|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 3
| Issue : 2 | Page : 124-128 |
|
Evaluation of vertical mandibular asymmetry in unilateral and bilateral posterior crossbite adult patients
Amjad Al Taki1, Omar Othman2, Fatma Al Kaddah1
1 Private Practice, Dubai, United Arab Emirates
2 Department of Orthodontics, College of Dentistry, Ajman University of Science and Technology, Ajman, United Arab Emirates, United Arab Emirates
| Date of Web Publication | 15-May-2015 |
Correspondence Address:
Amjad Al Taki
Private Practice, P.O. Box 10462, Dubai, United Arab Emirates
United Arab Emirates
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.149067

Objective : t0 he aim of this study was to estimate possible differences in skeletal asymmetry between group of adult subjects with normal occlusion and unilateral and bilateral posterior crossbite malocclusions. Materials and Methods: A sample of 91 subjects (consisted of 37 unilateral posterior crossbite [14 male and 23 female; mean age 22.49 ± 4.19 years] and 31 bilateral posterior crossbite patients [18 male and 13 female; mean age 24.36 ± 3.76 years] and a control group (CG) of 23 subjects with normal occlusion [13 male and 10 female; mean age 22.74 ± 1.74 years]) was examined in the study. Condylar, ramal, and condylar-plus-ramal asymmetry values were measured for all subjects on panoramic radiographs. Data were analyzed statistically by means of paired t-test. Results: Unilateral crossbite group (UCG) and bilateral cossbite group (BCG) showed significant asymmetric indices (condylar, ramal, and condylar-plus-ramal) relative to the CG, except for condylar index when comparing BCG and CG (P > 0.05). Comparisons within the crossbite groups showed no statistically significant differences in condylar, ramal, or condylar-plus-ramal heights (RHs) between left and right sides of the UCG, while for the BCG, significant difference was found only for the condylar-plus-RH (P < 0.05). Conclusions : b0 oth UCG and BCG have asymmetrical condyles compared to CG. Side comparisons within crossbite groups showed asymmetric mandible in BCG. Keywords: Condylar asymmetry, panoramic radiograph, posterior crossbite, ramal asymmetry
How to cite this article:
Al Taki A, Othman O, Al Kaddah F. Evaluation of vertical mandibular asymmetry in unilateral and bilateral posterior crossbite adult patients
. J Orthod Res 2015;3:124-8 |
How to cite this URL:
Al Taki A, Othman O, Al Kaddah F. Evaluation of vertical mandibular asymmetry in unilateral and bilateral posterior crossbite adult patients
. J Orthod Res [serial online] 2015 [cited 2018 Sep 6];3:124-8. Available from: http://www.jorthodr.org/text.asp?2015/3/2/124/149067 |
| Introduction | |  |
Assessing symmetry is important in any esthetic evaluation of the craniofacial region. Posterior crossbite is a reverse occlusion of at least one buccal tooth including the canine. In most patients, insufficient maxillary arch width accounts for the transverse discrepancy. [1],[2]
The causes of maxillary constriction can be abnormal finger-sucking habits, perverted perioral muscle functions, premature primary tooth loss, and obstruction of the upper airway. [3]
Untreated unilateral posterior crossbite could cause an asymmetry in condylar position, with displacement of the ipsilateral condyle toward the crossbite side and increased growth of the contralateral condyle. [4] Accordingly, an asymmetrically positioned mandible in a unilateral crossbite patient might lead to asymmetrical condylar heights (CHs).
Habets et al. [5] introduced a method to determine asymmetries between the condyles of the mandible. This method compared the vertical heights of the mandibular right and left condyles and rami.
Habets et al. method has been used for diagnosis in temporomandibular-disorder patients. [6] In addition, it was used to determine condylar asymmetries in various malocclusions such as Class II and III [7],[8] and in various skeletal patterns. [9],[10]
In literature, there are fewer studies comparing mandibular vertical asymmetry using the method of Habets et al. [5] in unilateral and bilateral crossbite patients with a normal occlusion sample. Uysal et al. [11] investigated condylar asymmetry with the method of Habets et al. in adolescent patients with unilateral and bilateral posterior crossbites and a normal occlusion sample and found no significant difference between the groups. Veli et al. [12] studied mandibular asymmetry in unilateral and bilateral posterior crossbite patients using cone-beam computed tomography and found that bilateral crossbite patients have side-specific asymmetry.
The aim of this study was to investigate vertical condylar and ramal asymmetry in a group of untreated adult patients with unilateral and bilateral posterior crossbite malocclusions and compare them with a control group (CG) with normal occlusion.
| Materials and Methods | | |
This study examined panoramic radiographs of 91 patients presenting for routine orthodontic treatment at Ajman University of Science and Technology obtained as part of diagnostic record gathering. The subjects were divided into three groups: 23 subjects with normal occlusion, 37 subjects with unilateral crossbite, and 31 subjects with bilateral posterior crossbite.
