|
 
 |
| REVIEW ARTICLE |
|
| Year : 2015 | Volume
: 3
| Issue : 2 | Page : 81-87 |
|
Diagnosis and management of facial asymmetries
Sandhya Maheshwari, Sanjeev Kumar Verma, Aditi Gaur, Sushma Dhiman
Department of Orthodontics and Dental Anatomy, Dr. Z. A. Dental College, Aligarh Muslim University, Aligarh, Uttar Pradesh, India
| Date of Web Publication | 15-May-2015 |
Correspondence Address:
Aditi Gaur
Department of Orthodontics and Dental Anatomy, Dr. Z. A. Dental College, Aligarh Muslim University, Aligarh, Uttar Pradesh
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.149054

Facial esthetics evaluation is the most important part of the orthodontic treatment-planning procedure. The attainment of the best facial esthetic appearance for a given patient is a primary goal of orthodontic treatment. The evaluation of a patient's frontal symmetry is the most critical aspect of diagnosis because this is most appreciated view for any individual. Even the most esthetic faces are associated with mild forms of facial asymmetry. The individuals who report for an orthodontic treatment are often associated with facial asymmetry that may be greater than the acceptable norms. Such asymmetries may have a skeletal or dental etiology. The diagnosis, treatment planning, and the mechanics for the asymmetric patient require the identification of the cause of the asymmetry. A careful differential diagnosis together with a thorough treatment plan can ensure successful treatment outcomes in the management of such cases. Keywords: Asymmetric mechanics, deviation, distraction, facial asymmetry
How to cite this article:
Maheshwari S, Verma SK, Gaur A, Dhiman S. Diagnosis and management of facial asymmetries
. J Orthod Res 2015;3:81-7 |
| Introduction | |  |
Symmetry is defined as "equality or correspondence in terms of parts distributed around a center or an axis at the two extremes or poles or on the two opposite sides of the body." [1] The word symmetry refers to balance between structures; on the other hand asymmetry can be explained as an imbalance or disproportionation.
The phenomenon of facial asymmetry can be described as differences in size or relationship of two sides of the face. According to Severt and Proffit, [2] frequencies of facial laterality are 5%, 36% and 74% in the upper, middle, and lower thirds of the face. Minor facial asymmetry can be observed even in the most normal appearing individuals, in most of the cases left side of the face being larger than the right side. Although the opposite has also been suggested in the literature. There is a variation in the distribution of asymmetry on various parts of the craniofacial region. [3] Peck et al. [4] observed that orbital region exhibited the least asymmetry (0.87 mm), mandibular region the most (3.54 mm) and the zygomatic region exhibiting a moderate asymmetry of 2.25 mm. It was suggested that as the facial structures farther from the cranium are observed there was an increase in asymmetry. Similar findings were seen by Maeda et al. [5] who said that asymmetry most frequently in mandibular body only about 6.1% of the patients examined demonstrated a mild degree of maxillary asymmetry. Chew et al. [6] reported asymmetry in 35.8% of 212 patients with dentofacial deformities, with the majority of cases in patients with class III occlusal deformity. Among the patients reporting for orthodontic treatment the most common asymmetry trait observed is mandibular midline deviation from the facial midline occurring in 62% of patients, followed by lack of dental midline coincidence (46%), maxillary midline deviation from the facial midline (39%), molar classification asymmetry (22%), maxillary occlusal asymmetry (20%), mandibular occlusal asymmetry (18%), facial asymmetry (6%), chin deviation (4%), and nose deviation (3%). [7]
| Etiology of Facial Asymmetry | | |
Haraguchi et al. suggested that the etiology of facial asymmetry can be divided between those with genetic origins and those with environmental origins. [8]
The major causes of facial asymmetry have been classified as congenital deformities, developmental asymmetry and acquired facial asymmetry. [9]
Congenital
The genetic malformations during the prenatal period lead to disruption in the growth and development of the cellular processes forming the various craniofacial structures. A number of congenital syndromes have been found to be reported to be associated with varying degrees of facial asymmetry. [10]
A common congenital deformity associated with asymmetry is hemifacial microsomia characterized by unilateral deficiency of the mandible and lower face. Various forms of craniosynostosis such as unicoronal synostosis and plagiocephaly have been found to be associated with mandibular dysmorphologies along with differences in facial measurements between the affected and unaffected sides. Facial clefts and cleft lip/palate deformities are also associated with asymmetry of the facial structures. Variations in intra-uterine pressure and force application during forceps delivery might lead to deformities in the skull and facial region. Congenital torticollis is idiopathic fibrosis of the sternocleidomastoid muscle that restricts movement and pulls the head toward the involved side. Deformation of the craniofacial skeleton will develop if the restriction is not released and result in esthetic and functional problems.
