|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 3
| Issue : 3 | Page : 175-180 |
|
Overjet as a predictor of vertical facial morphology in orthodontic patients with class II division 1 malocclusion
Nita Kumari Bhateja, Mubassar Fida, Attiya Shaikh
Department of Surgery, Section of Dentistry, The Aga Khan University Hospital, Karachi 74800, Pakistan
| Date of Web Publication | 11-Sep-2015 |
Correspondence Address:
Nita Kumari Bhateja
Department of Surgery, Section of Dentistry, The Aga Khan University Hospital, P.O. Box 3500, Stadium Road, Karachi 74800
Pakistan
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.158137

Objective: To evaluate the vertical facial morphology in untreated orthodontic patients with Class II division 1 malocclusion. Materials and Methods: The sample comprised of 113 patients (61 females and 52 males) between 8 and 13 years of age, having Class II malocclusion with overjet of >4 mm, no prior history of orthodontic treatment, no craniofacial anomalies and no missing first permanent molars. Skeletal parameters were assessed using pretreatment lateral cephalograms of these patients. Overjet was measured on the study casts, using digital vernier caliper. Descriptive statistics was calculated for age and different vertical facial cephalometric angles. Pearson's correlation was used to correlate various parameters. One-way analysis of variance was used for comparison of means of vertical facial cephalometric angles among three overjet groups (Group I = 5-7 mm, Group II =8-10 mm, Group III = >10 mm). Results: The means of all vertical facial cephalometric parameters were in the normal range representing average facial pattern in patients with Class II division 1 malocclusion, except Jarabak ratio which indicated a tendency toward long facial pattern. No statistically significant correlation was found between overjet and parameters of vertical facial morphology. Frankfort mandibular plane angle was found to have a moderately significant positive correlation with Steiner's mandibular plane angle (r = 0.789**) and Y-axis (r = 0.604**). Conclusion: Patients with Class II division 1 malocclusion have an average vertical growth pattern, Overjet value is not a predictor of vertical facial morphology, There is no significant correlation between overjet and parameters used to assess vertical facial morphology. Keywords: Class II malocclusion, overjet, vertical facial morphology
How to cite this article:
Bhateja NK, Fida M, Shaikh A. Overjet as a predictor of vertical facial morphology in orthodontic patients with class II division 1 malocclusion. J Orthod Res 2015;3:175-80 |
How to cite this URL:
Bhateja NK, Fida M, Shaikh A. Overjet as a predictor of vertical facial morphology in orthodontic patients with class II division 1 malocclusion. J Orthod Res [serial online] 2015 [cited 2018 Sep 6];3:175-80. Available from: http://www.jorthodr.org/text.asp?2015/3/3/175/158137 |
| Introduction | |  |
Orthodontic treatment of malocclusion has three major goals; improvement of smile and facial esthetics with resultant improvement in the individual's social well-being and the quality of life, establishment of normal occlusion and function in order to attain optimal functional efficiency, and stability of the results which are attained at the termination of the orthodontic treatment by positioning the teeth within the physiological limits.
Accomplishment of orthodontic goals is mainly reliant on the appropriate diagnosis and treatment planning. In every medical field, treatment plan is the road map that is followed by the patient on his journey throughout the treatment. The best treatment plan is the one that has minimum relapse and maximum stability. Likewise, in orthodontics, accurate diagnosis and precise appreciation of underlying etiological components will aid in understanding of the condition, prevention, early prediction, and eventually in optimal treatment outcomes.
