|
 
 |
| CASE REPORT |
|
| Year : 2014 | Volume
: 2
| Issue : 1 | Page : 42-45 |
|
Orthodontic extraction of a mandibular third molar to avoid nerve injury: A case report
Enver Yetkiner1, Ersin Mutlu1, Gulcan Coskun Akar2
1 Department of Orthodontics, Faculty of Dentistry, Atatürk Medical Technology Vocational Training School, University of Ege, Izmir, Turkey
2 Associate Professor, Faculty of Dentistry, Atatürk Medical Technology Vocational Training School, University of Ege, Izmir, Turkey
| Date of Web Publication | 29-Jan-2014 |
Correspondence Address:
Enver Yetkiner
Department of Orthodontics, Faculty of Dentistry, University of Ege, Bornova, Izmir
Turkey
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.125927

Surgical removal of impacted mandibular third molars is a common procedure with the potential of causing side-effects such as inferior alveolar nerve (IAN) injury and damaging of adjacent tissues. Orthodontic extrusion of such molars is an alternative treatment modality that reduces unwelcome risks. This case report presents the orthodontic extrusion and consequent surgical extraction of an impacted mandibular third molar intersecting the IAN canal and the 6-month follow-up status. A 41-year-old female with facial pain on the left side as the main complaint was diagnosed with a severely impacted mandibular third molar that required extraction. Radiographic evaluation revealed the critical proximity of the tooth to the IAN. The impacted third molar was surgically exposed and closed orthodontic extrusion protocol with light forces was administered. The third molar was surgically extracted following a 9-month traction period and bone healing was monitored for 6 months. The facial pain reduced gradually following the extrusion of the impacted molar. No neurological complications were observed immediately after and during the long-term follow-up the surgical extraction. Clinically and radiographically, significant healing distal to the second molar was obtained at the end of follow-up period. Orthodontic
extrusion and surgical extraction of severely impacted third molars may be an alternative treatment modality that facilitates easier surgical procedures with lower neurological risks. Keywords: Extraction, facial pain, impacted molar, IAN, inferior alveolar nerve, paresthesia
How to cite this article:
Yetkiner E, Mutlu E, Akar GC. Orthodontic extraction of a mandibular third molar to avoid nerve injury: A case report. J Orthod Res 2014;2:42-5 |
How to cite this URL:
Yetkiner E, Mutlu E, Akar GC. Orthodontic extraction of a mandibular third molar to avoid nerve injury: A case report. J Orthod Res [serial online] 2014 [cited 2018 Apr 2];2:42-5. Available from: http://www.jorthodr.org/text.asp?2014/2/1/42/125927 |
| Introduction | |  |
Pain and swelling are the two most frequent complaints caused by impacted mandibular third molars, regardless of their proximity to the inferior alveolar nerve (IAN). [1],[2] Surgical removal of such molars is often indicated when conservative palliative approaches fail to relieve the pain and inflammation. [2] Problems inherent in the surgical procedure can be encountered during or after the extraction procedure. Most common complications are alveolitis, infection, and paresthesia associated to IAN damage as well as mandibular fracture and periodontal tissue loss distal to the second molar although less frequently seen. [1],[2],[3],[4]
In order to reduce these possible risks, orthodontic extrusion and subsequent extraction of impacted third molars, also called orthodontic extraction, were advocated. [3],[4],[5] This procedure may facilitate safer extraction of impacted molars with less contact to adjacent tissues. [3],[4],[5],[6] Furthermore, it allows new bone formation distal to the second molar and apical to third molar during the occlusal movement of the impacted tooth depositing bone as it departs from the IAN and the mandibular angulus border. [3],[4],[5],[6] This, in turn, reduces the risk of IAN damage, angulus fracture and periodontal tissue loss being advantageous for the patients. [2],[3],[4],[6],[7]
In this present case report, orthodontic extrusion and surgical extraction of an impacted mandibular third molar with 6-months follow-up are presented.