The inclusion criteria for CG were as the following:
- Class I canine and molar relationships with minor or no crowding;
- No missing teeth, excluding the third molars;
- No history of orthodontic treatment or facial trauma;
- No signs or symptoms of temporomandibular disorder (TMD).
The inclusion criteria for unilateral crossbite group (UCG) were as following:
- Unilateral posterior crossbites involving at least 2 posterior teeth in crossbite;
- Functional unilateral posterior crossbite, as reported in the clinical history;
- Mandibular dental midline deviation of at least 1 mm to the crossbite side;
- No remarkable facial asymmetry;
- Absence of any severely malaligned or blocked out teeth;
- No missing teeth, excluding the third molars.
The inclusion criteria for bilateral crossbite group (BCG) were as following:
1. Bilateral posterior crossbites involving at least 2 posterior teeth in crossbite on both sides.
Selection criteria numbered 4-6 for UCG were also valid for the BCG.
As panoramic radiographs are routinely used as a diagnostic tool in the orthodontic clinics, all subjects had films available for evaluation. The same image size was taken in the standard manner and standard size. All films were traced and measured manually by the first author.
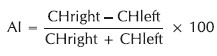
Habets' technique [5] was used to assess the mandibular asymmetry. This technique consists of measuring the vertical height of the right and left condyles on the panoramic X-ray [Figure 1]. A tangent (A) is traced to the most lateral points of the ramus (O1) and the condyle (O2). Then a perpendicular (B) is traced to the line A, tangential to the highest point of the condyle. The CH corresponds to the distance measured between the tangent (B) to the most lateral point of the condyle (O1), and the ramal height (RH) corresponds to the measurement that goes from the most lateral point of the ramus to the most lateral point of the condyle (distance between O1 and O2). Thus, a condylar asymmetry index (CAI) is proposed that is obtained by applying the following formula: | Figure 1: Measuring vertical mandibular asymmetry by Habets et al. method
Click here to view |
Statistical analysis
To determine the errors associated with tracing and measuring, 20 radiographs were selected randomly. Tracing and measuring the radiographs were repeated 2 weeks later. A paired t-test was used for the first and second measurements, and no error was found.
A paired t-test was used to determine the differences in condylar, ramal, and condylar-plus-RHs between the left and right sides of the subjects in each group. T-test was also applied to determine whether there was any difference between the asymmetry indices of the groups. Statistical analysis was performed using the SPSS software package (version 19.0, SPSS Inc., Chicago, IL, USA). The results were regarded as statistically significant at P < 0.05.
| Results | | |
The statistical data and the results of paired t-tests comparing the measurements of the left and right sides in UCG and BCG are presented in [Table 1] and [Table 2], respectively. Comparisons within the crossbite groups showed no statistically significant differences in CH, RH, or CH + RH between left and right sides of the UCG, while for the BCG, significant difference was found only for the CH + RH (P < 0.05).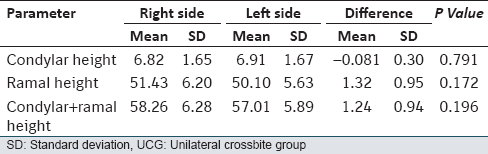 | Table 1: Descriptive statistics of side comparison in UCG (paired t-test)
Click here to view |
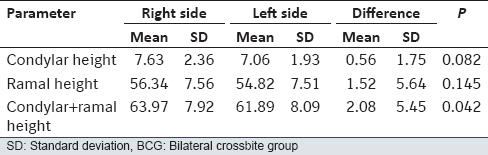 | Table 2: Descriptive statistics of side comparison in BCG (paired t-test)
Click here to view |
Comparisons of the asymmetry indices between the CG and the crossbite groups are shown in [Table 3] and [Table 4]. [Table 3] showed statistically significant differences between CG and UCG for the CAI, ramal AI (RAI), condylar and ramal AI (CRAI). On the other hand, [Table 4] showed significant differences between CG and BCG for the RAI and CRAI only.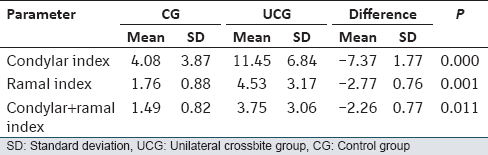 | Table 3: Descriptive statistics and comparison of mandibular asymmetry indices between CG and UCG (paired t-test)
Click here to view |
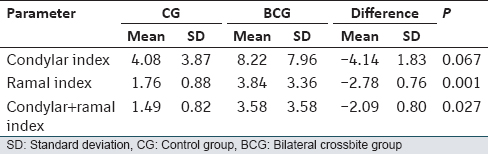 | Table 4: Descriptive statistics and comparison of mandibular asymmetry indices between CG and BCG (paired t-test)
Click here to view |
Comparisons of the asymmetry indices between the crossbite groups are shown in [Table 5]. No significant difference was observed for any of the asymmetry indices.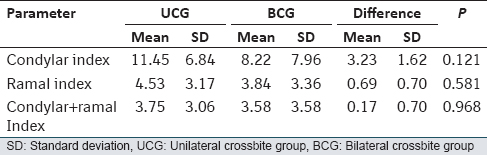 | Table 5: Descriptive statistics and comparison of mandibular asymmetry indices between UCG and BCG (paired t-test)
Click here to view |
| Discussion | | |
Assessment of mandibular asymmetry has been performed using submentovertex, [13] postero-anterior cephalometric radiographs, [14] and computed tomography. [15] However, panoramic radiographs are the most frequently used viewing technique because it is possible to image joints, teeth, and other parts of the jaws in one exposure.
