|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2016 | Volume
: 4
| Issue : 1 | Page : 8-12 |
|
Evaluation of cervical spine posture after functional therapy with twin-block appliances
Cahide Aglarci
Department of Orthodontics, Faculty of Dentistry, Sifa University, Izmir, Turkey
| Date of Web Publication | 5-Apr-2016 |
Correspondence Address:
Cahide Aglarci
Department of Orthodontics, Faculty of Dentistry, Sifa University, Mansuroglu Mahallesi 293/1 Sokak, No: 2, 35100 Bayrakli, Izmir
Turkey
 Source of Support: None, Conflict of Interest: None  | Check |
DOI: 10.4103/2321-3825.179739

Objective: The aim of this study was to investigate the effect of the twin-block appliances to the cervical spine posture. Materials and Methods: Twenty-one skeletal Class II patients (11 female, 10 male; 13.31 ± 0.92) with mandibular retrusion were included in the study. Twin-block appliances with no expansion protocol were applied to all individuals. Cervical spine posture changes after treatment were evaluated by cephalograms. The differences between pre- and post-treatment measurements were evaluated by paired sample t-test. Results: No significant differences were observed after treatment, in the angle between the horizontal lines of the head (sella-nasion, anterior nasal spine-posterior nasal spine, and gonion and gnathion) and the upper and middle section of the spinal column (odontoid process tangent [OPT] and cerebral venous thrombosis [CVT]) (P > 0.05), while the increase of cervical curvature angle (OPT/CVT°) was found significant after the treatment (P = 0.009). Conclusion: A backward inclination of the middle segment of cervical column seems to be associated with the advancement of the mandible by twin-block treatment. Keywords: Cervical posture, head posture, twin-block
How to cite this article:
Aglarci C. Evaluation of cervical spine posture after functional therapy with twin-block appliances. J Orthod Res 2016;4:8-12 |
| Introduction | |  |
Cervical posture is related with the craniofacial morphology; mostly mandibular divergence, mandibular size, and facial shape. [1],[2] A strong association has been devoted among the sagittal skeletal malocclusions and posture of the neck in the literature. [3] However the cause-effect relationships between craniofacial form and head posture have not been clearly established.
The relationship between a habitual lack of an upright head posture, an Atlas More Details inferior position, and a lordosis of the cervical spine relation with the angle Class II has been demonstrated. [4] In addition, a negative correlation between the cervical lordosis angle and mandible length in adult skeletal Class II individuals was stated. [2],[5]
The effect of functional orthopedic treatment of the skeletal Class II to the head posture was also investigated. It was established that craniocervical system changes occur after mandibular base is repositioned in a more anterior position. [4],[6] Cervical lordosis seems to increase after mandibular advancement by a functional appliance, for instance, with a FR-2. [6]
Orthodontic appliances can produce improvement on the maxillo-mandibular relationship. [4] Numerous studies showed the changes of craniofacial morphology after the twin-block therapy on lateral skull radiographs. [7],[8] To our knowledge, no study has been focused whether cervical spine posture changes occurred after the twin-block therapy.
The aim of this study was to investigate the effect of the twin-block appliances to the cervical spine posture.
| Materials and Methods | | |
Study Sample
Study sample was selected from patients who were consecutively admitted to the Department of Orthodontics, Sifa University, Izmir, Turkey. Patients according to criteria as following were included in the study: (1) No prior orthodontic treatment, (2) skeletal Class II malocclusion (ANB° ≥5°) (3) prepubertal period (evaluated from cephalometrics by cervical vertebral stadium method) (4) vertically normal growth pattern (sella-nasion [SN]-GoGn <40°).
Subjects with known mandibular or craniofacial pathology and systemic muscle and joint disorders were excluded from the study sample.
Three patients were excluded due to co-operation problems. Finally, 21 patients who met these criteria (11 female and ten male) were included in the study.
