|
 
 |
| CASE REPORT |
|
| Year : 2016 | Volume
: 4
| Issue : 1 | Page : 24-27 |
|
Reconstruction of orofacial injury due to a horse hoof kick: Report of a case
Mehmet Dalkiz1, Fundagul Bilgic2
1 Department of Prosthetic Dentistry, Faculty of Dentistry, Mustafa Kemal University, Hatay, Turkey
2 Department of Orthodontics, Faculty of Dentistry, Mustafa Kemal University, Hatay, Turkey
| Date of Web Publication | 5-Apr-2016 |
Correspondence Address:
Fundagul Bilgic
Department of Orthodontics, Faculty of Dentistry, Mustafa Kemal University, 31100 Hatay
Turkey
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.172220

We report the case of an orofacial injury caused by a horse kick. Animal attacks most commonly involve domestic animals, such as dogs, cats, bulls, camels, and horses. When an orofacial injury caused by a kick from a horse occurs, it is often serious, and may even be fatal. Children are the most common victims of horse kick injuries, generally being attacked by a horse they know. The patient was successfully treated via three stages of reconstruction: surgical, orthodontic, and prosthetic. Keywords: Horse kick, orofacial deformity, prosthetic reconstruction, rapid palatal expansion
How to cite this article:
Dalkiz M, Bilgic F. Reconstruction of orofacial injury due to a horse hoof kick: Report of a case. J Orthod Res 2016;4:24-7 |
| Introduction | |  |
Horse-related injuries comprise approximately 55% of the accidents caused by large animals. [1] However, maxillofacial injuries caused by animal incidents are uncommon, with the head, hand, wrist, foot, ankle, vertebral column, and spinal cord being the most susceptible to horse-related injuries. [2],[3] Injuries caused by horses may occur due to a horse hoof kick, a horse throwing its head, falling from a horse, or a horse bite. [4] Furthermore, 79% of horse-related injuries are associated with a hoof kick and may result in head or facial injuries, abrasions, fractures, strains, lacerations, and internal injury. [3]
Horse accidents most often occur while riding horses or farming, whether in a field or a paddock. In addition, these accidents are more common in the warmer weather. Therefore, the use of helmets or protective headgear, as well as learning how to properly deal with horses, may reduce the serious head injury risks caused by horse-related injuries. Face shields and mouth guards for facial and oral protection are recommended during contact sports involving horses. [3],[5]
The objective of this study was to report a severe case of dentoalveolar fracture caused by a horse's hoof kick.
| Case Report | | |
A 12-year-old male was referred to the Army Medical Center, from a nearby small rural town, with a history of having been attacked by a horse 2 years previously. The patient had undergone immediate surgical closure of the facial wounds, as well as repair of the upper lip, at Another Hospital. Two years later, the patient exhibited an orofacial deformity, so a functional occlusal reconstruction was undertaken, starting with the removal of the impacted left maxillary central and lateral incisor teeth and a rapid palatal expansion, followed by a prosthetic application (fixed partial denture).
At the time of presentation, the patient was conscious, alert, and calm, and the clinical examination showed normal vital signs. The radiological evaluation showed a callused fracture line on the right side of the maxilla and at the roots of the first and second upper incisor teeth. During the extraoral examination, a scar line was observed traveling from the left lower part of the left nostril to the vestibular sulcus, passing directly through the upper lip.
On intraoral examination, all teeth were observed in situ, except the left central and lateral incisors. The upper left central and left lateral incisor teeth were avulsed (unerupted), and there were anterior and posterior crossbites with a loss of occlusal contact, with the exception of the right upper first central incisor (to the lingual side of the lower incisors). There was hard tissue observed in the upper anterior region, with infected tissues visible nearby [Figure 1].