| Case Description | | |
Patient History, Clinical and Radiographic Examinations
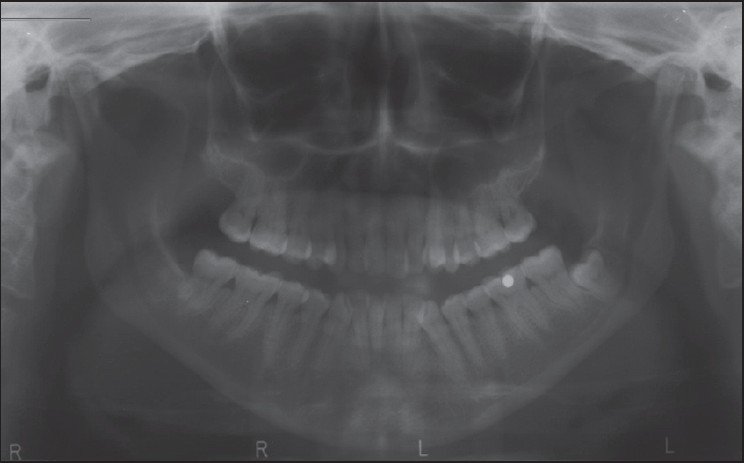
A 41-year-old female with facial pain on the left side was referred to the local dental faculty in Izmir, Turkey. She reported absence of any diagnosed systemic illnesses. Her chief complaint was the deep blunt pain located on the left masseter area that gradually increased in the last 12 months which was accompanied with the feeling of paresthesia forming lately. Clinical examination revealed restricted maximum mouth opening (35 mm) indicating possible inflammation of masticatory muscles or temporomandibular joint. Panoramic radiograph [Figure 1] revealed the presence of a fully impacted mesioangular left mandibular third molar tooth #38. Due to the deep vertical position and close proximity to the second mandibular molar, a cone-beam computed tomography was prescribed to obtain the precise topographic localization. An anatomic intersection between the impacted molar roots and the mandibular canal as well as a close relationship between the crown of the third molar and the second molar roots were confirmed [Figure 2]a and b. | Figure 2: (a) and (b) Sagittal and transversal slices of tomographic images showing the proximity of impacted molar roots and inferior alveolar nerve
Click here to view |
| Surgical Procedure and Orthodontic Extrusion Mechanics | | |
Surgical exposure of tooth #38 under local anesthesia was performed via elevation of a mucoperiosteal flap and removal of overlying bone. Inflammatory tissue remnants distal to the second molar root were debrided using a periodontal scaler. A button was bonded on the occlusal surface of the impacted molar and a stainless steel ligature was extended buccoocclusally. Mucoperiosteal flap was sutured back to its original position with the ligature extending from the incision line in the direction of planned orthodontic traction. No antibiotics or anti-inflammatory medication was prescribed; only application of extraoral cold compression was instructed.
Sutures were removed after 1 week and a 0.016*0.016" rectangular stainless-steel cantilever arm passively fitting the buccal aspects of teeth #34, 35, 36 with a loop medially positioned to #36 was bonded on the enamel surface. The tip of the cantilever arm was tied to the wire ligature extending from the impacted molar, exerting a light extrusive force in the buccoocclusal direction.
