|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2014 | Volume
: 2
| Issue : 2 | Page : 85-89 |
|
Comparison of tooth size discrepancies in patients who have had upper anterior supernumerary teeth and a control group
Khaled Khalaf
Department of Orthodontics, University of Aberdeen, United Kingdom
| Date of Web Publication | 22-Apr-2014 |
Correspondence Address:
Khaled Khalaf
University of Aberdeen Dental School and Hospital, Cornhill Road, Foresterhill, AB25 2ZR, Aberdeen
United Kingdom
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.131119

Context: There have been a number of studies of tooth size discrepancy (TSD) in various populations, but none has investigated TSD in patients who have had upper anterior supernumerary teeth. Aims: The aim of the following study is to investigate TSD in patients who have had upper anterior supernumerary teeth. Settings and Design: This is a cross-sectional, case-control analytical study of an orthodontic sample carried out at Aberdeen Dental Hospital, University of Aberdeen, UK. Subjects and Methods: Mesiodistal dimensions of the permanent teeth on 120 study models of orthodontic patients (40 with upper anterior supernumerary teeth and 80 controls) were measured to determine anterior and overall Bolton ratios as well as the tooth size corrections. Statistical Analysis Used: Chi-square test was used to compare the supernumerary group with the control with regards to the incidence of TSD. Results: The percentage of subjects with anterior and an overall TSD in the supernumerary group was similar to that in the control group, however the supernumerary group had a greater percentage of patients who had smaller anterior and overall ratios more than 2 standard deviations (SDs) of Bolton's mean than the control group and the opposite holds true for those who had higher ratios more than 2 SDs of Bolton's mean (P < 0.05). Similar results were found when TSD was expressed in millimetric means (P < 0.05). Conclusions: Patients who have had anterior supernumerary teeth have a relative tooth tissue excess in the maxillary arch compared with the control group and thus may require tooth tissue reduction of the maxillary teeth to achieve optimal orthodontic outcome. Keywords: Anterior, Bolton ratio, overall, supernumerary, tooth size discrepancy
How to cite this article:
Khalaf K. Comparison of tooth size discrepancies in patients who have had upper anterior supernumerary teeth and a control group. J Orthod Res 2014;2:85-9 |
How to cite this URL:
Khalaf K. Comparison of tooth size discrepancies in patients who have had upper anterior supernumerary teeth and a control group. J Orthod Res [serial online] 2014 [cited 2018 Mar 6];2:85-9. Available from: http://www.jorthodr.org/text.asp?2014/2/2/85/131119 |
| Introduction | |  |
Tooth size discrepancy (TSD) is a mismatch in tooth dimensions between the mandibular and maxillary teeth. It is not an uncommon reason for failure to achieve good occlusion in orthodontic patients as it affects the overjet, overbite and buccal interdigitation. [1],[2],[3]
Several studies have suggested various methods of detecting and quantifying TSD, [4],[5] but the most known is a study by Bolton, [1] in which he developed two ratios for estimating TSD, the anterior and overall ratios.
Some authors consider a ratio of beyond one standard deviation (SD) of the mean to be of significant diagnostic value. [2],[6] While others consider TSD to be present in a given malocclusion when the ratios are more than 2 SDs from Bolton's mean. [3],[7],[8] Othman and Harradine [9] have suggested that TSD is better expressed in terms of millimeters required for correction, with a recommended threshold of 2 mm. The question of which method should be used to best express a clinically significant TSD was investigated by Endo et al.[10] They found that TSD is better expressed in terms of both Bolton's ratios and the amount of tooth size correction in millimeters. They recommended that Bolton's ratio beyond 2 SDs of Bolton's mean and mandibular or maxillary corrections beyond 2 mm are considered to be thresholds for clinically significant TSD.