A treatment plan was created to form a functional occlusion, with surgical, orthodontic, and finally, prosthetic stages. Through the surgical approach, the impacted roots and infected tissues were removed [Figure 1]. Fifteen days later, to treat the anterior and posterior cross-bite issues, we designed a fixed rapid maxillary expansion (RME) appliance using a Hyrax-type screw. The patient was instructed to twist the screw open twice daily for 20 days, in order to expand the maxilla [Figure 2]. For retention, the patient continued to use the RME device for 3 additional months [Figure 2].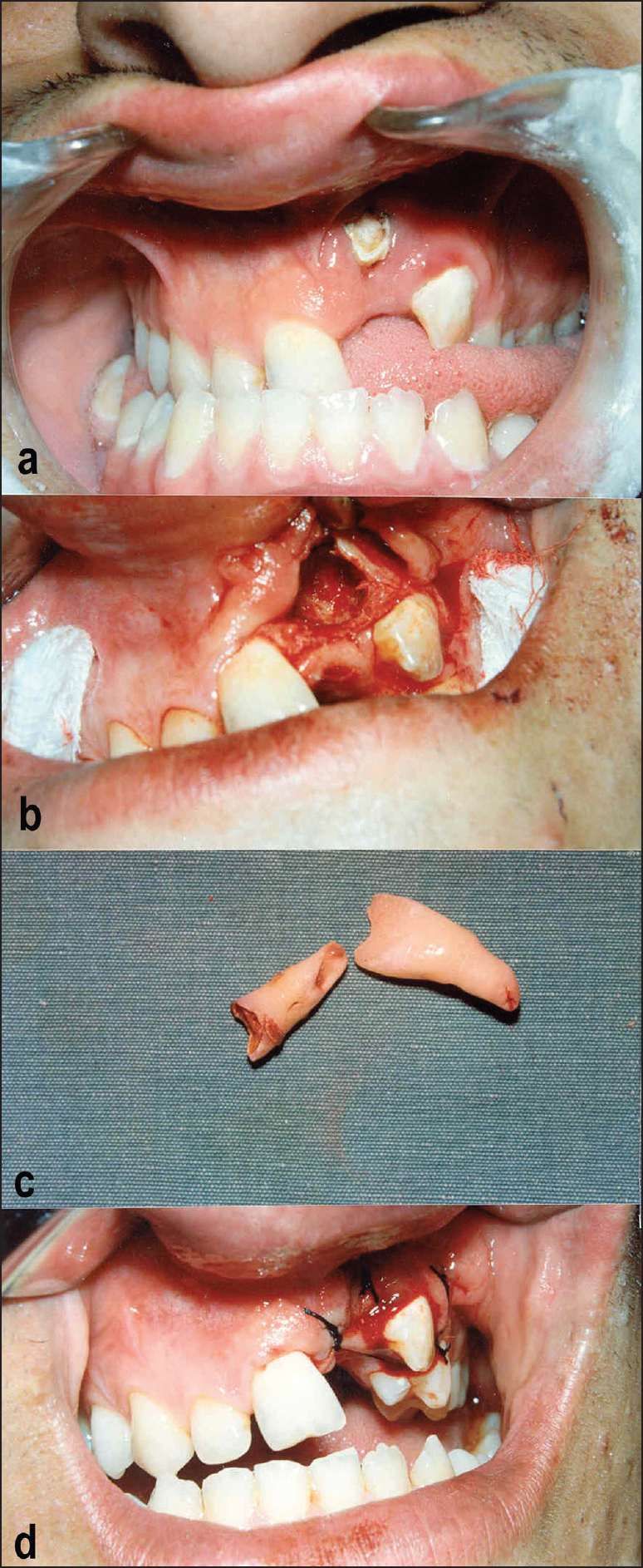 | Figure 1: Photographs of the surgical procedure: (a) Upper left central and left lateral incisor teeth showing avulsion (unerupted). Anterior and posterior cross-bite with a loss of