Treatment Protocol
No expansion screws were used in appliances and no transversal expansion protocol was applied. The construction bite of the appliance was recorded. The acrylic blocks are placed on the occlusal surface of posterior teeth with a vertical opening of 2-3 mm between upper and lower incisors and sagittally advancing the mandible to an edge-to-edge incisor relationship. The anterior portion of planes present an angle of 70°, which, in combination with the mandibular planes, keeps the mandible protruded.
All patients were asked to use their appliances at least 18 h a day. Treatment was continued until Class I or slight Class III molar relationship was achieved.
Cephalometric Analysis
Lateral cephalograms were obtained at the beginning (T1) and at the end (T2) of treatment. Cephalograms were taken with the teeth in occlusion and in the standardized head posture, the mirror position. [9]
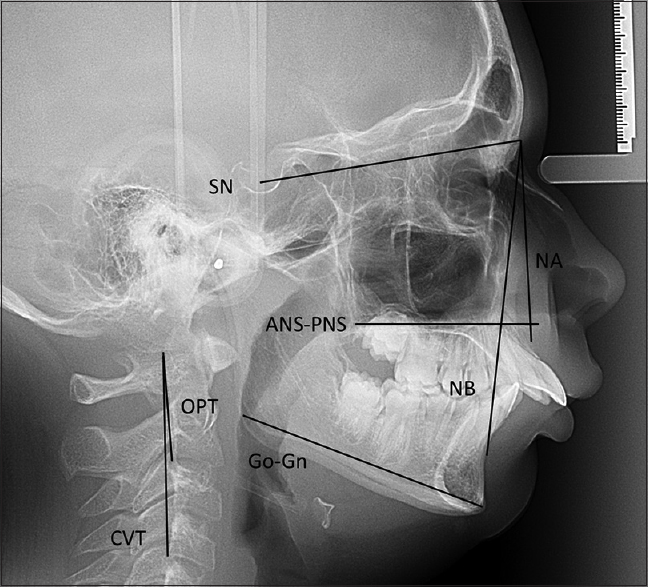
All cephalometric measurements were obtained by the same author (C.A.). Eleven measurements representing the vertical and the sagittal craniofacial dimensions and the head posture were calculated. A list of the cephalometric lines was defined in [Table 1] and demonstrated in [Figure 1].
Statistical Analysis
All statistical analyses were performed with SPSS for Windows Version 20.0 (SPSS Inc., Chicago, IL, USA). Numerical variables were represented by mean and standard deviation. The Kolmogorov-Smirnov test was performed for homogeneity assessment. The differences between pre- and post-treatment measurements were evaluated by paired sample t-test. P <0.05 was considered statistically significant.
Method Error
Reliability of the measurements was assessed by remeasuring 30% of the lateral radiographs selected at random from the previously evaluated radiographs. All measurements of 13 cephalograms that were randomly selected, repeated 1 month after the first tracing. Cronbach's reliability test was performed to detect method error. Intra-class correlation coefficients were found to be within a range of 0.792-0.965. No statistically significant differences were found between the first and second measurements.
| Results | | |
Age, treatment duration, and pubertal stages of the study group were demonstrated in [Table 2]. Age and treatment duration were normally distributed and did not differ significantly between the genders (respectively; P = 0.473, P = 0.923) [Table 2]. All pretreatment measurements showed a normal distribution (P = 0.457-0.998). Total data of genders were used to evaluate the differences between pre- and post-treatment measurements, due to no significant gender dimorphisms was found. | Table 2: Differences of the age and treatment duration between genders and pubertal stage distribution
Click here to view |
Mean cephalometric measurement changes between T1 and T2 are presented in [Table 3]. Reduction of the ANB° angle (P < 0.001) [Table 3] and increase of the SNB° (P < 0.001) [Table 3] angle are significant, while reduction of the SNA° (P = 0.138) [Table 3] angle is insignificant. Slight increase was observed in vertical dimensions, however the change between T2-T1 is insignificant (SN/gonion and gnathion [Go-Gn°]; P = 0.11) [Table 3].