Developmental
This form of facial asymmetry is most commonly observed in the general population. It is the idiopathic, non-syndromic form of asymmetry that gradually develops over the years after birth and might become prominent during the adolescent period.
A possible cause of such a deformity may unilateral chew or other postural habits in the affected groups be unliateral chewing, which might lead to greater skeletal development on one-half of the face. [11]
Acquired
Such facial asymmetries have a known cause and develop post natal. The various causes of an acquired facial asymmetry are Primary condylar hyperplasia, hemifacial atrophy (Romberg syndrome), temporomandibular joint ankylosis, facial trauma and facial tumors.
Classification of Facial Asymmetry
Based on the structures involved facial asymmetry has been classified by into four major categories as skeletal, dental, muscular, and functional asymmetries.
Skeletal
The skeletal facial asymmetry involves one or more bones of the craniofacial region.
The skeletal asymmetry as a result of mandible has been classified by Obwegeser and Makek [12] into two categories:
Hemimandibular hyperplasia: Half of the entire mandible enlarged three-dimensionally leading to increased distances from tooth apices to lower border of the mandible. Since there is an increase in height of the hemi mandible there is, usually, no shifting of the chin point.
Hemimandibular elongation: It is characterized by elongation of either condyle or the ramus in the vertical plane or the mandibular body in the horizontal plane or combinations of both. Elongation of the hemi-mandible leads to shifting of chin toward the opposite side.
Dental
Dental asymmetry is associated with disproportion in the distribution of teeth along the arch. The various reasons for such mal-alignment of teeth are premature loss of deciduous teeth, congenitally missing teeth, presence of supernumerary teeth and tooth size asymmetries.
Muscular
Such asymmetries may result due to an abnormal muscle structure or activity on one side of the face. Often subjects may be associated with hypertrophy of the masseter on one side of the face giving the appearance of facial asymmetry.
Functional Asymmetry
A functional asymmetry occurs as a result of functional deviation of mandible in response to occlusal prematurities. Such cases include presence of constricted arches or unilateral posterior crossbites. Often a single malposed tooth may result in shifting of mandible during closure from centric relation to centric occlusion.
Diagnosis of Facial Asymmetry
Medical history
A thorough medical history of the patient would aid in diagnosing the exact cause of the asymmetry. The patient should be asked for any prolonged illness or infections during childhood. Any history of trauma to the craniofacial region should be noted.
Dental history
The necessary information regarding any trauma to the dentition, history of previous extractions, caries, premature loss of teeth or presence of supernumerary teeth should be recorded.
| Clinical Examination | | |
Extra-oral Examination
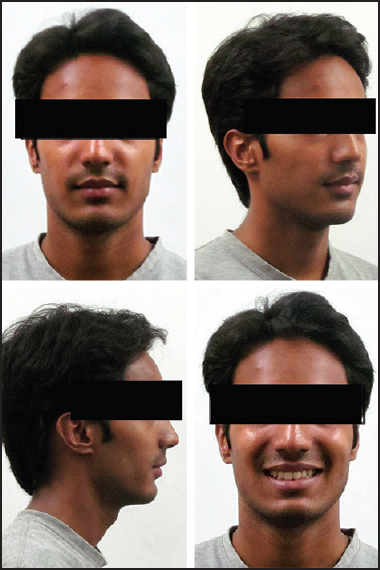
Frontal evaluation
The patient should be evaluated from the frontal view. A gross evaluation of the facial proportions can be done by dividing the face into equal fifths (Farkas and Munro 1980). [13]
Along with this an inspection of symmetry between the bilateral gonial angles should be made.