Panoramic radiographs are known to provide a reproducible vertical and angular measurements if they were recorded properly. [16] Thus in the present study, orthopantomogram were used for evaluation of mandibular asymmetry. Habets et al. [5] concluded that the head holder must be fixed well to the OPG, and the head has to be well centered in the head holder of the OPG when a clinical OPG is to be evaluated. In this study, the age of all subjects was >18 years to ensure that mandibular growth had reached adult levels.
The sex differences of the groups did not seem to be a problem because studies of the vertical condylar and ramal asymmetries in which sex differences were investigated found no statistically significant differences. [5],[11],[16],[17]
Results of the side comparison of UCG showed that CH, RH, CH + RH were similar on the right and left sides, and no statistically significant side differences were found. Our result was in agreement with Uysal et al. [11] who found no significant side-specific asymmetry for unilateral crossbite patients. On the other hand, some authors reported vertical mandibular asymmetry in unilateral posterior crossbite patients. Kilic et al. [18] found that CH, RH, CH + RH were significantly smaller on the crossbite side than on the corresponding side in unilateral posterior crossbite patients.
Side comparisons results of BCG revealed a significant difference in the CH + RH, which indicates that bilateral crossbite patients have asymmetric mandibles. Similar results were observed by Halicioglu et al., [19] who found that bilateral crossbite patients have asymmetric RHs. Another study by Veli et al. [12] concluded that contrary to UCG, BCG was found to have side-specific asymmetry.
The method described by Habets et al. [5] has been used for evaluating condylar and ramal asymmetries in TMD patients and in various malocclusions. According to Habets et al., a 3% index ratio can result from a 1-cm change in head position while the panoramic radiograph is being taken, and thus AI values (CAI, RAI, and CRAI) >3% should be considered as mandibular posterior vertical asymmetry.
In this study, in UCG, BCG, and CG, CAIs were found above 3% (11.45 ± 6.84%, 8.22 ± 7.96%, 4.08 ± 3.87%, respectively) indicating the presence of asymmetry.
Other studies evaluating condylar asymmetry with this method in different malocclusions and in TMD patients also found asymmetry values >3% both in study and CGs. [9],[11],[12],[19] These high values indicating asymmetry both in experimental and CGs can be attributed to shape, angular and positional differences between right and left condyles without any pathology or without any related malocclusion.
Cohlmia et al. [20] found that left condyle was positioned more anteriorly than the right condyle. Kambylafkas et al. [14] stated that CH was unreliable when determining asymmetry from the panoramic radiograph because of the small dimension of the measurement and operator error in tracing and identifying landmarks.
Inui et al. [21] suggested that continuous condylar displacement in the glenoid fossa during the growth period, derived from occlusal problems, induced differential growth of the left and right condyles. From this perspective, these asymmetries could be the result of a functional deviation of the mandible in all subjects in the crossbite group, or it is explained by either adaptation of the condyle or systematic measurement errors because of the small dimension of condyle.
Comparisons of asymmetry indices between UCG and CG showed statistically significant differences in CAI, RAI, CRAI, while comparisons between BCG and CG showed that the asymmetry was observed for RAI and CRAI values, rather than CAI value.
No, statistically significant differences were found in between crossbite groups for mandibular asymmetry determined separately by CAI, RAI, and CRAI.
In literature, studies that compared asymmetry indices in crossbite groups and CG showed different results. Halicioglu et al. [19] found an asymmetry between the UCB and BCB groups in RAI and CRAI values, rather than CAI values. On the other hand, Uysal et al. [11] results showed that CAI in crossbite groups and CG were high, but no statistically significant differences were found among the groups. Kiki et al. [16] compared CAI in BCG and CG and concluded that patients with bilateral posterior crossbite had more asymmetrical condyles relative to the controls.