No significant differences were observed after treatment, in the angle between the horizontal lines of the head (SN, anterior nasal spine-posterior nasal spine, and Go-Gn) and the upper section of the spinal column (odontoid process tangent [OPT]) in the present study (P > 0.05) [Table 3].
All measurements that have been created between the midsection of the spinal column (cerebral venous thrombosis [CVT]) and horizontal lines of the head showed increase after treatment, however the differences after treatment are not statistically significant.
The increase of cervical curvature angle (OPT/CVT°) was found significant after treatment (P = 0.009) [Table 3].
| Discussion | | |
The probability of developing the cervical curvature through the use of an oral appliance, twin-block in skeletal Class II individuals, was investigated in this clinical study.
Besides skeletal improvements of the skeletal-sagittal relationship was achieved; increase of the cervical curvature angle was observed.
The effect of a few functional appliances to the head posture was investigated. However, twin-block is a commonly used functional appliance in the orthodontic clinics and the changes in the skeletal, dental, and airway dimensions were reported widely already in the literature, [7],[8],[10] this is the first study that gives information about the effect on head posture and cervical spine.
It was reported that cervical posture is related to age. Therefore, only patients in prepubertal stage and similar ages were included in the present study.
Maxillary expansion could cause an increase in the nasal cavity's total volume. [11] The influence of respiratory airway function on craniofacial development and head posture has been demonstrated. [12] Thus, no expansion protocol was applied in the present study to avoid the effect of expansion to the results.
Significant changes were observed in the craniofacial skeletal measurements, since this has been noted in a number of previous studies. [7],[8] Improvement in the maxillo-mandibular relationship was obtained, depending on significant mandibular protrusion after the treatment.
The morphological development of the upper and the middle segments of the spine (respectively; OPT, CVT) is closely linked to facial development. [13] In skeletal Class II patients, it was reported that a more lordotic curve of the spine is related to a greater extension of the head on the spinal column. [3] Furthermore, it was reported that the upper cervical spine is the mediator between head and trunk that forms a functionally inter-related system. [14]
No significant change was found between the upper section of the spinal column and horizontal lines of the head (cranial base, palatal plane, and mandibular plane) in the current study. Similar to this study, no major changes were showed between upper section of the spinal column and cranial base, palatal plane after functional treatment of skeletal Class II by activator, and bite-jump appliance. [4] Despite these results, significant increase was found after FR-2 treatment in those measurements mentioned above. [6] However, treatment duration was quite long in FR-2 study (2.5 years) in comparison with the current study (0.7 year) and in a recent study that gives results of activator and bite-jump appliance (1 year). The results are reflecting the combined effects of growth as well as treatment, as the patients in this study have to still grow. A control group is needed to assess the growth effects involved and to determine the clear effect of treatment.
Similar to upper cervical spine, no major changes was observed in the midsection of the spinal column. However, a nonsignificant slight increase was demonstrated in SN/CVT. It was reported that subjects in skeletal Class II demonstrated a more extended head upon the spinal column (SN/CVT) than subjects in skeletal Classes I and III in a previous study. [3] The growth pattern of the Class II individuals could be the cause of the slight increase in this measurement.
It was reported that lower angulation between the mandibular line and the midsection of the spinal column (Go-Gn/CVT) was observed in skeletal Class II in comparison with skeletal Class III. [3] In addition, significant increase was reported after FR-2 treatment. [6] However, in this study, increase of Go-Gn/CVT was not found significant. After twin-block treatment, changes in lower facial height could occur and might camouflage the change during growth and development. [10]
During skeletal Class II treatment, the position of upper cervical spine change was demonstrated in previous studies. [4],[6] Cervical curvature angle (OPT/CVT°) was significantly increased after twin-block treatment according to the present study's result. The activator treatment effect was reported, authors noticed that activator effects on upper cervical spine are more pronounced than the treatment of bite-jump appliance.
As a slight increase in all measurements were observed with the middle segment of the cervical column (CVT) in the current study, the advancing of the mandible seems to influence the increase in the cervical curvature angle due to the backward inclination of the middle segment of the cervical column, as similar results were achieved after the FR-2 treatment. [6] It could be well expected that different functional appliances, in various design based on mandibular advancement, could provide the same findings.