Malocclusion is defined as an occlusion in which there is an atypical relationship, or there are aberrations in tooth position beyond normal limits. [1] Patients with malocclusion can be presented with a problem in skeletal components in vertical and sagittal dimensions. In vertical dimensions, jaw relationship may have normodivergent, hyperdivergent, and hypodivergent facial patterns depending on the position of skeletal base, demonstrating normal, long and short faces, respectively. [2] Similarly in the sagittal plane, the jaw relationship can either be Class I, II, and III depending on the relative positions of upper and lower jaws. [3] Angle [4] classified malocclusion in three classes depending on the relation of the upper and lower first permanent molars in the sagittal plane. In Class II malocclusion, the mesiobuccal cusp of the upper first permanent molar occludes mesial to the mesiobuccal groove of lower first permanent molar. Class II is further subdivided into two divisions: Class II division 1 (II/1) with maxillary incisors being protrusive resulting in increased overjet and Class II division 2 with maxillary incisors being retrusive resulting in decreased overjet. Overjet is the linear distance, measured from the labial surface of mandibular central incisor to the labial surface of most prominent maxillary incisor, and its normal value is 3-4 mm. [4] A local study conducted in Pakistan on hospital patients showed that 70.5% patients had Angle's Class II and among them 64.7% had Class II/1, and 75% had increased overjet. [5] Being so frequently seen disharmony, this is one of the chief concerns for an orthodontist. Moreover, according to the index of orthodontic treatment need, increased overjet of >6 mm is considered as a severe problem definitely needing treatment in orthodontic practice. [6]
Class II/1 malocclusion is a clinical manifestation of various skeletal and dental discrepancies having multifactorial etiology. [4],[7],[8] Untreated Class II/1 malocclusion can cause introversion, withdrawal from the society, self-consciousness, increased incidence of dental trauma resulting in fractures and avulsions. [9] When associated with deep bite and posterior crossbites, it may be a contributing factor of temporomandibular joint disorders. [10] Therefore, correction of Class II/1 malocclusion is crucial for maintenance of normal health of oral hard- and soft-tissue structures.
This is the established fact in the literature that overjet is a good predictor of sagittal relationship, [11] but recent studies [12],[13] have reported that overjet is also a good predictor of vertical facial morphology. They reported a positive association between increased overjet and the tendency toward long facial morphology. If this is true than patients presenting with increased overjet in growing age, should be treated with high pull headgear which restricts the forward and vertical growth of maxilla along with facilitating the upward and forward rotation of mandible. It helps in reduction of overjet and lower anterior facial height. When combined with the functional appliance, it has a synergistic effect and promotes the growth of mandible in an anterior direction and facilitates in the reduction of overjet. If patients having problem in sagittal dimension as well as in the vertical dimension present after the completion of growth, they can only be treated with invasive procedures such as mini-implant placement and orthognathic surgery. Hence, the aim of current study was to evaluate vertical facial morphology in untreated Class II/1 patients in a sample of the Pakistani population. If these patients have increase in mean vertical facial cephalometric parameters, early treatment that controls the amount and direction of mandibular growth to prevent the excessive increase in vertical facial height, by using growth modification appliances could be ideal for them.
| Materials and Methods | | |
A cross-sectional study was conducted using the data from pretreatment orthodontic records of patients who visited the orthodontic clinics at the Aga Khan University Hospital, Karachi, Pakistan. Ethical clearance was obtained from the Institutional Ethical Review Committee (ERC No. 2928-Sur-ERC-13) prior to data collection. The duration of this study was from January 2014 to June 2014. The present study primarily focused on orthodontic patients with Class II/1 malocclusion. The inclusion criteria were subjects of Pakistani origin having Class II/1 malocclusion with the overjet of >4 mm and age range of 8-13 years with no history of previous orthodontic treatment were included in the study. Patients with craniofacial anomalies and missing first permanent molars were excluded. A nonprobability purposive sampling technique was used. By taking the prevalence of increased overjet in Class II malocclusion patients is 66.3%, [5] margin of error 9%, confidence level of 95%, the sample size comes out to be at least 113 patients to meet the objectives of the study.
Data were collected from the standard pretreatment lateral cephalograms at the Orthodontic Clinics, the Aga Khan University Hospital. These lateral cephalograms were recorded with rigid head fixation and a 165-cm film-to-tube distance using Orthoralix® 9200 (Gendex-KaVo, Milan, Italy). The following measures were taken for each subject to ensure a high degree of precision in obtaining cephalograms: The head was fixed in a way that the sagittal plane was at a right angle to the path of the X-rays and the Frankfort horizontal plane was parallel to the horizontal plane; teeth were occluded in the centric occlusion and lips were maintained in a relaxed position.