It has been found that patients with supernumerary teeth tend to have larger tooth sizes than the average population and anomalous tooth shape. [11],[12],[13],[14] Hence, this poses an important question of whether this group of patients have a different incidence and type of TSD than a population with a numerically normal dentition. Although, there have been a number of studies of TSD in subjects with numerically normal dentitions in various populations [3],[8],[15],[16],[17],[18],[19],[20],[21] none has investigated TSD in orthodontic patients with upper anterior supernumerary teeth. Therefore, the aim of the present study was to investigate TSD in patients who have had upper anterior supernumerary teeth and to compare this with a control group.
| Subjects and Methods | | |
The sample consisted of 120 pre-treatment study models of orthodontic patients. The control group comprised 80 orthodontic patients selected retrospectively and consecutively from the orthodontic treatment list (35 males and 45 females; mean age 14.43 years) and the study group 40 supernumerary tooth patients who had 48 supernumerary teeth [23 males and 17 females; mean age 14.07 years, [Table 1]] referred for orthodontic treatment. The vast majority of supernumerary teeth (42) was of conical form and located between the upper central incisors. The remaining few supernumerary teeth were either of the tuberculate type (4) or supplemental lateral incisors (2) and all located in the upper anterior region. All subjects were white Caucasians, with no general medical conditions or syndromes, had no missing teeth and no previous orthodontic treatment and had all the permanent teeth from the first molar to the contralateral first molar erupted and intact (no interproximal caries and/or restorations and minimal or no tooth wear). All subjects fulfilling the above criteria were chosen from the orthodontic treatment waiting list and thus the sample represented a random distribution of malocclusions.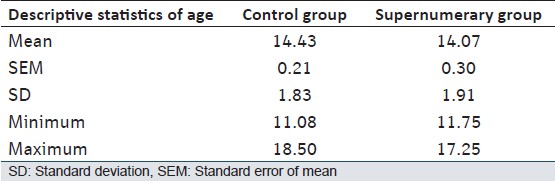 | Table 1: Age distribution (years) in the supernumerary and control groups
Click here to view |
The mesiodistal diameter of each tooth was measured to the nearest 0.1 mm using digital Vernier calipers as described by Moorrees and Reed [22] and defined as the maximum distance between the proximal mesial and distal surfaces at the contact points. All measurements were carried out by one trained operator (KK) twice and the mean value of the two measurements was used. The Bolton ratios and the required tooth size corrections were calculated.
The method error, including the systematic and random error, was assessed on repeated measurements of 20 randomly selected study models (10 upper and 10 lower) taken 4 weeks apart. There was no systematic bias as the paired sample t-test showed none of the differences were statistically significant (P > 0.05). Random error was assessed in terms of the repeatability coefficient which represents a range of agreement within which 95% of the differences in measurements would lie. The method showed a high level of repeatability with a maximum value of the repeatability coefficient of 0.38 mm.
Statistical Analysis
Statistical analyses were carried out using the Statistical Package for Social Sciences (SPSS Inc., Chicago, Illinois, USA) version 17.0. A two sample t-test was used to compare the means of Bolton ratios between males and females as their data were found to be normally distributed. Each subject in each of the supernumerary and control groups was classified in one of the three following categories: A TSD with an anterior/overall ratio ≤ 2 SD, a TSD with anterior/overall ratio ≥ 2 SD, or no TSD with an anterior/overall ratio between −2 SD and +2 SD. The differences in the frequencies of subjects falling into one of the above three categories between the supernumerary and control groups were tested using a Chi-square test. The same method was used to determine the differences in the frequencies of subjects falling into similar categories to the above (but in millimetric terms) of anterior and overall corrections in the lower and upper arches. The categories for tooth size corrections were ≤ 2 mm, ≥ 2 mm and between −2 mm and +2 mm.
| Results | | |
No significant differences were found in mean anterior and overall Bolton ratios between genders (P > 0.05, t-test), hence the genders were combined for all further analyses.