Postoperative Evaluation
The facial pain on the left side presented a gradual decrease as well as the restriction in the maximum mouth opening in the weeks following the application of orthodontic traction forces. At the 6-month follow-up, no orofacial pain (OFP) or paresthesia was reported. A follow-up periapical radiograph was obtained and the separation of the impacted molar from the IAN was observed [Figure 3]. The tooth was surgically removed following 9 months of orthodontic traction [Figure 4]. Bone healing was observed at the end of 6-months after surgical removal [Figure 5]. | Figure 3: Periapical radiograph showing the separation of the impacted tooth from inferior alveolar nerve
Click here to view |
 | Figure 5: Periapical radiograph showing bone healing after 6-months follow-up
Click here to view |
| Discussion | | |
In this case report, the diagnosis and treatment of a female patient with pain and partial paresthesia in the left facial area was presented. Orthodontic extraction is not the common choice of treatment in impacted third molar cases, since it requires relatively long treatment time. [3],[4] Furthermore, orthodontic appliances cause discomfort for the patient. [3],[4] However, as the vertical position of the impacted tooth gets deeper and closer to the IAN, the risk of neurological complications and the amount of bone that is to be removed increases. [1],[2],[3],[4] This, in turn, escalates the postoperative complications such as paresthesia and risk of infection as well as swelling and pain. [1],[2],[3],[4] Therefore, orthodontic extraction presents an alternative treatment modality in cases of severely impacted third molars with less postoperative edema and reduced risk of IAN damage. [3],[4],[5],[6]
One possible advantage of orthodontic extrusion is the periodontal status of the second molar on the distal aspect. [3] Due to the inflammatory processes and surgical intervention, attachment and bone loss is encountered occasionally distal to the second molar neighboring the impacted third molar. [3] It was claimed that the periodontal status would be conserved better with the orthodontic extraction approach due to the less extensive surgical intervention. [3] In the present case, level of bone and periodontal attachment stayed stable during and following the extrusion and surgical removal of the third molar. This finding was in accordance with previous reports.
Orthodontic mechanics used during the extrusion of the impacted molar is another important factor determining the outcome. [4],[5],[6],[8] In this present case, short crown length of the lower molar and the extruded cusp of the upper molar dictated the bonding of the cantilever arm directly on the teeth surface instead of using brackets as carriers. This made the activation of the cantilever arm impossible, because it was fixed to the teeth surface providing the extrusive force. However, rewinding of the extending ligature wire and tying the cantilever tip closer to the impacted tooth made relative reactivations possible. Nevertheless, use of brackets when possible will facilitate superior control of extrusive mechanics, which can be manipulated at each session.
| Conclusion | | |
Orthodontic extrusion of severely impacted third molars prior to extraction might be an alternative treatment modality for safer surgical procedure and to reduce postoperative complications.
| References | | |
| 1. | Dogan D, Orhan K, Gunaydin Y, Koymen R, Okcu K, Ucok O. Unerupted mandibular third molars: Symptoms, associated pathologies, and indications for removal in a Turkish population. Quintessence Int 2007;38:e497-505. 
|
| 2. | Bui CH, Seldin EB, Dodson TB. Types, frequencies, and risk factors for complications after third molar extraction. J Oral Maxillofac Surg 2003;61:1379-89.
[PUBMED] |
| 3. | Bonetti GA, Parenti SI, Checchi L. Orthodontic extraction of mandibular third molar to avoid nerve injury and promote periodontal healing. J Clin Periodontol 2008;35:719-23.
[PUBMED] |
| 4. | Alessandri Bonetti G, Bendandi M, Laino L, Checchi V, Checchi L. Orthodontic extraction: Riskless extraction of impacted lower third molars close to the mandibular canal. J Oral Maxillofac Surg 2007;65:2580-6.
[PUBMED] |
| 5. | Kim JW, Park JY, Baek SH, Kim Tw, Chang YI. Forced eruption of an impacted third molar using a bracket-head miniscrew. J Clin Orthod 2010;44:313-8.
[PUBMED] |
| 6. | Park W, Park JS, Kim YM, Yu HY, Kim KD. Orthodontic extraction of the lower third molar with an orthodontic mini implant. Oral Surg Oral Med Oral Pathol Oral Radio Endod 2010;110:e1-6.
|
| 7. | Blaeser BF, August MA, Donoff RB, Kaban LB, Dodson TB. Panoramic radiographic risk factors for inferior alveolar nerve injury after third molar extraction. J Oral Maxillofac Surg 2003;61:417-21.
[PUBMED] |
| 8. | Wang Y, He D, Yang C, Wang B, Qian W. An easy way to apply orthodontic extraction for impacted lower third molar compressing to the inferior alveolar nerve. J Craniomaxillofac Surg 2012;40:234-7.
[PUBMED] |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5]
|











 Search Pubmed for
Search Pubmed for