occlusal contact, except in the right upper first central incisor. (b-d) Surgical approach; impacted tooth roots and infected tissues were removed
Click here to view |
 | Figure 2: A fixed rapid maxillary expansion appliance with a Hyrax-type screw
Click here to view |
Next, to bring the upper left canine tooth distally and extrude, a new removable appliance was designed. A cleat was bonded to the vestibular face of the upper left canine tooth, and elastics were used from the canine to the vestibular arch of the appliance. The patient continued to use this appliance until the canine came into the desired position, which occurred after 18 months [Figure 3].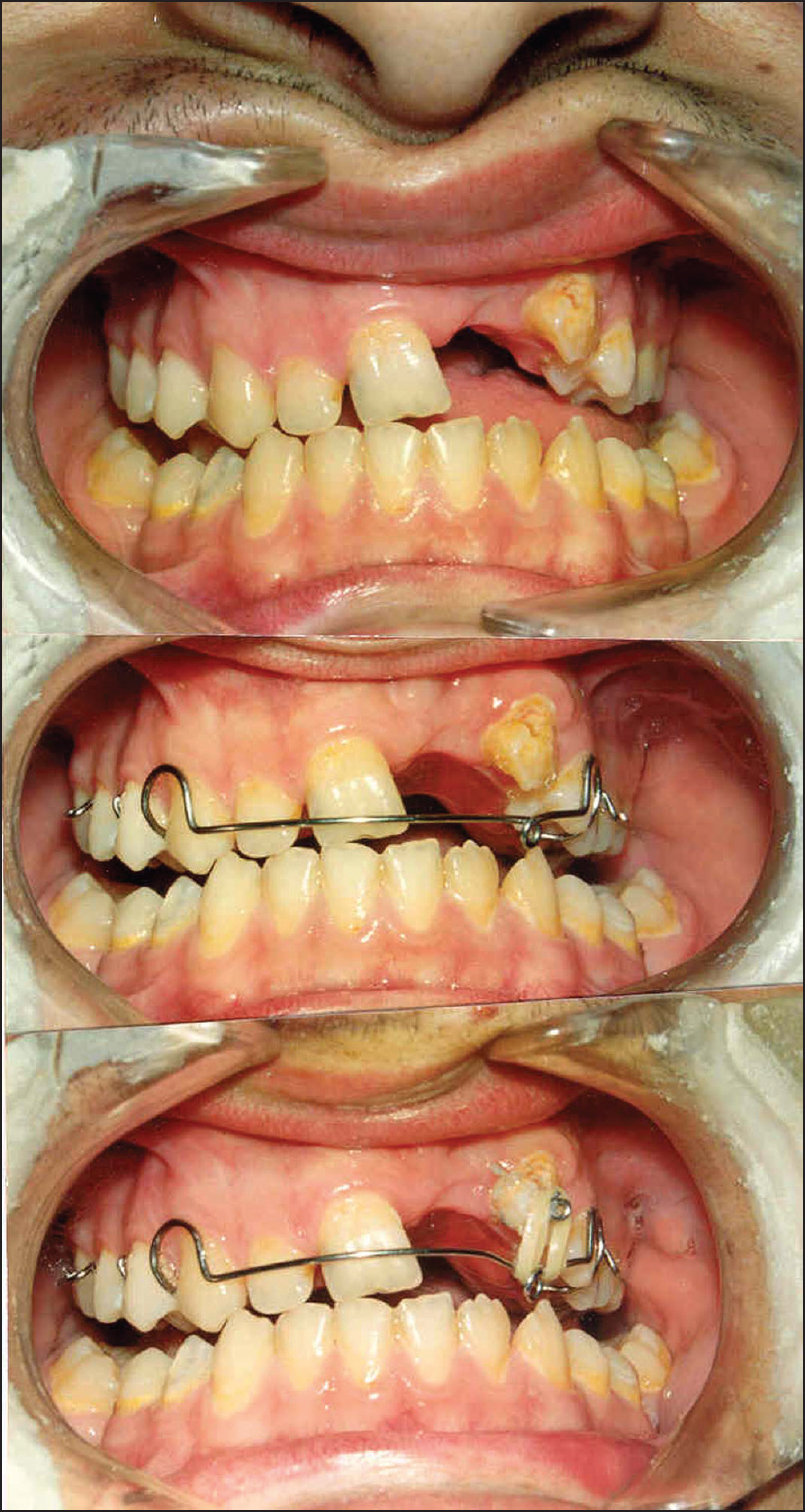 | Figure 3: Removable orthodontic appliance for upper left canine tooth (for distal movement and extrusion)
Click here to view |