A detailed clinical examination of the patients was carried out by the orthodontists at the time of initial assessment. Complete medical and dental history along with the findings of extra and intra oral examination of the patients were noted in their pretreatment file. Patients were inquired about their previous extractions and orthodontic treatment. Extra orally their anteroposterior, vertical and transverse skeletal pattern was assessed. Thorough examination of the soft tissues, rest position of the mandible, centric occlusion-centric relation discrepancy, and presence of para-functional habits was performed. Intra orally, complete evaluation of the oral hygiene, gingival condition, status of the present teeth, upper and lower incisor inclinations with respect to the jaw base, presence of crowding, spacing, rotations, displacements, overjet, overbite, midlines, incisor, canine, and molar relationships was done.
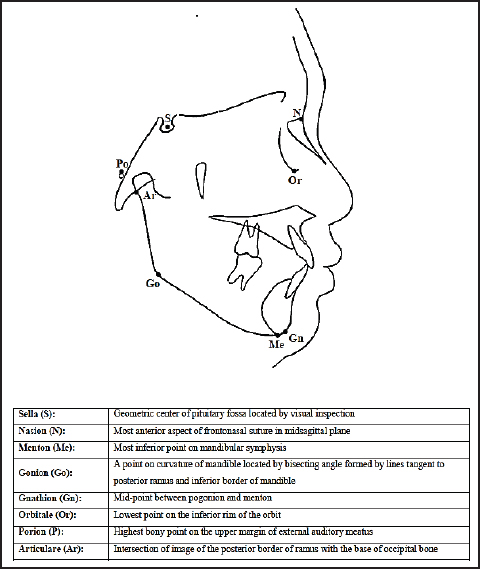
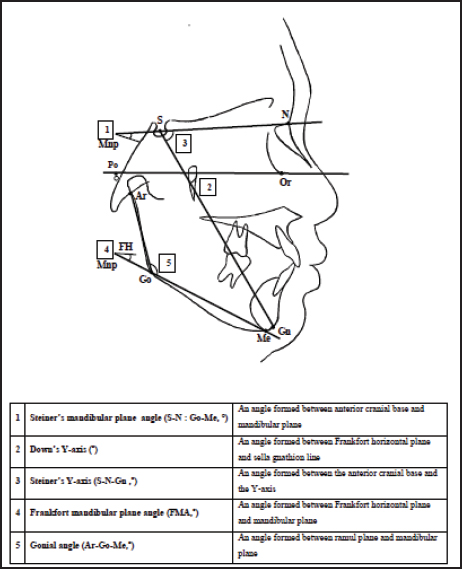
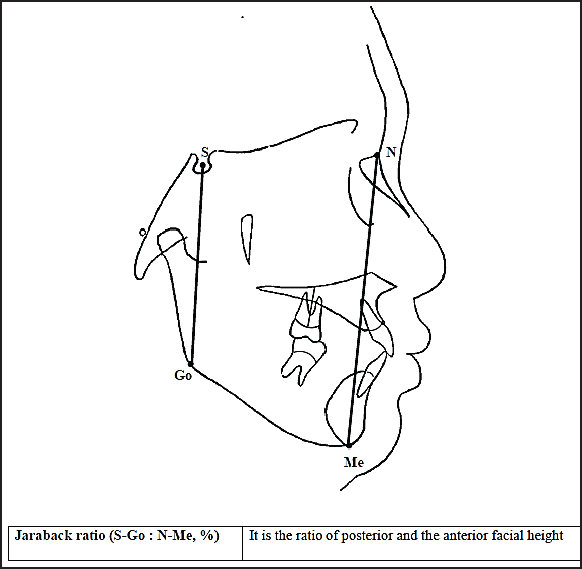
Cephalograms were traced manually by the principal investigator on acetate paper in a dark room. The linear and angular measurements were taken with the help of a millimeter ruler and protractor, respectively. Cephalometric landmarks were marked [Figure 1], and cephalometric parameters were measured [Figure 2] and [Figure 3]. [14] The values for mean and SD for four outcome variables (S-N:Go-Me°, N-S-Gn (Y)°, S-Go:N-Me°, Ar-Go-Me°) were taken from the study conducted by Saltaji et al.[12]
Overjet was measured on study casts taken from each subject, with a digital vernier caliper (0-150 mm ME00183, Dentaurum, Pforzheim, Germany) with accuracy of 0.02 mm and reliability of 0.01 mm manufacturer's specification.