[Table 2] shows Bolton's ratios in the supernumerary and control groups. The anterior and overall mean ratios for the supernumerary group were smaller than those of the control group and the former had larger SDs than the latter and thus a greater variability.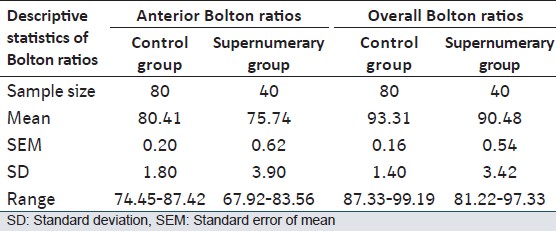 | Table 2: Anterior and overall Bolton ratios in the supernumerary and control groups
Click here to view |
[Table 3] shows the number and percentage of subjects with an anterior and overall ratio in the supernumerary and control groups. For both anterior and overall ratios the supernumerary group had a greater percentage of patients with ratios less than 2 SDs than the control group and the opposite holds true for patients with ratios greater than 2 SDs [Table 3] with the differences being statistically significant (P < 0.001, Chi-square test). | Table 3: Number and percentage of subjects (in parentheses) with anterior and an overall ratio in the supernumerary and control groups
Click here to view |
[Table 4] shows the number and percentage of subjects with an anterior and overall correction (in millimeters) in the supernumerary and control groups. As it can be seen from [Table 4], the supernumerary group had a greater percentage of subjects who will require an increase of the mandibular teeth or a reduction of the maxillary teeth to correct tooth size to achieve Bolton's means than that of the control group with the differences being statistically significant (P = 0.001, Chi-square test). This would suggest that there was a relative tooth size excess of the maxillary arch in the supernumerary group as a consistent feature.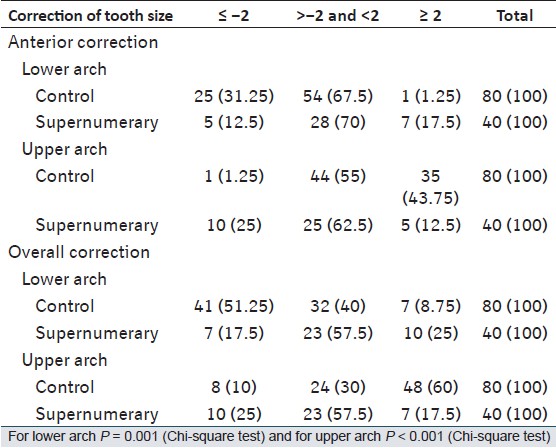 | Table 4: Number and percentage of subjects (in parentheses) with an anterior and overall correction (in mm) in the supernumerary and control groups
Click here to view |
| Discussion | | |
The study group included patients with upper anterior supernumerary teeth and with various malocclusions referred for orthodontic treatment. Thus, it does not represent upper anterior supernumerary tooth subjects in the general population and therefore the results need to be interpreted with caution. The control group was selected from consecutively treated orthodontic patients with various malocclusions, thus matching the supernumerary group in composition except the absence of supernumerary teeth and a larger size than the supernumerary group. Bearing in mind the low prevalence of supernumerary teeth in the general population at 2.1% [23] and the inclusion criteria above, the sample size of the supernumerary group was still adequate for appropriate statistical analysis and comparison with the control group.
Although males had larger Bolton's ratios than females the differences were not statistically significant. This agrees with studies of TSD in a numerically normal dentition that found either no gender dimorphism in mean Bolton's ratios [9],[10],[16],[19] or a slightly larger ratios for males than females, albeit less than 1%. [15],[17] In the present study and in both supernumerary and control groups and as in all previous studies, the percentage of subjects having an overall arch ratio beyond 2 SDs of Bolton's mean was smaller than that of subjects with the corresponding figure for the anterior ratio. This is may be due to the greater variability of tooth size of the anterior teeth when compared with the posterior teeth. [24]
The incidence of anterior and an overall TSD in the control group in the present investigation was higher than that of previous studies of TSD in orthodontic populations with numerically normal dentitions. [3],[6],[7],[8],[9],[25] In the present study, TSD of the anterior ratio was 45% and of the overall ratio 23.75%, whereas in previous studies the range was 17.4-30.6% and 5.4-13.5%, respectively. This difference in the anterior and overall TSD between the present and previous studies was due to differences in sampling techniques, sample composition, size and method of expressing TSD. Araujo and Souki [6] used ±1 SD as a definition of TSD whilst others [3],[7],[8],[9],[25] used +> 2 SD and −< SD as a measure of TSD. In the present study, TSD was defined as +≥ 2 SD and −≤ 2 SD and +≥ 2 mm and −≤ 2 mm as suggested by Endo et al. [10]
It is not possible to compare the results of the supernumerary group with similar studies, as to date this is the first to report TSD in patients with upper anterior supernumerary teeth referred for orthodontic treatment.
