|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 3
| Issue : 3 | Page : 188-191 |
|
Seventh key of occlusion: Diagnostic significance in different angle's class I, II and III malocclusions
Rajkumar Maurya1, Ankur Gupta2, Jaishree Garg3, Harsh Ashok Mishra4
1 Department of Orthodontics, Corps Dental Unit, Bhopal, Madhya Pradesh, India
2 Department of Orthodontics, IDS, Bareily, Uttar Pradesh, India
3 Department of Periodontics, IDS, Bareily, Uttar Pradesh, India
4 Department of Orthodontics, Ashok Dental Hospital, Mumbai, Maharashtra, India
| Date of Web Publication | 11-Sep-2015 |
Correspondence Address:
Rajkumar Maurya
Corps Dental Unit, Bhopal Military Station, Bhopal, Madhya Pradesh
India
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.155991

Introduction: As significant tooth size discrepancies prevent an ideal occlusion being produced at the end of orthodontic treatment, absence of a tooth size discrepancy is the seventh "key" for an ideal occlusion. Present study aimed to assess diagnostic reliability of Bolton's ratio for different Angle's malocclusion. Materials and Methods: The study models of 144 patients were divided in three groups based on malocclusion.The mesiodistal tooth width from permanent first molar to first molar were measured on the orthodontic study models. The readings were obtained using a digital vernier caliper to the nearest 0.01mm, with the blades of the caliper held perpendicular to the long axis of the tooth. Results: ANOVA showed no significant difference between all groups except between anterior ratio of Class II group. The mean ratio for the Class III sample was significantly greater than Class I and Class II subjects (P < 0.05). The overall ratio was significantly larger for the Class III subjects than other groups, but with no significance for either gender. Regarding absolute values, mean overall ratio for the different groups was in the order Class III > Class I > Class II with significant difference between the Class I and Class II groups. Conclusion: Subjects with Class III group had a significantly greater prevalence of tooth size discrepancies than Class I and Class II group. Statistically significant difference was seen in the anterior ratio between the males and females of Class II malocclusion and no significant difference between other groups. Keywords: Analysis of variance, Bolton′s ratio, malocclusion
How to cite this article:
Maurya R, Gupta A, Garg J, Mishra HA. Seventh key of occlusion: Diagnostic significance in different angle's class I, II and III malocclusions. J Orthod Res 2015;3:188-91 |
How to cite this URL:
Maurya R, Gupta A, Garg J, Mishra HA. Seventh key of occlusion: Diagnostic significance in different angle's class I, II and III malocclusions. J Orthod Res [serial online] 2015 [cited 2018 Sep 6];3:188-91. Available from: http://www.jorthodr.org/text.asp?2015/3/3/188/155991 |
| Introduction | |  |
A tooth size discrepancy is a proportion among the sizes of the individual teeth. [1] As significant tooth size discrepancies prevent an ideal occlusion being produced at the end of orthodontic treatment, the absence of a tooth size discrepancy is the seventh "key" for an ideal occlusion. [2] Overall tooth size discrepancy relate to all teeth excluding permanent second and third molars, whereas anterior tooth discrepancies involve the six anterior teeth.
Tooth size exhibits a continuous range of variation among individuals and populations. Tooth size represents an important diagnostic tool that illustrates some prediction of treatment outcomes and may also limit the necessity for diagnostic managements for complex cases. A proper relationship of the total mesiodistal width of the maxillary dentition to the mesiodistal width of the mandibular dentition favors an optimal post treatment occlusion. [3]
A significant variation in the harmony of tooth size ratio leads to malocclusion and difficulties in obtaining an occlusion with optimal over-jet, overbite, and Class I canine and molar relationships. [1] The size of the teeth matches very well in most individuals however some degree of discrepancy exists among individuals of any population. Though Bolton's study has been done in the past by many researchers, there is no conclusive study or guidelines or its correlation with a heterogeneous population. Following the study was conducted to assess if there is any applicability and clinical reliability of Bolton's ratio among different Angle's Class I, II, and III malocclusion.
| Methodology | | |
The study models of 144 patients aging from 12 to 30 years were selected from OPD. The sample included 60 sample of Class I (30 males, 30 females), 60 sample of Class II group comprised of 30 males, 30 females, and Class III group consisted of 24 individuals (12 males, 12 females) with random age group from 12 to 30 years. The inclusion criteria were based on equivalent skeletal and dental classification, all permanent teeth (except third molars) erupted in the upper and the lower arches, absence of visible crowding, spacing, proclination or ectopic eruption, good quality study models, absence of any dental deformity or severe mesiodistal, and occlusal tooth abrasions, no restorations extending to the mesial or distal surfaces, or enamel stripping of the anterior or posterior teeth.
The sagittal relationship was assessed cephalometrically using the ANB angle: Skeletal Class I, from 0° to 4°, Class II, >4° and Class III <0°. The occlusal characteristics of all subjects were classified using Angle's classification and corresponded to the skeletal relationships.