For the final stage, the prosthetic treatment was begun. By using the upper right canine tooth for guidance, the posterior part of the mandibular dental arch was restored bilaterally. Metal-porcelain bridges were used so that the patient gained posterior occlusal contact for good mastication [Figure 4].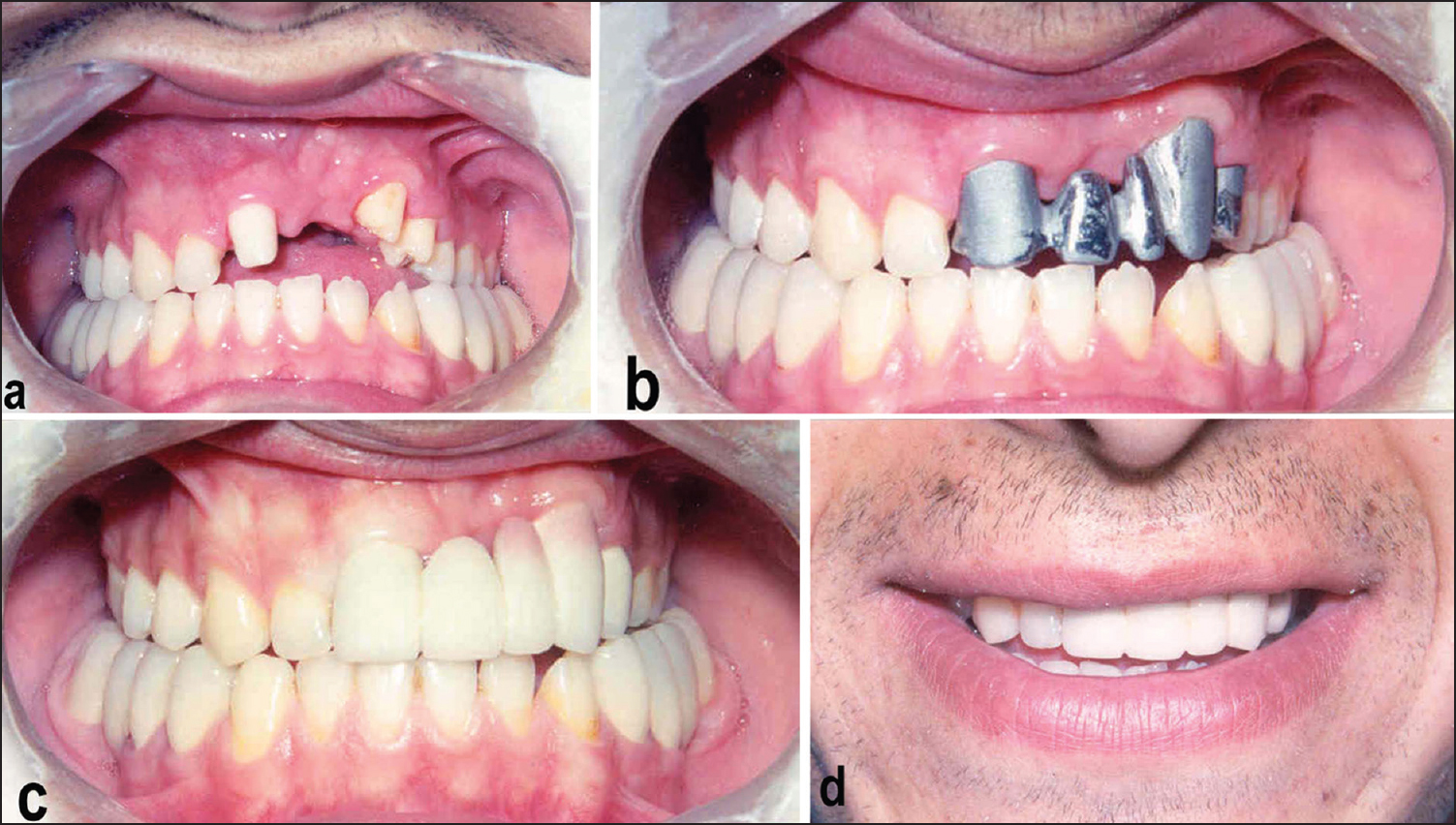 | Figure 4: Anterior metal-porcelain bridge: (a) Prepared anterior teeth. (b) Checking the metal casting. (c) Anterior metal porcelain bridge. (d) Gained aesthetic appearance
Click here to view |
After the patient had turned 17-year-old, a restoration from the upper right first incisor to the first left bicuspid tooth was completed using metal-porcelain bridges [Figure 4]. Finally, the patient obtained an aesthetic smile together with good functional occlusion.