Although, there was no difference in the percentage of subjects who had anterior and an overall TSD between the supernumerary and control groups, the type of TSD was statistically significantly different between the two groups (P < 0.05, Chi-square test). A large proportion of the supernumerary tooth patients had equal or smaller ratios than -2 SD of Bolton's mean, whereas a large proportion of the control group patients had equal or greater ratios than 2 SD of Bolton's mean. This would suggest a relative tooth tissue excess of the mandibular teeth in the control group in agreement with the findings of Othman and Harradine [9] and a relative tooth excess of the maxillary teeth in the supernumerary group. In addition, tooth size excess of the maxillary teeth was pronounced more anteriorly [25% of supernumerary patients had an anterior ratio equal to or less than -2 SD compared with 1.25% of the control, [Table 3]] than over the whole dentition [17.5% of supernumerary patients had overall ratio equal to or less than -2 SD compared with 1.25% of the control, [Table 3]]. As all the supernumerary teeth in the supernumerary group were located in the upper anterior region it appears that the impact of the presence of supernumerary teeth on tooth size of the remaining dentition and subsequently mean Bolton's tooth ratio was so significant such that the latter became smaller than -2 SD rather than greater than 2 SD in the control group. Further support to this finding can be drawn from previous odontometric studies in patients with supernumerary teeth [11],[12],[14] that have found a tendency for the remaining dentition of patients with supernumerary teeth to be larger in size than the average population with a "local field effect theory" so that the closer the teeth to the location of the supernumerary tooth the more affected their size. These findings also indicate that the impact of the presence of supernumerary teeth on TSD involves the whole dentition, but to a greater extent in the anterior region.
It is interesting to note that when expressing TSD in millimetric terms, the percentage of cases deemed to have a significant problem was greater for the overall arch but similar for the anterior segment compared with the corresponding figures of Bolton's ratios, a finding which was reported by others. [8],[9]
| Conclusions | | |
- An orthodontic population with upper anterior supernumerary teeth has a similar incidence of clinically significant TSD to that of an orthodontic population with a normal complement of teeth, but the type of TSD was statistically significantly different between the two groups.
- Orthodontic patients who have had upper anterior supernumerary teeth may have a relative tooth size excess of the maxillary arch and thus will require tooth size reduction of the upper teeth to achieve optimal intra-arch alignment and inter-arch relationships.
- Orthodontic patients with a normal complement of teeth may have a relative tooth size excess of the mandibular arch and thus may require tooth size reduction of the lower teeth to achieve optimal intra-arch alignment and inter-arch relationships.
| References | | |
| 1. | Bolton WA. Disharmony in tooth size and its relation to the analysis and treatment of malocclusion. Angle Orthod 1958;28:113-30. 
|
| 2. | Bolton WA. The clinical application of tooth-size analysis. Am J Orthod 1962;48:504-29.
|
| 3. | Crosby DR, Alexander CG. The occurrence of tooth size discrepancies among different malocclusion groups. Am J Orthod Dentofacial Orthop 1989;95:457-61.
|
| 4. | Steadman SR. The relation of upper anterior teeth to lower anterior teeth as present on plaster models of a group of acceptable occlusions. Angle Orthod 1952;22:91-7.
|
| 5. | Lundstrom A. Intermaxillary tooth width ratio and tooth alignment and occlusion. Acta Odontol Scand 1955;12:265-92.
