize the extent of the surgical procedures.
- Pleasing facial esthetics can be achieved - Thus improving the psychosocial development of the child. [10]
Treatment Progress
Treatment was started with a Petit type facemask, which was used along with a maxillary expansion appliance with hooks, to engage elastics [Figure 4]. Intraorally, a bonded expansion appliance was cemented. Though, the patient did not have a constricted upper arch, the orthopedic expansion appliance was activated to disarticulate the maxilla from the circum-maxillary sutures.
Treatment Results
After 6 months of treatment, the anterior crossbite was corrected [Figure 5]. Analysis of the cephalometric radiograph [Figure 6] and photograph [Figure 7] revealed a marked improvement in her profile with a slight fullness in the maxillary anterior region.
| Discussion | | |
The protraction facemask has been used in the treatment of patients with Class III malocclusion and a maxillary deficiency. The facemask has an adjustable anterior wire that can accommodate a downward and forward pull on the maxilla with elastics. To minimize the tipping of the palatal plane, the protraction elastics are attached near the maxillary canines with a downward and forward pull of 30° to the occlusal plane. [9] Maxillary protraction usually requires 300-600 g of force per side, depending on the age of the patient. Patients are instructed to wear the appliance for 12 hours/day. Correction using facemask along with palatal expansion occurs by a combination of skeletal and dental changes in both sagittal and vertical dimensions. These changes occur as a result of forward movement of the maxilla, backward and downward rotation of the mandible and proclination of the maxillary incisors.
To protract the maxilla effectively, the force should be applied to the maxilla as a unit. Usually a bonded or banded rapid maxillary expansion appliance is placed. Activation of the rapid maxillary expansion appliance not only provides orthopedic expansion of the maxilla, but also helps to "disarticulate" the maxilla at the circum-maxillary sutures. Such a "disarticulated" maxilla would respond better to the anteriorly directed orthopedic forces exerted by the facemask. Therefore, activation of the rapid maxillary expansion appliance is indicated even if there is no transverse discrepancy to begin with.
Depending on the severity of the malocclusion, anterior crossbite can be corrected from 3 to 4 months of maxillary expansion and protraction with facemask. Improvement in overbite and molar relationship can be expected with an additional 4-6 months of treatment.
| Conclusion | | |
Orthopedic facemask is the appliance of choice in cases with maxillary deficiency and produces dramatic results in the shortest period of time. Early treatment of Class III patients with maxillary deficiency using appliances such as the protraction facemask can be used to eliminate anterior crossbite, CO/CR discrepancy and maximize the growth potential of the nasomaxillary complex. Earlier diagnosis and faster treatment would help to achieve a faster and more stable result. The key to successful management of such cases, therefore, is to remove the anterior crossbite as early as possible so as to allow for the normal unrestricted growth of the maxilla and also to guide the mandible to a normal position.
| Acknowledgment | | |
The Author would like to thank the patient for providing consent to use her photograph in this article.
| References | | |
| 1. | Litton SF, Ackermann LV, Isaacson RJ, Shapiro BL. A genetic study of Class 3 malocclusion. Am J Orthod 1970;58:565-77. 
[PUBMED] |
| 2. | Rakosi T, Schilli W. Class III anomalies: A coordinated approach to skeletal, dental, and soft tissue problems. J Oral Surg 1981;39:860-70.
[PUBMED] |
| 3. | Newman GV. Prevalence of malocclusion in children six to fourteen years of age and treatment in preventable cases. J Am Dent Assoc 1956;52:566-75.
[PUBMED] |
| 4. | Ishii H, Morita S, Takeuchi Y, Nakamura S. Treatment effect of combined maxillary protraction and chincap appliance in severe skeletal Class III cases. Am J Orthod Dentofacial Orthop 1987;92:304-12.
[PUBMED] |
| 5. | Guyer EC, Ellis EE 3 rd , McNamara JA Jr, Behrents RG. Components of class III malocclusion in juveniles and adolescents. Angle Orthod 1986;56:7-30.
|
| 6. | Turley PK. Orthopedic correction of Class III malocclusion with palatal expansion and custom protraction headgear. J Clin Orthod 1988;22:314-25.
[PUBMED] |
| 7. | McNamara JA Jr. An orthopedic approach to the treatment of Class III malocclusion in young patients. J Clin Orthod 1987;21:598-608.
[PUBMED] |
| 8. | Joondeph DR. Early orthodontic treatment. Am J Orthod Dentofacial Orthop 1993;104:199-200.
[PUBMED] |
| 9. | Ngan P. Treatment of Class III malocclusion in the primary and mixed dentitions. In: Bishara SE, editor. Textbook of Orthodontics. Philadelphia: WB Saunders; 2001. p. 375-411.
|
| 10. | Ngan P, Hägg U, Yiu C, Merwin D, Wei SH. Soft tissue and dentoskeletal profile changes associated with maxillary expansion and protraction headgear treatment. Am J Orthod Dentofacial Orthop 1996;109:38-49.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7]
|
















 Search Pubmed for
Search Pubmed for