The mesiodistal tooth width from permanent first molar to first molar was measured on the orthodontic study models by single author Dr. RM. The readings were obtained using a digital Vernier caliper (Mitutoyo Digimatic Caliper, Mitutoyo Corporation, Japan) to the nearest 0.01 mm, with the blades of the caliper held perpendicular to the long axis of the tooth [Figure 1].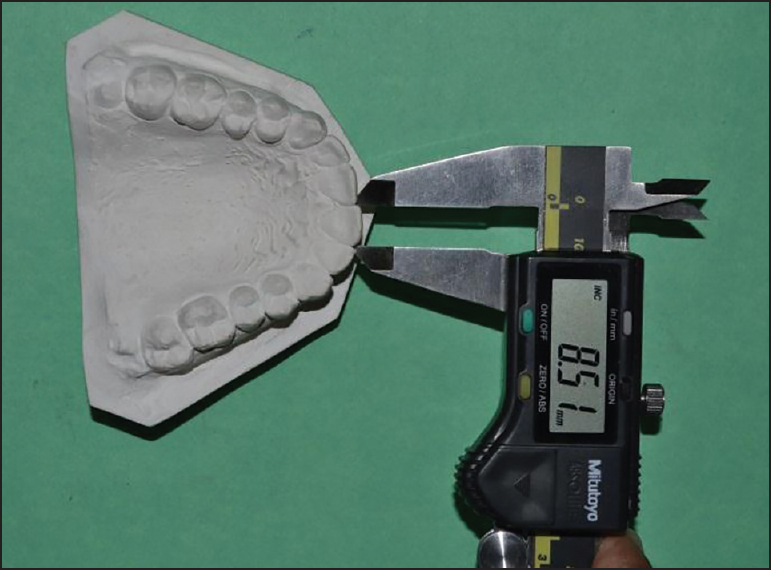 | Figure 1: Measurement of mesiodistal width with the help of digital Vernier caliper
Click here to view |
The anterior and the overall ratio (AR and OR) tooth size ratios were calculated for each subject as described by Bolton:
Bar = (S6 Mand/S6 Max)× 100, Bor = (S12 Mand/S12 Max) × 100
Where,
BAR and BOR = AR and OR respectively.
S12 Mand - Σ of the 12 mandibular teeth (mm).
S12 Max - Σ of the 12 maxillary teeth (mm).
S6 Mand - Σ of the 6 mandibular teeth (mm).
S6 Max - Σ of the 6 maxillary teeth (mm).
In order to determine the measurement error, the study models of 25 randomly selected individuals were measured again by the same examiner after a week's interval. An analysis of error was performed using the nonparametric Wilcoxon statistical test. The results showed no significant difference between the two measurements.
To compare the prevalence of tooth size discrepancies among the three malocclusion groups and two genders, a Chi-square test was performed. In addition, to compare the mean Bolton tooth size ratios as a function of Angle's classification, as well as gender, analysis of variance (ANOVA), was undertaken.
| Results | | |
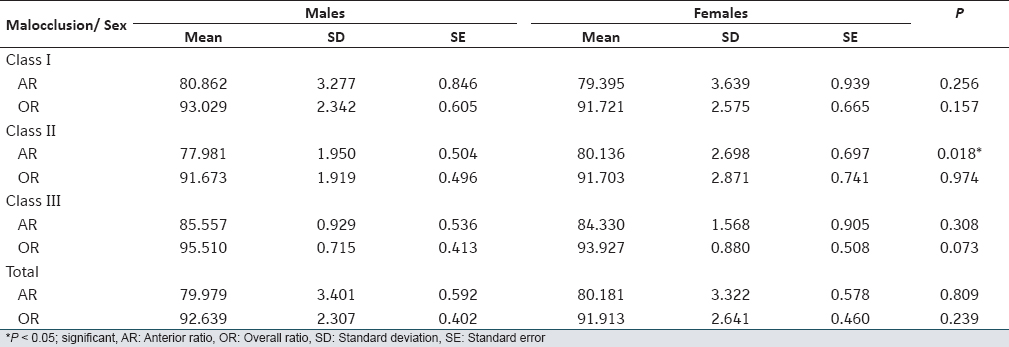
The means, standard deviation, and standard error of the tooth size ratios were obtained for each group [Table 1].
Anterior ratio
The mean AR of male subjects (79.979 ± 3.40) showed no significant difference than that of female subjects (80.181 ± 3.32). ANOVA demonstrates that there is no significant difference between all groups except between the AR of Class II males and females [Table 2].
Using Duncan's multiple range tests, it was found that no significant difference was present between Class II and Class I malocclusion, but significant differences were seen between Class I and Class III malocclusion and also in between Class II and Class III malocclusion subjects. The mean ratio for the Class III sample was significantly greater than that for the Class I and Class II subjects (P < 0.05) when compared with each other [Table 3].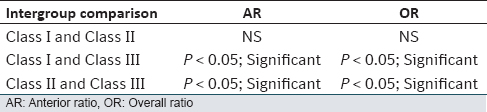 | Table 3: Significant mean ratios between different malocclusion group using Duncan's multiple tests
Click here to view |
Overall ratio
The OR was significantly larger for the Class III malocclusion subjects than the other groups, but with no significance for either gender. Regarding absolute values, the mean OR for the different groups was in the order Class III > Class I > Class II. In addition, there was statistically significant difference between the Class I and Class II malocclusion groups.
| Discussion | | |
The findings of the present study demonstrates significant difference in the AR between males and females of the Class II malocclusion group and no significant difference in between the other malocclusion, and also no significant difference between the OR and the three malocclusion groups.