The lower border of the body of the mandible should also be assessed for bilateral symmetry [Figure 1].
Evaluation of facial and dental midline
The midline of the face should pass through the point between the eyebrows, the dorsum and tip of the nose, the philtrum and the chin point. Facial midline can be assessed by extending a wire from the forehead to the chin.
The dental midline should coincide within both the arches and with the facial midline. The evaluation of the concordance between the midlines should be made in various positions of the mandible such as mouth open, centric relation, initial contact and in centric relation. A true facial asymmetry due to a skeletal cause maintains the same relation both in centric relation and centric occlusion [Figure 2]. [14]
Evaluation of the vertical relations
The cant of both the maxillary and mandibular planes should be evaluated. The patient is made to bite on a tongue blade and is assessed for a parallelism with the interpupillary plane. The threshold for recognizing an occlusal cant is 4° between the plane of occlusion and the inter-pupillary line. [15] The patient should also be evaluated for the amount of gingival display on both sides of the midline as the patient is made to smile [Figure 3].
Evaluation of the transverse relations
The chin point is compared with the lower dental midline indicating the shift of the mandible leading to asymmetry. Furthermore, the patient is made to recline the head backwards, and the lower borders of the mandibular body are evaluated from an inferior view.
Functional evaluation
The patient is made to perform the various functional movements such as opening of the mouth, protrusive movements and the lateral movements of the mandible and any imbalance between the two sides is recorded.
A note of the maximum inter-incisal opening is made along with the inter-occlusal gap. Temporomandibular joint evaluation is done to check any symptoms of clicking, popping or tenderness to rule out any temporomandibular joint dysfunction disorder.
An accurate registration of the centric relation must be made. The use of diagnostic splints has been recommended by Joondeph, [16] to deprogram the muscle memory and correct recording of the centric relation.
Diagnostic Records
Photographic assessment
The routine frontal-relaxed and smiling, profile view and oblique view photographs of the patient are taken. The photographs are assessed for any gross asymmetry between the two sides of the face.
An asymmetry analysis by digitizing standard photographs was proposed by Edler et al. [17] in 2002. The four ratios to be measured are the area (relative size of right and left mandibular segments), perimeter or length of outlines, compactness (shape), and moment on each side of lower half of the face to assess the asymmetry [Figure 4].
Stereophotogrammety - The three-dimensional photograph