Statistics
The statistical analysis of data was done using the SPSS for Windows (version 19.0, SPSS Inc., Chicago, IL, USA). Descriptive statistics was calculated for age and different vertical facial cephalometric angles of Class II/1 patients. Pearson's correlation was used to correlate various parameters. Stratification with respect to age and gender was done to see the influence of these on outcome variables. One-way analysis of variance (ANOVA) was used for comparison of means of vertical facial cephalometric angles among the three overjet groups (Group I = 5-7 mm, Group II =8-10 mm, Group III = >10 mm). A P ≤ 0.05 was taken as statistically significant.
| Results | | |
The sample size consisted of 113 subjects (52 males and 61 females). The mean age for the female subjects was 11.61 ± 1.36 years and for the male subjects was 11.73 ± 1.22 years.
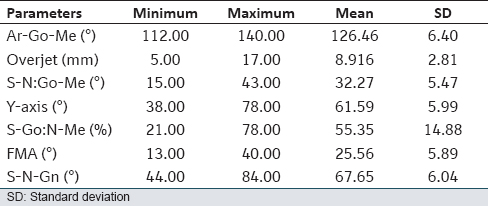
The key results of this cross-sectional study showed that the means of all the vertical facial cephalometric parameters were in the normal range representing average facial pattern in patients with Class II/1 malocclusion, except the Jarabak ratio that indicated tendency toward long facial pattern. Moreover, no statistically significant correlation was found between the overjet and the parameters of vertical facial morphology. Frankfort mandibular plane angle was found to have a moderately significant positive correlation with Steiner's mandibular plane angle (r = 0.789**) and Y-axis (r = 0.604**).
[Table 1] shows the descriptive statistics of the study parameters. Mean values of all the study parameters demonstrating the vertical facial morphology were in the normal range but the Jarabak ratio that indicated predisposition to long facial pattern.
Pearson correlation coefficient was used to investigate correlations between various study parameters as shown in [Table 2]. There was no statistically significant correlation between overjet and the parameters used for assessment of vertical facial morphology. Steiner's mandibular plan angle was found to have weak positive correlation with Steiner's Y-axis (r = 0.492**), Down's Y-axis (r = 0.492**) and gonial angle (r = 0.536**). Likewise, there was moderately positive correlation between the Steiner's mandibular plan angle and the Frankfort mandibular plane angle (r = 0.789**). Down's Y-axis was found to have a weak positive correlation with Frankfort mandibular plane angle (r = 0.604**) and strong positive correlation with Steiner's Y-axis (r = 0.998**). Furthermore, Jarabak ratio showed weak negative correlation with the gonial angle (r = −0.220*), Frankfort mandibular plane angle (r = −0.142) and Steiner's Y-axis (r = −0.182).
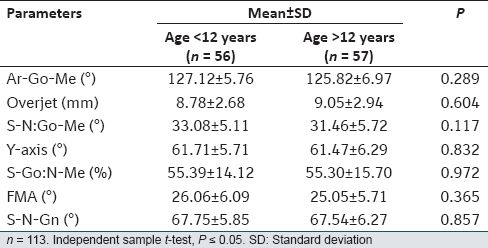
In order to see the influence of age on various study parameters, the entire sample was divided into two groups (Group I = <12 years, Group II = >12 years) as shown in [Table 3]. No statistically significant difference was found in the means of all the study parameters among groups.
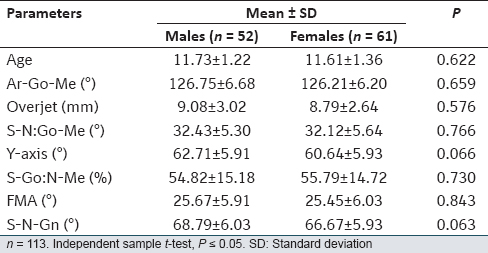
To evaluate the effect of gender on several study parameters, the whole sample was distributed in two groups (Group I = 52 males, Group II = 61 females) as shown in [Table 4]. No statistically significant difference was found in the means of all the study parameters among groups.
