|
 
 |
| REVIEW ARTICLE |
|
| Year : 2015 | Volume
: 3
| Issue : 3 | Page : 162-165 |
|
Nickel allergies in orthodontics
Suchita Madhukar Tarvade (Daokar), Sheetal Ramkrishna
Department of Orthodontics, CSMSS Dental College, Aurangabad, Maharashtra, India
| Date of Web Publication | 11-Sep-2015 |
Correspondence Address:
Suchita Madhukar Tarvade (Daokar)
Plot No. 1, Bharatnagar Housing Society, Jyotinagar, Aurangabad, Maharashtra
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.152121

Nickel (Ni) is a common component in many orthodontic materials. An allergy to Ni is commonly seen in the population, more frequently in women. Possible allergy to Ni should be a question in the initial patient health history questionnaire. The orthodontic practitioner should be mindful of this allergy during the course of treatment and know how to diagnose a Ni allergy if it appears and subsequent action in treatment and referral if it is suspected. This paper provides a summary of Ni allergy, its epidemiology, diagnosis and recommendations and alternatives to treatment. Keywords: Allergies, metal ions, nickel ions
How to cite this article:
Tarvade (Daokar) SM, Ramkrishna S. Nickel allergies in orthodontics. J Orthod Res 2015;3:162-5 |
| Introduction | |  |
Almost all fixed metallic orthodontic appliance comprises metals such as nickel (Ni), chromium (cr) and cobalt. [1] Appliances and additional devices used during treatment are exposed to different factors, such as temperatures, pH, mechanical stress, and micro flora. [2] All these factors may lead to release of toxic metal ions from alloy. Various studies have been conducted to show release of metal ions and its toxic effects. [3] These leached out components of orthodontic treatment are well known allergenic, cytotoxic and mutagenic. [3]
| Prevalence | | |
Nickel is the most common causes of allergenic contact dermatitis and produces more allergic reactions than all other metals combined. [4] Both Ni and cr can cause hypersensitivity in some people, especially in women. Hypersensitivity to Ni in females is thought to be related to environmental exposure, as a result of contact with detergents, jewelry, earrings, and other metallic objects. In males, the hypersensitivity is usually related to occupational exposure. [5],[6]
Dietary intakes of Ni have been estimated to be 200-300 μg/day, Ni concentrations in drinking water are generally below 20 μg. Ni content in excess of 50% elicit manifestations of an allergic reaction. [7]
Nickel ion release from orthodontic appliances and its toxic reaction has been a concern to the orthodontist as well as the patients. This article will focus on the release of Ni ions, their action on the tissues, its prevention and care to be taken.
| Studies on Release of Nickel Ions | | |
According to Agaoglu et al., [7] level of Ni in saliva and serum increases significantly after insertion of fixed orthodontic appliances. According to Bengleil et al. [8] there was an increase in ion concentrations after 2 weeks of conventional archwires placement. Barrett et al. [6] and Amini et al. [1] have shown an increase in metal ion concentration in the oral fluid of patients with orthodontic appliances as long as 16 months from start of treatment.
Menezes et al. [9] performed studies at different intervals and concluded, individuals vary with different salivary compositions also vary with release of ion concentrations.
| Biologic Reactions | | |
An allergic response is one in which certain components of the immune system react excessively to a foreign substance. Ni elicits contact dermatitis, which is a type IV delayed hyper sensitivity immune response. [10],[11] This process has two interrelated, distinct phases:
- Sensitization phase - first exposure and,
- Elicitation - re-exposure to allergen.
| Occurrence of Nickel Allergy | | |
Nickel is the most commonly used metals, as it is a component of the super elastic and shape memory wires. [12] Ni is the most common metal to cause contact dermatitis. Kerosuo et al. [13] found prevalence of Ni allergy adolescents to be 30% in girls and 3% boys. Sensitizing patients to Ni through routine orthodontic treatment has been a concern. [13] It has been suggested that a threshold concentration of approximately 30 ppm of Ni may elicit a cytotoxic response. [14] It is believed to be increased by mechanical irritation, skin macerations or oral mucosal injury, all which may occur in orthodontic treatment. [15]
| Diagnosis | | |
The diagnosis of Ni allergy has usually been based on patient history, clinical findings, genetic factors, and the results of patch testing's. [16] In the patch test, 5% Ni sulfate in petroleum jelly is used. Lesions due to mechanical irritation; allergies to other materials such as acrylic should be ruled out. [17]
| Signs and Symptoms | | |
Extra Oral
- Generalized urticaria.