When comparing the mean to interpret the AR and OR, the results of the present study were not similar to that of Bolton [1] and Stifter. [4] For AR and OR, which were 80.08 ± 3.34 and 92.28 ± 2.49 when all malocclusion subjects (i.e., 144 patients) were combined, no similarity was found. The subjects in the present study all had malocclusions sufficiently, severe to warrant treatment, and it is possible that this is contributed to the larger percentage of tooth size discrepancies in the anterior as well as posterior region.
The findings that individuals with a Class III malocclusion have a significantly greater mean AR than the other groups may confirm the results of Lavelle [5] that Class III individuals have disproportionately smaller maxillary teeth than Class I and Class II subjects. However, a small size of the maxillary teeth was not found in the present study. Therefore, the Bolton discrepancy in the Class III sample must either be attributed to an increase in the width of the mandibular anterior teeth or the accumulation of minor discrepancies of individual teeth.
The results obtained by Nie and Lin [6] using Angle's classification as a variable in analyzing 360 Chinese individuals for tooth size discrepancies are in agreement with the present findings that Class III patients demonstrate a greater tooth size discrepancy when compared with Class II and I patients. These findings also confirm the initial investigations by Sperry et al.[7]
Crosby and Alexander [8] tried to verify the presence of a tooth size discrepancy in 109 patients divided into four malocclusion groups, but not including Class III subjects.
They compared the average of the anterior and overall Bolton indices but did not find any statistical difference in the incidence of the tooth size discrepancy among the groups (Class I, Class II divisions 1 and 2, and surgical Class II). Some of the findings in the present investigation were similar to their results with respect to the absence of statistically significant differences when comparing Class I, and Class II malocclusion groups. Since they did not include subjects with a Class III malocclusion in their investigation, they could not find any difference between normal occlusion and malocclusion groups coinciding with the Bolton indices, while in the present study, a large part of the differences in the Bolton indices were attributed to the presence of a Class III malocclusion.
Regarding studies reporting the mesiodistal dimensions of lower teeth to be larger in Class III malocclusion subjects when compared with Classes I and II (divisions 1 and 2), it seems that the greater mean of Bolton's ratio in these classes might be due to etiological factors that lead to mandibular prognathism. [5],[7] Further studies are needed to clarify whether a correlation exists between increased mandibular growth (as in Class III malocclusions) with increased mesiodistal dimensions of lower anterior teeth. The possible interaction of genetic factors could determine mandibular size while affecting the mesiodistal dimensions of lower mandibular teeth, in the same way.
| Conclusions | | |
Subjects with an Angle Class III malocclusion had a significantly greater prevalence of tooth size discrepancies than those with Class I and Class II malocclusions. Statistically, a significant difference was seen in the AR between the males and females of Class II malocclusion, however, no significant difference was seen in the OR in the three malocclusion groups. Significant difference was seen between the mean AR and OR when Class I versus Class III and Class II versus Class III groups were compared, but no significant difference was seen when Class I versus Class II groups.
| References | | |
| 1. | Bolton WA. Disharmony in tooth size and its relation to the analysis and treatment of malocclusion. Angle Orthod 1958;28:112.  |
| 2. | Bennett JC, McLaughlin RP. Orthodontic Management of the dentition with the Preadjusted Appliance. 1 st ed. Edinburgh: Mosby; 2001. p. 12, 14, 54, 56, 86-91. |
| 3. | Santoro M, Ayoub ME, Pardi VA, Cangialosi TJ. Mesiodistal crown dimensions and tooth size discrepancy of the permanent dentition of Dominican Americans. Angle Orthod 2000;70:204-13. |
| 4. | Stifter J. A study of Pont′s, Howes′, Rees′, Neff′s and Bolton′s analyses on class I adult dentitions. Angle Orthod 1958;28:215-25. |
| 5. | Lavelle CL. Maxillary and mandibular tooth size in different racial groups and in different occlusal categories. Am J Orthod 1972;61:29-37. |
| 6. | Nie Q, Lin J. Comparison of intermaxillary tooth size discrepancies among different malocclusion groups. Am J Orthod Dentofacial Orthop 1999;116:539-44. |
| 7. | Sperry TP, Worms FW, Isaacson RJ, Speidel TM. Tooth-size discrepancy in mandibular prognathism. Am J Orthod 1977;72:183-90. |
| 8. | Crosby DR, Alexander CG. The occurrence of tooth size discrepancies among different malocclusion groups. Am J Orthod Dentofacial Orthop 1989;95:457-61. |
[Figure 1]
[Table 1], [Table 2], [Table 3]
|










 Search Pubmed for
Search Pubmed for