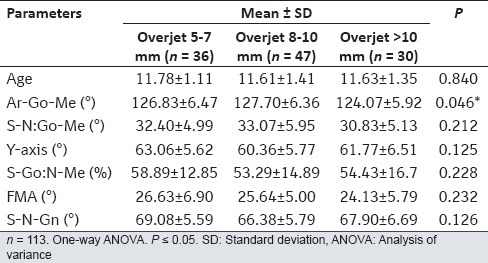
One-way ANOVA was used to determine the differences among three overjet groups (Group I = 5-7 mm, Group II = 8-10 mm, Group III = >10 mm) as displayed in [Table 5]. Only statistically significant difference was found in gonial angle (P = 0.046*).
| Discussion | | |
Various diagnostic records are acquired to determine the ideal treatment plan. The diagnostic database comprises patient's history, clinical examination, study cast analysis, cephalometric analysis, and facial photographs. [9]
Overjet is an important measure in the study cast analysis. It is one of the parameters used to evaluate the sagittal relationship. In adolescents beyond the growth spurt, when deciding on surgical or orthodontic intervention, besides the facial profile, overjet is an essential guideline. Usually, when the overjet is >10 mm, surgery is a more successful treatment option. [9]
However, overjet is not always a reliable measure of the jaw relationship in the sagittal plane, especially in subjects with Class III malocclusions. [15] For the precise determination of jaw relationship, cephalometric analysis is essential because two malocclusions can appear alike when observing just study casts but careful cephalometric analysis can show that the basic problem is very different.
Radiographic analysis not only assists in the diagnosis of malocclusions but can also influence the treatment plan. It has been shown that especially when extractions are involved, cephalometric data significantly influence the course of treatment. [16] Hence, this study was designed to appreciate the correlation between skeletal cephalometric parameters of vertical facial morphology and the overjet value.
Saltaji et al.[13] conducted a study to examine the extent to which vertical facial morphology and the sagittal relationship determined by overjet, Wits appraisal, and ANB angle are interrelated in patients with skeletal and dental Class II malocclusion. They found that sagittal relationship, determined by overjet is a moderate predictor of the vertical facial morphologic pattern.
Saltaji et al.[12] in another study examined the craniofacial morphology in three different overjet patterns; normal, increased and extreme overjet, and reported a positive association between the overjet and the tendency toward a vertical facial pattern. They concluded that the horizontal, neutral, and vertical patterns were dominant in Class II patients with normal, increased, and extreme overjet, respectively. Moreover, they reported that mean (S-N:Go-Me°) and (S-N-Gn°) angles were significantly increased whereas, the mean facial height ratio (S-Go:N-Me) was significantly decreased in extreme overjet group. They stated that the association between extreme overjet and vertical facial pattern may be the result of abnormal muscle function related to the mouth breathing and tongue thrust swallowing. In contrast, the present study did not find any statistically significant difference in the means of vertical facial cephalometric parameters among overjet groups, other than the mean facial height ratio (S-Go:N-Me).
Tanaka et al.[17] conducted a study to assess the correlation between Wits and AF-BF appraisals with the ANB angle and to verify the influence of the facial type on these appraisals. They evaluated ANB and Wits in a sample of 118 untreated individuals divided into the three groups according to the vertical facial pattern. The study identified a positive association between vertical facial pattern and ANB and Wits (R2 = 0.62) and concluded that facial pattern does not have an influence on the correlation between ANB and AF-BF nor between ANB and Wits, but it does influence the measurements of ANB, AF-BF, and Wits.
Siriwat and Jarabak [18] performed a study to examine associations between facial morphology and malocclusion. They concluded that based on the facial height ratio, a neutral growth pattern was dominant in Class II/1 malocclusion, and a hypodivergent pattern was dominant in Class II/2. Our results were in agreement with their results.
It has been assumed that the eruption of the second molars may influence the vertical facial dimension as well as the amount of overbite. Moreover, lower age group mostly does not have fully erupted second molars, unlike the older age group. Hence, in the present study, the whole sample was distributed in two groups (Group I = <12 years, Group II = >12 years) in order to see the impact of age on various study parameters. The statistically significant difference was not appreciated in the means of all the study parameters among groups.
In the present retrospective study, significant evidence on the validity and reliability of the data was not obtainable. Moreover, the present study was implemented only on orthodontic population. Therefore, results cannot be applied on generalized Pakistani population. To acquire more accurate data, a large study on community basis would need to be performed through valid and reliable measures of parameters of concern and calibration of the surveyors.