The three-dimensional photographic imaging can act as an aid in evaluating the degree of asymmetry between the two sides of the face. Stereophotogrammetry uses two or more cameras, configured as a stereopair to generate a three-dimensional image of the face. This provides a useful three-dimensional assessment of facial soft tissue asymmetry before and after orthognathic surgery. The images can be used for comparison and quantitative measurement.
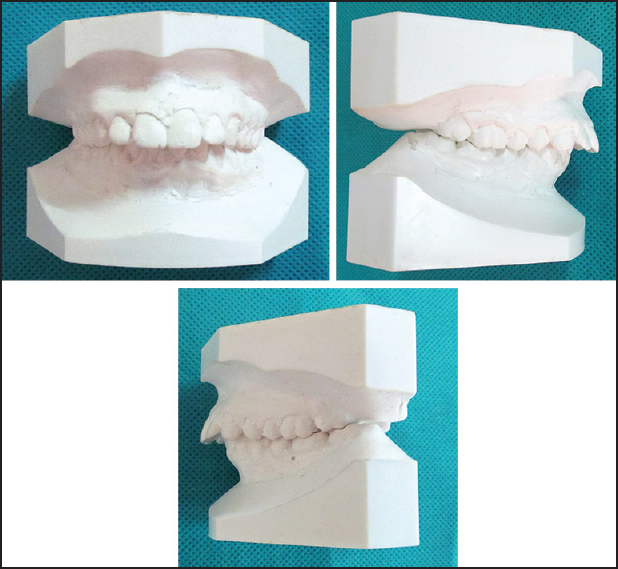
Study models
The articulated study models give a comprehensive three-dimensional view of dental relations. An examination of each dental arch and quadrant can be done by the oriented dental casts. Bilateral symmetry can be established by using oriented occlusograms on the dental casts. The study models can be used to assess the presence of constricted arches and crossbites, which might be the cause of functional asymmetry in the patient. Three-dimensional models can be assessed for various parameters using software to indicate the position of dental asymmetry. Characteristic dental anomalies have been reported in the facial asymmetry group, including asymmetry of the curve of Spee, molar inclination, dental arch form, lateral overjet, and slanting of the occlusal plane [Figure 5]. [18]
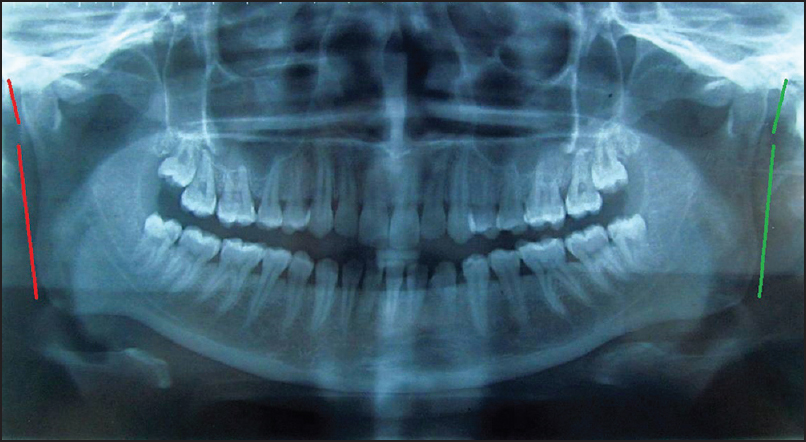
Orthopantomogram
A panoramic radiograph gives the details of the mandibular ramus and body along with the entire dentition.
An analysis to calculate the asymmetry index based on the values of ramus height and the condylar height was proposed by Habets et al. [19] This index helps in the assessment of the morphological asymmetry between the two sides of the mandible. The limitations of an orthopantomographic analysis are that such radiographs are prone to distortion thus might give an impression of false asymmetry between the two sides [Figure 6].
Lateral cephalogram
The lateral cephalogram, usually, suggests an antero-posterior or vertical discrepancy and cannot be used to assess a transverse discrepancy. Although, such radiographs might prove to be useful in cases of hemimandibular hyperplasia where there is no overlapping of the two sides of the mandible.
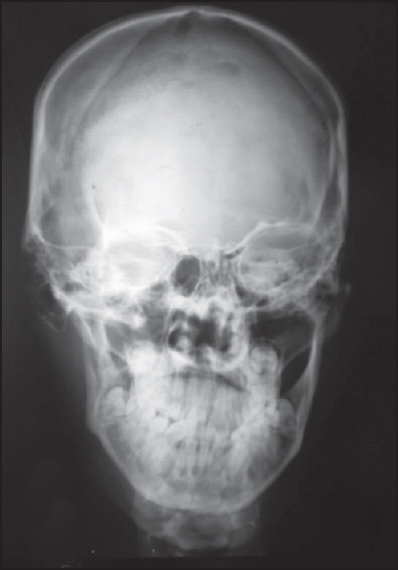
Postero-anterior cephalogram
The postero-anterior view gives an assessment between the transverse dimensions of the skeletal and dental structures. Three basic approaches for a postero-anterior analysis have been proposed anatomic approach, triangulation approach and bisection approach. Hwang et al. [20] measured variables in the postero-anterior radiograph of patients and classified them into five major groups on the basis of three major parameters-Menton deviation, apical base midline discrepancy, vertical difference of ante-gonial notch between the right and left sides. According to Trpkova [21] lines constructed as perpendiculars through midpoints between pairs of orbital landmarks showed excellent validity for measuring asymmetry using posteroanterior cephalogram. Crista galli-anterior nasal spine and nasion-anterior nasal spine have low validity and should not be used in cephalometric analysis of asymmetries. A posteroanterior cephalometric radiograph is a more valuable diagnostic tool when it is exposed with no head rotation to minimize the projection errors [Figure 7].