- Wide spread eczema.
- Flare up of allergic dermatitis.
- Exacerbation of preexisting eczema.
Intra Oral
- Stomatitis from mild to severe erythema.
- Papulaperi oral rash.
- Loss of metallic taste.
- Numbness.
- Burning sensation.
- Soreness at side of the tongue.
- Angular chelitis severe gingivitis in the absence of plaque. [12]
| Possible Risks Associated With Nickel Toxicity | | |
The literature has shown many in vivo and in vitro studies documenting the corrosion of orthodontic appliances and the release of metal ions are indisputable. It has been reported that metal ions are taken up by the adjacent oral tissues. [18],[19]
Risk of Nephrotoxicity
Sunderman [17] reported a patient with documented IgA nephropathy.
Risk of Cytotoxicity
Grimsdottir et al. [5] used the agar overlay cytotoxicity test with mouse fibroblast cells and reported that none of the arch wires tested caused by cytotoxic effect whereas the multicomponent devices. The study carried out by Hafez et al.[18] proved the cytotoxicity and genotoxicity of orthodontic appliances remained in the mouth for 6 months.
Risk of Carcinogenicity
Sunderman [17] and Mastromatteo [19] reported that Ni subsulphide, Ni oxide, and metallic Ni dust have been suspected to be the principal respiratory carcinogens.
Risk of DNA Damage
Several studies conducted by Faccioni et al., [20] Hafez et al.[18] and Fernαndez-Miñano et al. [21] suggesting the DNA damage in buccal mucosal cells [22] and Heravi et al. [23] suggested that DNA damage induced by orthodontic appliance would repair in healthy individuals, but decrease in repair capacity or alterations in the immune system may allow the DNA damage to remain and expressed as genome alteration and DNA mutations. Older age, presence of systemic diseases and risk factors such as tobacco smoke may also aggravate the harmful effects of fixed appliances. [23]
Study by Das et al. [24] shown Ni ion leaching from appliances can also generate free radicals resulting in oxidative stress in cell and tissue level.
Risk of Immune Changes and Alveolar Bone Loss
Lamster et al. [25] reviewed two cases of women who demonstrated significant alveolar bone loss around Ni-rich nonprecious alloy and porcelain crown. A type IV hypersensitivity reaction was observed which may have caused the loss of the alveolar bone.