| Discussion | | |
The human facial region is a frequent target of animal attacks. Facial defects can vary in size and severity depending on the injured anatomical structures, including the nose, lips, and maxillary and mandibular bones. [6],[7],[8],[9] Surgical correction of these injuries remains an important challenge, due to both the lesion itself and the resulting infection. Delayed reconstruction of significant facial defects may cause an undesirable appearance and physiological problems for the patient. The initial approach to injuries caused by animal attacks depends on several well-known principles, including anti-tetanus prophylactic irrigation of the wound with 1% iodine solution, and antibiotic prophylaxis. In our case, we administered prophylactic antibiotic therapy for 7 days.
In the RME method, during the 1 st or 3 rd weeks, appropriately spaced and strong forces are applied to the midpalatal suture to separate the two parts of the maxilla from each other. The aim is to obtain the greatest skeletal effect, with the least movement of the teeth, using heavy strengths. [10] Any maxillary narrowness caused by a maxillary fracture is treated using RME in order to obtain an ideal occlusal relationship, as well as an aesthetic appearance. In this case, with a one-fourth rotation of the screw twice per day, the RME continued for 20 days, and a retention plate was used for 3 months.
Researchers have reported that after urgent surgical intervention, a prosthetic restoration prevented speech and chewing disorders and provided a good aesthetical appearance; therefore, any psychological problems could be resolved. [7],[8] We applied fixed prosthetic restorations (metal-porcelain) in our case, after RME treatment, to provide good masticatory and speech functions, as well as a good appearance.
During the 5 years follow-up examination, this patient was determined to be doing well.
A multidisciplinary approach prevents most complications of a facial-jaw trauma and can obtain an aesthetic smile together with good functional occlusion, for the patient.
Financial Support and Sponsorship
Nil.
Conflicts of Interest
There are no conflicts of interest.
| References | | |
| 1. | Norwood S, McAuley C, Vallina VL, Fernandez LG, McLarty JW, Goodfried G. Mechanisms and patterns of injuries related to large animals. J Trauma 2000;48:740-4.  |
| 2. | Martins WD, Fávaro DM, Ribas Mde O, Martins G. Dentoalveolar and mandibular body fractures caused by a horse kick: Report of a case. J Contemp Dent Pract 2006;7:137-44. |
| 3. | Hawson LA, McLean AN, McGreevy PD. The roles of equine ethology and applied learning. Theory in horse-related human injuries. J Vet Behav 2010;5:324-38. |
| 4. | Blümel J, Pfeifer G. Injuries caused by horses and their effects on maxillofacial regions analysis of cases in nordwestdeutsche kieferklinik from 1970 - 1975 (author′s transl)]. Unfallheilkunde 1977;80:27-30. |
| 5. | Douglas BL. Oral protection for equestrians. CDS Rev 1995;88:28-30. |
| 6. | Giebel G, Braun K, Mittelmeier W. Equestrian accidents in children. Chirurg 1993;64:938-47. |
| 7. | Cooter RD, Dunaway DJ, David DJ. The influence of maxillary dentures on mid-facial fracture patterns. Br J Plast Surg 1996;49:379-82. |
| 8. | Wiens JP. Acquired maxillofacial defects from motor vehicle accidents: Statistics and prosthodontic considerations. J Prosthet Dent 1990;63:172-81. |
| 9. | Giraldo-Ansio F, García-Domínguez MD, Abad-Mariñez A. One-stage immediate reconstruction of partial auricular amputation by dog bite. Int J Oral Maxillofac Surg 1997;26:260-2. |
| 10. | Silverstein K, Quinn PD. Surgically-assisted rapid palatal expansion for management of transverse maxillary deficiency. J Oral Maxillofac Surg 1997;55:725-7. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
|










 Search Pubmed for
Search Pubmed for