Clinical Implication
Although previous studies [12],[13],[17] have reported that sagittal pattern is highly correlated with vertical facial pattern, but in our study, we did not find any statistically significant correlation between sagittal pattern determined by overjet and the parameters that are used to assess vertical facial morphology. Hence, along with overjet, skeletal cephalometric parameters should be used as the predictors and representatives of the vertical facial pattern.
| Conclusion | | |
- Patients with Class II division 1 malocclusion have an average vertical growth pattern.
- Overjet value is not a predictor of the vertical facial morphology.
- There is no significant correlation between overjet and parameters used to assess vertical facial morphology.
| Acknowledgment | | |
Entire dental faculty and residents.
| References | | |
| 1. | Daskalogiannakis J. Glossary of Orthodontic Terms. Berlin: Quintessence Publishing; 2000.  |
| 2. | Kuitert R, Beckmann S, van Loenen M, Tuinzing B, Zentner A. Dentoalveolar compensation in subjects with vertical skeletal dysplasia. Am J Orthod Dentofacial Orthop 2006;129:649-57. |
| 3. | Ishikawa H, Nakamura S, Iwasaki H, Kitazawa S, Tsukada H, Sato Y. Dentoalveolar compensation related to variations in sagittal jaw relationships. Angle Orthod 1999;69:534-8. |
| 4. | Bishara SE, editor. Text Book of Orthodontics. Philadelphia: WB Saunders Co.; 2001. p. 53-60. |
| 5. | Erum G, Fida M. Pattern of malocclusion in orthodontic patients: A hospital based study. J Ayub Med Coll Abbottabad 2008;20:43-7. |
| 6. | Brook PH, Shaw WC. The development of an index of orthodontic treatment priority. Eur J Orthod 1989;11: 309-20. [ PUBMED] |
| 7. | Ben-Bassat Y, Brin I, Jarjoura R, Regev E. Morphological occlusal features following condylar fractures in children. Eur J Orthod 2012;34:147-51. |
| 8. | Sarver DM, Janyavula S, Cron RQ. Condylar degeneration and diseases-local and systemic etiologies. Semin Orthod 2013;19:89-96. |
| 9. | Proffit WR, Fields HW, editors. Contemporary Orthodontics. 4 th ed. St. Louis: C.V. Mosby; 2007. |
| 10. | McDowell EH, Baker IM. The skeletodental adaptations in deep bite correction. Am J Orthod Dentofacial Orthop 1991;100:370-5. |
| 11. | Zupancic S, Pohar M, Farcnik F, Ovsenik M. Overjet as a predictor of sagittal skeletal relationships. Eur J Orthod 2008;30:269-73. |
| 12. | Saltaji H, Flores-Mir C, Major PW, Youssef M. The relationship between vertical facial morphology and overjet in untreated class II subjects. Angle Orthod 2012;82:432-40. |
| 13. | Saltaji H, Flores-Mir C, Major PW, Youssef M. Vertical facial pattern and sagittal relationship in patients with class II malocclusion: Are they interrelated? World J Orthod 2012;1:115-20. |
| 14. | Jacabson A, Jacabson RL, editors. Radiographic Cephalometery from Basics to 3-D Imaging. 2 nd ed. Hanover Park: Quintessence Publishing Co.; 2006. |
| 15. | Iwasaki H, Ishikawa H, Chowdhury L, Nakamura S, Iida J. Properties of the ANB angle and the Wits appraisal in the skeletal estimation of angle′s class III patients. Eur J Orthod 2002;24:477-83. |
| 16. | Pae EK, McKenna GA, Sheehan TJ, Garcia R, Kuhlberg A, Nanda R. Role of lateral cephalograms in assessing severity and difficulty of orthodontic cases. Am J Orthod Dentofacial Orthop 2001;120:254-62. |
| 17. | Tanaka JL, Ono E, Filho Medici E, Cesar de Moraes L, Cezar de Melo Castilho J, Leonelli de Moraes ME. Influence of the facial pattern on ANB, AF-BF, and Wits appraisal. World J Orthod 2006;7:369-75. |
| 18. | Siriwat PP, Jarabak JR. Malocclusion and facial morphology is there a relationship? An epidemiologic study. Angle Orthod 1985;55:127-38. [ PUBMED] |
[Figure 1], [Figure 2], [Figure 3]
[Table 1], [Table 2], [Table 3], [Table 4], [Table 5]
|










 Search Pubmed for
Search Pubmed for