The major limitation of the study could be the effect of the gender. Most of the previous studies included female subjects as cervical spine inclination has been associated to gender, since men usually present a straightened curve and women usually present a partly reversed curvature. [4],[6] However, similar number of patients were included in the study according to gender. Results of the current study could be considered the mean value of males and females. [3] In addition, no differences were found between gender according to age and treatment duration. In addition, pubertal stages are quite similar.
Further studies including a Class II control group are needed to determine whether these effects may be caused directly by the functional treatment, regardless of growth. [4]
| Conclusion | | |
A backward inclination of the middle segment of cervical column seems to be associated with the advancement of the mandible by twin-block treatment.
Financial Support and Sponsorship
Nil.
Conflicts of Interest
There are no conflicts of interest.
| References | | |
| 1. | Springate SD. A re-investigation of the relationship between head posture and craniofacial growth. Eur J Orthod 2012;34:397-409.  |
| 2. | Festa F, Tecco S, Dolci M, Ciufolo F, Di Meo S, Filippi MR, et al. Relationship between cervical lordosis and facial morphology in Caucasian women with a skeletal Class II malocclusion: A cross-sectional study. Cranio 2003;21:121-9. |
| 3. | D′Attilio M, Caputi S, Epifania E, Festa F, Tecco S. Evaluation of cervical posture of children in skeletal Class I, II, and III. Cranio 2005;23:219-28. |
| 4. | Ohnmeiss M, Kinzinger G, Wesselbaum J, Korbmacher-Steiner HM. Therapeutic effects of functional orthodontic appliances on cervical spine posture: A retrospective cephalometric study. Head Face Med 2014;10:7. |
| 5. | D′Attilio M, Epifania E, Ciuffolo F, Salini V, Filippi MR, Dolci M, et al. Cervical lordosis angle measured on lateral cephalograms; findings in skeletal Class II female subjects with and without TMD: A cross sectional study. Cranio 2004;22:27-44. |
| 6. | Tecco S, Farronato G, Salini V, Di Meo S, Filippi MR, Festa F, et al. Evaluation of cervical spine posture after functional therapy with FR-2: A longitudinal study. Cranio 2005;23:53-66. |
| 7. | Baccetti T, Franchi L, Toth LR, McNamara JA Jr. Treatment timing for Twin-block therapy. Am J Orthod Dentofacial Orthop 2000;118:159-70. |
| 8. | Giuntini V, Vangelisti A, Masucci C, Defraia E, McNamara JA Jr., Franchi L. Treatment effects produced by the Twin-block appliance vs the forsus fatigue resistant device in growing Class II patients. Angle Orthod 2015;85:784-9. |
| 9. | Siersbaek-Nielsen S, Solow B. Intra- and interexaminer variability in head posture recorded by dental auxiliaries. Am J Orthod 1982;82:50-7. |
| 10. | Sidlauskas A. The effects of the Twin-block appliance treatment on the skeletal and dentoalveolar changes in Class II Division 1 malocclusion. Medicina (Kaunas) 2005;41:392-400. |
| 11. | Yagci A, Uysal T, Usumez S, Orhan M. Rapid maxillary expansion effects on dynamic measurement of natural head position. Angle Orthod 2011;81:850-5. |
| 12. | Solow B, Tallgren A. Dentoalveolar morphology in relation to craniocervical posture. Angle Orthod 1977;47:157-64. |
| 13. | Graber T. Implementation of the roentgenographic cephalometric technique. Am J Orthod 1958;44:906-32. |
| 14. | Korbmacher H, Eggers-Stroeder G, Koch L, Kahl-Nieke B. Correlations between dentition anomalies and diseases of the of the postural and movement apparatus - A literature review. J Orofac Orthop 2004;65:190-203. |
[Figure 1]
[Table 1], [Table 2], [Table 3]
|












 Search Pubmed for
Search Pubmed for