Risk of Sensitivity
Nickel dermatitis could be seen of two types. First type of dermatitis is described as a reaction on the skin characterized by itching or burning, popularly seen as erythemas in the web of the fingers, which would spread to the fingers, wrist, and forearms. A second type of Ni dermatitis was described as papulo-vesicular dermatitis with a tendency for lichenification. [11]
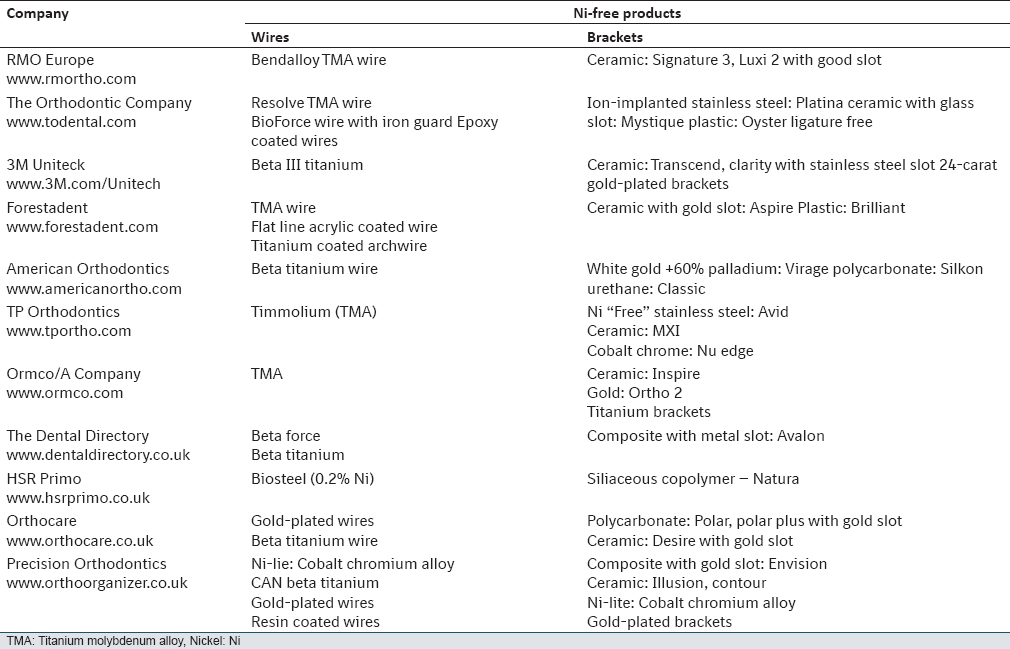
Alternate Treatment Modalities
Nickel free appliances are available to prevent an allergic reaction and toxic effects in orthodontic treatment various [Table 1]. [12]
| Conclusion | | |
In recent decades, there has been greater importance of biocompatibility of orthodontic appliances due its harmful effects. The frequency of orthodontic treatment and common use of Ni containing orthodontic material may act to increase or decrease the burden of Ni hypersensitivity in the population. There is evidence that oral exposure to Ni may induce immunologic tolerance to Ni and thereby reduce the incidence of Ni allergies. It's also seen that damage caused by Ni ions repair in healthy individuals over period of time. Nevertheless when clinical signs or symptoms presumed to be due to Ni hypersensitivity are distressing to patients there are many choices of materials available to the orthodontist as alternatives and should be thought about. Along with orthodontic care, general wellbeing of the patient should be prime motto and steps should be taken to achieve it whenever needed.
| References | | |
| 1. | Amini F, Borzabadi Farahani A, Jafari A, Rabbani M. In vivo study of metal content of oral mucosa cells in patients with and without fixed orthodontic appliances. Orthod Craniofac Res 2008;11:51-6.  |
| 2. | Mikulewicz M, Chojnacka K, Wozniak B, Downarowicz P. Release of metal ions from orthodontic appliances: An in vitro study. Biol Trace Elem Res 2012;146:272-80. |
| 3. | Eliades T, Athanasiou AE. In vivo aging of orthodontic alloys: Implications for corrosion potential, nickel release, and biocompatibility. Angle Orthod 2002;72:222-37. |
| 4. | Staerkjaer L, Menné T. Nickel allergy and orthodontic treatment. Eur J Orthod 1990;12:284-9. |
| 5. | Grimsdottir MR, Gjerdet NR, Hensten-Pettersen A. Composition and in vitro corrosion of orthodontic appliances. Am J Orthod Dentofacial Orthop 1992;101:525-32. |
| 6. | Barrett RD, Bishara SE, Quinn JK. Biodegradation of orthodontic appliances. Part I. Biodegradation of nickel and chromium in vitro. Am J Orthod Dentofacial Orthop 1993;103:8-14. |
| 7. | Agaoglu G, Arun T, Izgi B, Yarat A. Nickel and chromium levels in the saliva and serum of patients with fixed orthodontic appliances. Angle Orthod 2001;71:375-9. |
| 8. | Bengleil MS, Orfi JM, Abdelgader I. Evaluation of salivary nickel level during orthodontic treatment. Int J Med Pharm Sci Eng 2013;7:668-70. |
| 9. | Menezes LM, Campos LC, Quintão CC, Bolognese AM. Hypersensitivity to metals in orthodontics. Am J Orthod Dentofacial Orthop 2004;126:58-64. |