To conclude, posterior crossbite patients have asymmetric mandibles as revealed by the high CAI values, but normal occlusion subjects also have some asymmetry. Results of this study have shown that posterior crossbite patients may act as a predisposing factor for having asymmetric mandibles, so it should be remembered that the early correction of posterior crossbite is of major importance.
| Conclusions | | |
- Mandibular side asymmetry was observed in BCG.
- Asymmetry indices were found to be significantly high in crossbite groups compared to CG.
- Comparisons between the crossbite groups were not statistically significant.
| References | | |
| 1. | McNamara JA. Maxillary transverse deficiency. Am J Orthod Dentofacial Orthop 2000;117:567-70.  |
| 2. | Allen D, Rebellato J, Sheats R, Ceron AM. Skeletal and dental contributions to posterior crossbites. Angle Orthod 2003;73:515-24. |
| 3. | Proffit WR, Fields HW, Sarver DM. The etiology of orthodontic problems. In: Contemporary Orthodontics. 5 th ed. St. Louis, Mo: CV Mosby; 2013. p. 141-5. |
| 4. | Solberg WK, Bibb CA, Nordström BB, Hansson TL. Malocclusion associated with temporomandibular joint changes in young adults at autopsy. Am J Orthod 1986;89: 326-30. |
| 5. | Habets LL, Bezuur JN, Naeiji M, Hansson TL. The Orthopantomogram, an aid in diagnosis of temporomandibular joint problems. II. The vertical symmetry. J Oral Rehabil 1988;15:465-71. |
| 6. | Miller VJ. Variation of condylar asymmetry with age in edentulous patients with a craniomandibular disorder of myogenous origin. J Prosthet Dent 1994;71:384-6. |
| 7. | Miller VJ, Bodner L. Condylar asymmetry measurements in patients with an Angle's Class III malocclusion. J Oral Rehabil 1997;24:247-9. |
| 8. | Miller VJ, Smidt A. Condylar asymmetry and age in patients with an Angle's Class II division 2 malocclusion. J Oral Rehabil 1996;23:712-5. |
| 9. | Saglam AM. The condylar asymmetry measurements in different skeletal patterns. J Oral Rehabil 2003;30:738-42. |
| 10. | Sabuncuoglu FA, Sencimen M, Varol A. Orthodontic surgical correction of two patients with asymmetrical Class III malocclusion: Case report. Turkiye Klinikleri J Dent Sci 2011;17:294-9. |
| 11. | Uysal T, Sisman Y, Kurt G, Ramoglu SI. Condylar and ramal vertical asymmetry in unilateral and bilateral posterior crossbite patients and a normal occlusion sample. Am J Orthod Dentofacial Orthop 2009;136:37-43. |
| 12. | Veli I, Uysal T, Ozer T, Ucar FI, Eruz M. Mandibular asymmetry in unilateral and bilateral posterior crossbite patients using cone-beam computed tomography. Angle Orthod 2011;81:966-74. |
| 13. | Rose JM, Sadowsky C, BeGole EA, Moles R. Mandibular skeletal and dental asymmetry in Class II subdivision malocclusions. Am J Orthod Dentofacial Orthop 1994;105:489-95. |
| 14. | Kambylafkas P, Kyrkanides S, Tallents RH. Mandibular asymmetry in adult patients with unilateral degenerative joint disease. Angle Orthod 2005;75:305-10. |
| 15. | Vitral RW, Telles Cde S. Computed tomography evaluation of temporomandibular joint alterations in class II Division 1 subdivision patients: Condylar symmetry. Am J Orthod Dentofacial Orthop 2002;121:369-75. |
| 16. | Kiki A, Kiliç N, Oktay H. Condylar asymmetry in bilateral posterior crossbite patients. Angle Orthod 2007;77: 77-81. |
| 17. | Sezgin OS, Celenk P, Arici S. Mandibular asymmetry in different occlusion patterns. Angle Orthod 2007;77:803-7. |
| 18. | Kilic N, Kiki A, Oktay H. Condylar asymmetry in unilateral posterior crossbite patients. Am J Orthod Dentofacial Orthop 2008;133:382-7. |
| 19. | Halicioglu K, Celikoglu M, Yavuz I, Sekerci AE, Buyuk SK. An evaluation of condylar and ramal vertical asymmetry in adolescents with unilateral and bilateral posterior crossbite using cone beam computed tomography (CBCT). Aust Orthod J 2014;30:11-8. |
| 20. | Cohlmia JT, Ghosh J, Sinha PK, Nanda RS, Currier GF. Tomographic assessment of temporomandibular joints in patients with malocclusion. Angle Orthod 1996;66:27-35. |
| 21. | Inui M, Fushima K, Sato S. Facial asymmetry in temporomandibular joint disorders. J Oral Rehabil 1999;26: 402-6. |
[Figure 1]
[Table 1], [Table 2], [Table 3], [Table 4], [Table 5]
|










 Search Pubmed for
Search Pubmed for