Submento-vertex radiograph
The coordinates of the submental radiographic view were proposed by Ritucci and Burnstone. The analysis of a submento-vertex radiograph was suggested by Forsberg et al. (1984). [22] This analysis helps an investigator in calculation of asymmetry on the cranial base, zygomatic complex and mandible.
Cone beam computed tomography - The three-dimensional radiography
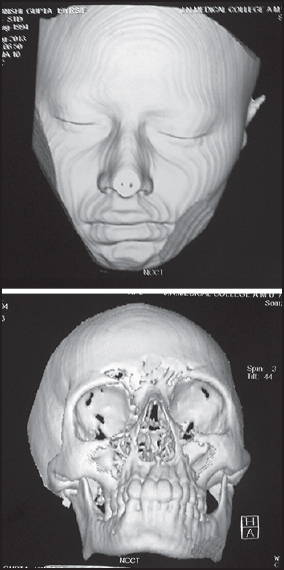
Cone beam computed tomography (CBCT) images can be used to localize the exact position of the skeletal asymmetry. CBCT images have been measured for the following parameters to localize facial asymmetry.
- Maxillary height
- Ramus length,
- Ramal inclination from a frontal view,
- Ramal inclination from a lateral view,
- Mandibular body length, and
- Mandibular body height.
The assessment of all the above variables helps a clinician to locate the site of disproportion and consequently plan for the correction [Figure 8]. [21]
Single positron emission computed tomography
Single positron emission computed tomography is an essential diagnostic tool for visualizing hyperactivity in condyle. The radioactive isotope technetium 99 methylene bisphosphonate is injected into the patient and evaluated on a computed tomogram for signs of increased unilateral condylar activity in the form of hot spots. The difference in activity of 10% or more between the two condyles is indicative of condylar hyperplasia. [23]
Management of Facial Asymmetries
The management of facial asymmetry includes a dentoalveolar movement if compensation is feasible, functional orthopedics if the patient is actively growing and it is anticipated that further growth will be symmetric or orthognathic surgery if the underlying skeletal discrepancy is severe and/or the patient is no longer growing.
Correcting the Functional Asymmetry
Functional shifting of the mandible can be corrected by eliminating the occlusal interferences. Occlusal splint may be given to the patients to localize the occlusal high spots, and the correction would involve minor occlusal adjustments such as grinding of the teeth. Orthodontic intervention can be done by expanding the constricted maxillary arches, either unilateral or bilateral which might be responsible for the mandibular deviation.
Correcting the Dental Asymmetry
Deviations in the position of teeth can be corrected by orthodontic tooth movements. Such treatment procedures involve the application of asymmetric mechanics such as asymmetric extractions, asymmetric elastics, cross elastics, asymmetric lacebacks, unilateral fixed functional appliances, use of miniscrew based mechanics. Use of asymmetric elastics is often associated with certain side effects such as canting of the occlusal plane. Use of unilateral fixed functional appliances may result in unilateral open bite and an occlusal cant. [24]
Managing the Skeletal Asymmetry
Hybrid functional appliances
In a growing individual skeletal asymmetry correction can be attempted by using hybrid functional appliances which act by components causing eruption of teeth (biteplanes), altering the linguofacial muscle balance and mandibular repositioning through construction bites. Such appliances allow selective dento-alveolar eruption and encourage normal mandibular growth to compensate for asymmetrical deficiencies. [25]
Surgical management
In adult patients, minor skeletal asymmetries may be managed by orthodontic corrections but major asymmetries require surgical intervention. Tseng et al. (2013) [26] evaluated 30 surgical and 30 non-surgical cases using six criteria and suggested that four out of these six variables must be fulfilled for a surgical treatment plan. The six criteria were mandibular shift angle ≥ 4.1°, < Ra-Me-ANS ≥ 3.40°, < Zy-Me-ANS ≥ 5.30°, < GWSO-Me-ANS ≥ 4.90°, < J-Me-ANS ≥ 2.10° and Go(ver)-M-ANS ratio ≥ 1.11.