| 10. | Van Loon LA, van Elsas PW, Bos JD, ten Harkel-Hagenaar HC, Krieg SR, Davidson CL. T-lymphocyte and Langerhans cell distribution in normal and allergically induced oral mucosa in contact with nickel-containing dental alloys. J Oral Pathol 1988;17:129-37. |
| 11. | Agarwal P, Upadhyay U, Tandon R, Kumar S. Nickel allergy and orthodontics. AJOHAS 2011;1:61-3. |
| 12. | Rahilly G, Price N. Current products and practice nickel allergy and orthodontics. J Orthod 2003;30:171-4. |
| 13. | Kerosuo H, Kullaa A, Kerosuo E, Kanerva L, Hensten-Pettersen A. Nickel allergy in adolescents in relation to orthodontic treatment and piercing of ears. Am J Orthod Dentofacial Orthop 1996;109:148-54. |
| 14. | Bass JK, Fine H, Cisneros GJ. Nickel hypersensitivity in the orthodontic patient. Am J Orthod Dentofacial Orthop 1993;103:280-5. |
| 15. | Bour H, Nicholas JF, Garrigue JL, Demidem A, Schmitt D. Establishment of nickel specific T cell lines from patients with allergic contact dermatitis comparisons of three different protocol. Clin Immunopathol 1994;73:142-5. |
| 16. | Marigo M, Nouer DF, Genelhu MC, Malaquias LC, Pizziolo VR, Costa AS, et al. Evaluation of immunologic profile in patients with nickel sensitivity due to use of fixed orthodontic appliances. Am J Orthod Dentofacial Orthop 2003;124:46-52. |
| 17. | Sunderman FW. Metal carcinogenesis advances in modern toxicology. Toxicology of Trace Elements. Vol. 2. New York: Halsted Press; 1977. p. 257-95. |
| 18. | Hafez HS, Selim EM, Kamel Eid FH, Tawfik WA, Al-Ashkar EA, Mostafa YA. Cytotoxicity, genotoxicity, and metal release in patients with fixed orthodontic appliances: A longitudinal in-vivo study. Am J Orthod Dentofacial Orthop 2011;140:298-308. |
| 19. | Mastromatteo E. Yant memorial lecture. Nickel. Am Ind Hyg Assoc J 1986;47:589-601. |
| 20. | Faccioni F, Franceschetti P, Cerpelloni M, Fracasso ME. In vivo study on metal release from fixed orthodontic appliances and DNA damage in oral mucosa cells. Am J Orthod Dentofacial Orthop 2003;124:687-93. |
| 21. | Fernández-Miñano E, Ortiz C, Vicente A, Calvo JL, Ortiz AJ. Metallic ion content and damage to the DNA in oral mucosa cells of children with fixed orthodontic appliances. Biometals 2011;24:935-41. |
| 22. | Pereira BR, Tanaka OM, Lima AA, Guariza-Filho O, Maruo H, Camargo ES. Metal and ceramic bracket effects on human buccal mucosa epithelial cells. Angle Orthod 2009;79:373-9. |
| 23. | Heravi F, Abbaszadegan MR, Merati M, Hasanzadeh N, Dadkhah E, Ahrari F. DNA damage in oral mucosa cells of patients with fixed orthodontic appliances. J Dent (Tehran) 2013;10:494-500. |
| 24. | Das KK, Das SN, Dhundasi SA. Nickel, its adverse health effects & oxidative stress. Indian J Med Res 2008;128:412-25. [ PUBMED]  |
| 25. | Lamster IB, Kalfus DI, Steigerwald PJ, Chasens AI. Rapid loss of alveolar bone associated with nonprecious alloy crowns in two patients with nickel hypersensitivity. J Periodontol 1987;58:486-92. |
[Table 1]
|










 Search Pubmed for
Search Pubmed for