[PUBMED] |
| 6. | Araujo E, Souki M. Bolton anterior tooth size discrepancies among different malocclusion groups. Angle Orthod 2003;73:307-13.
|
| 7. | Freeman JE, Maskeroni AJ, Lorton L. Frequency of Bolton tooth-size discrepancies among orthodontic patients. Am J Orthod Dentofacial Orthop 1996;110:24-7.
|
| 8. | Bernabé E, Major PW, Flores-Mir C. Tooth-width ratio discrepancies in a sample of Peruvian adolescents. Orthod Craniofac Res 2004;6:173-6.
|
| 9. | Othman S, Harradine N. Tooth size discrepancies in an orthodontic population. Angle Orthod 2007;77:668-74.
|
| 10. | Endo T, Uchikura K, Ishida K, Shundo I, Sakaeda K, Shimooka S. Thresholds for clinically significant tooth-size discrepancy. Angle Orthod 2009;79:740-6.
|
| 11. | Brook AH, Elcock C, al-Sharood MH, McKeown HF, Khalaf K, Smith RN. Further studies of a model for the etiology of anomalies of tooth number and size in humans. Connect Tissue Res 2002;43:289-95.
|
| 12. | Khalaf K, Robinson DL, Elcock C, Smith RN, Brook AH. Tooth size in patients with supernumerary teeth and a control group measured by image analysis system. Arch Oral Biol 2005;50:243-8.
|
| 13. | Khalaf K, Smith RN, Elcock C, Brook AH. Multiple crown size variables of the upper incisors in patients with supernumerary teeth compared with controls. Arch Oral Biol 2009;54 Suppl 1:S71-8.
|
| 14. | Brook AH, Griffin RC, Smith RN, Townsend GC, Kaur G, Davis GR, et al. Tooth size patterns in patients with hypodontia and supernumerary teeth. Arch Oral Biol 2009;54 Suppl 1:S63-70.
|
| 15. | Lavelle CL. Maxillary and mandibular tooth size in different racial groups and in different occlusal categories. Am J Orthod 1972;61:29-37.
[PUBMED] |
| 16. | Richardson ER, Malhotra SK. Mesiodistal crown dimension of the permanent dentition of American Negroes. Am J Orthod 1975;68:157-64.
[PUBMED] |
| 17. | Smith SS, Buschang PH, Watanabe E. Interarch tooth size relationships of 3 populations: "Does Bolton′s analysis apply?" Am J Orthod Dentofacial Orthop 2000;117:169-74.
|
| 18. | Ta TA, Ling JY, Hägg U. Tooth-size discrepancies among different occlusion groups of southern Chinese children. Am J Orthod Dentofacial Orthop 2001;120:556-8.
|
| 19. | Al-Tamimi T, Hashim HA. Bolton tooth-size ratio revisited. World J Orthod 2005;6:289-95.
|
| 20. | Akyalçin S, Doðan S, Dinçer B, Erdinc AM, Oncað G. Bolton tooth size discrepancies in skeletal Class I individuals presenting with different dental angle classifications. Angle Orthod 2006;76:637-43.
|
| 21. | Paredes V, Gandia JL, Cibrian R. Do Bolton′s ratios apply to a Spanish population? Am J Orthod Dentofacial Orthop 2006;129:428-30.
|
| 22. | Moorrees CF, Reed RB. Correlations among crown diameters of human teeth. Arch Oral Biol 1964;9:685-97.
[PUBMED] |
| 23. | Brook AH. Dental anomalies of number, form and size: Their prevalence in British schoolchildren. J Int Assoc Dent Child 1974;5:37-53.
[PUBMED] |
| 24. | Yuen KK, So LL, Tang EL. Mesiodistal crown diameters of the primary and permanent teeth in southern Chinese - A longitudinal study. Eur J Orthod 1997;19:721-31.
|
| 25. | Al-Omari IK, Al-Bitar ZB, Hamdan AM. Tooth size discrepancies among Jordanian schoolchildren. Eur J Orthod 2008;30:527-31.
|
[Table 1], [Table 2], [Table 3], [Table 4]
|










 Search Pubmed for
Search Pubmed for