Presurgical orthodontics
Orthognathic surgeries are, usually, preceded by pre-surgical orthodontics that involves relief of crowding and alignment of the dental arches. Decompensation to unmask true extent of skeletal discrepancy involves corrections of the axial inclinations of maxillary and mandibular dentition and the transverse occlusal plane canting. No attempt should be made to correct the dental midlines at this stage as the correction will occur mostly with surgical movements. Mandibular dental midline should be made coincident with midline of the chin, allowing correction with asymmetric mandibular repositioning at surgery.
Two-jaw surgery
The various orthognathic surgical procedures, which are routinely used are bone grafting, maxillary impaction using Le fort I maxillary osteotomy and intra-oral vertical ramus osteotomies for mandibular corrections. Most of the skeletal asymmetries require two-jaw surgeries for complete correction. Surgical planning of two-jaw orthognathic surgery requires three-dimensional consideration in the sagittal, coronal and horizontal planes. Ideally, the dental midline and skeletal midline are aligned to the facial midline. The intercommissural plane should be parallel to the inter exocanthal plane. [27]
Orthognathic surgeries are often supplemented with additional surgical procedures involving bone contouring such as mandibular angle reduction, mandibular inferior border ostectomy, bony augmentation and soft tissue contouring such as buccal fat pad reduction, masseter muscle reduction, fat graft injection and subcutaneous liposuction.
Distraction osteogenesis
Multiplanar distraction osteogenesis can be used to correct mandibular hypoplasia. The treatment planning using distraction osteogenesis involves osteotomy, distraction device placement, vector planning and selection of a distractor. McCarthy et al. [28] reported that only a single osteotomy and two pin sites are required for mandibular distraction. Distraction for lengthening mandibular ramus also increases soft tissue by increasing the volume of medial pterygoid muscle.
Genioplasty
The lower border osteotomy (genioplasty) of the mandible can reposition the chin point transversely or vertically in order to address the asymmetry. It is one of the most stable movements compared with managing mandibular asymmetries by other orthognathic movements. It is reported that a minimum of 6 mm between the inferior border of the mental nerve canal and the proximal osteotomy during sliding genioplasty can greatly reduce the chance of inferior alveolar nerve damage, although it does not completely eliminate the risk. Thus, keeping at least 6 mm of space should be a goal during surgery to protect the patient. [29]
| Conclusion | | |
A detailed clinical examination and formulation of the correct diagnosis would help the clinicians achieve the desired treatment goals. Cases of facial asymmetry may be managed by orthodontic or surgical means depending upon the degree of severity and the patient's expectations regarding their treatment. The clinician must be aware of the patient's expectations while treating such cases and evaluate the cost to benefits ratio of the various treatment modalities to achieve the best possible outcomes.
| References | | |
| 1. | Bishara SE, Burkey PS, Kharouf JG. Dental and facial asymmetries: A review. Angle Orthod 1994;64:89-98.  |
| 2. | Severt TR, Proffit WR. The prevalence of facial asymmetry in the dentofacial deformities population at the University of North Carolina. Int J Adult Orthodon Orthognath Surg 1997;12:171-6. |
| 3. | Pirttiniemi PM. Associations of mandibular and facial asymmetries - A review. Am J Orthod Dentofacial Orthop 1994;106:191-200. |
| 4. | Peck S, Peck L, Kataja M. Skeletal asymmetry in esthetically pleasing faces. Angle Orthod 1991;61:43-8. |
| 5. | Maeda M, Katsumata A, Ariji Y, Muramatsu A, Yoshida K, Goto S, et al. 3D-CT evaluation of facial asymmetry in patients with maxillofacial deformities. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2006;102:382-90. |
| 6. | Chew MT. Soft and hard tissue changes after bimaxillary surgery in Chinese Class III patients. Angle Orthod 2005;75:959-63. |
| 7. | Sheats RD, McGorray SP, Musmar Q, Wheeler TT, King GJ. Prevalence of orthodontic asymmetries. Semin Orthod 1998;4:138-45. |
| 8. | Haraguchi S, Iguchi Y, Takada K. Asymmetry of the face in orthodontic patients. Angle Orthod 2008;78:421-6. |
| 9. | Sisman Y, Uysal T, Gelgor IE. Hypodontia. Does the prevalence and distribution pattern differ in orthodontic patients? Eur J Dent 2007;1:167-73. |
| 10. | Gelgor IE, Sisman Y, Malkoc S. Prevalence of dimensional anomaly in the permanent dentition. Turkiye Klinikleri J Dent Sci 2005;11:49-53. |
| 11. | Shah SM, Joshi MR. An assessment of asymmetry in the normal craniofacial complex. Angle Orthod 1978;48:141-8. |
| 12. | Obwegeser HL, Makek MS. Hemimandibular hyperplasia - hemimandibular elongation. J Maxillofac Surg 1986;14:183-208. |
| 13. | Farkas LG, Munro IR. Anthropometric Facial Proportions in Medicine. Illinois: Charles C Thomas; 1987. |
| 14. | Nanda R, Margolis MJ. Treatment strategies for midline discrepancies. Semin Orthod 1996;2:84-9. |
| 15. | Padwa BL, Kaiser MO, Kaban LB. Occlusal cant in the frontal plane as a reflection of facial asymmetry. J Oral Maxillofac Surg 1997;55:811-6. |
| 16. | Joondeph DR. Mysteries of asymmetries. Am J Orthod Dentofacial Orthop 2000;117:577-9. |
| 17. | Edler R, Wertheim D, Greenhill D. Outcome measurement in the correction of mandibular asymmetry. Am J Orthod Dentofacial Orthop 2004;125:435-43. |
| 18. | Kusayama M, Motohashi N, Kuroda T. Relationship between transverse dental anomalies and skeletal asymmetry. Am J Orthod Dentofacial Orthop 2003;123:329-37. |
| 19. | Habets LL, Bezuur JN, Naeiji M, Hansson TL. The Orthopantomogram, an aid in diagnosis of temporomandibular joint problems. II. The vertical symmetry. J Oral Rehabil 1988;15:465-71. |
| 20. | Hwang HS, Hwang CH, Lee KH, Kang BC. Maxillofacial 3-dimensional image analysis for the diagnosis of facial asymmetry. Am J Orthod Dentofacial Orthop 2006;130:779-85. |
| 21. | Trpkova B, Prasad NG, Lam EW, Raboud D, Glover KE, Major PW. Assessment of facial asymmetries from posteroanterior cephalograms: Validity of reference lines. Am J Orthod Dentofacial Orthop 2003;123:512-20. |
| 22. | Forsberg CT, Burstone CJ, Hanley KJ. Diagnosis and treatment planning of skeletal asymmetry with the submental-vertical radiograph. Am J Orthod 1984;85:224-37. |
| 23. | Cisneros GJ, Kaban LB . Skeletal scintigraphy. In: Bell WH, editor. Surgical Correction of Dentofacial Deformities . Philadelphia, PA: Saunders; 1985. p. 316-34 . |
| 24. | Burstone CJ. Diagnosis and treatment planning of patients with asymmetries. Semin Orthod 1998;4:153-64. |
| 25. | Vig PS, Vig KW. Hybrid appliances: A component approach to dentofacial orthopedics. Am J Orthod Dentofacial Orthop 1986;90:273-85. |
| 26. | Tseng YC, Yang YH, Pan CY, Chou ST, Ou KC, Chang HP. Treatment of adult facial asymmetry with orthodontic therapy or orthognathic surgery: Receiver operating characteristic analysis. J Dent Sci 2014;9:235-43. |
| 27. | Tai K, Park JH, Ikeda K, Nishiyama A, Sato Y. Severe facial asymmetry and unilateral lingual crossbite treated with orthodontics and 2-jaw surgery: 5-year follow-up. Am J Orthod Dentofacial Orthop 2012;142:509-23. |
| 28. | McCarthy JG, Schreiber J, Karp N, Thorne CH, Grayson BH. Lengthening the human mandible by gradual distraction. Plast Reconstr Surg 1992;89:1-8. |
| 29. | Ousterhout DK. Sliding genioplasty, avoiding mental nerve injuries. J Craniofac Surg 1996;7:297-8. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7], [Figure 8]
|













 Search Pubmed for
Search Pubmed for