|


 |
| CASE REPORT |
|
| Year : 2011 | Volume
: 3
| Issue : 1 | Page : 52-55 |
|
|
Management of maternofetal emergency in shock with fracture of femur
Pradeep K Singh1, Deepti Shrivastva2, Snigdha Paddalwar3, Nagraj Shetty1, Vipin Raut1, Sarthak Patnaik1, Abhishek Yadav1
1 Department of Orthopaedics and Trauma, DMIMS, Wardha, India
2 Department of Obstetrics and Gynecology, DMIMS, Wardha, India
3 Department of Anesthesiology, DMIMS, Wardha, India
| Date of Web Publication | 30-Mar-2011 |
Correspondence Address:
Pradeep K Singh
Department of Orthopaedics and Trauma, Jawahar Lal Nehru Medical College and Acharya Vinoba Bhave Rural Hospital, DMIMS, Wardha 442 004
India
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.78477

 Abstract Abstract | | |
Trauma is the leading nonobstetric cause of maternal death. The worst complication can be fetal compromise that threatens premature labor or even fetal death. We are reporting a case of a 30-year-old primi, short stature woman who had fracture femur with hypovolaemic shock. Managing such trauma complicated by shock in a pregnant patient needs multidisciplinary approach. Clinician team evaluating and coordinating the care of pregnant trauma patient should understand the pathophysiological changes in pregnancy with trauma to manage hypovolaemic shock, related complications, treatment of fracture, and radiation exposure to the fetus. The use of imaging studies, invasive hemodynamics and surgery, if necessary, should be individualized. A clear understanding of fetal viability, physiological changes of pregnancy, and pathophysiology of shock, is mandatory for optimal, maternal functional, and obstetrical outcome. Keywords: Fracture femur, ionizing, pregnancy, radiation, trauma
How to cite this article:
Singh PK, Shrivastva D, Paddalwar S, Shetty N, Raut V, Patnaik S, Yadav A. Management of maternofetal emergency in shock with fracture of femur. J Surg Tech Case Report 2011;3:52-5 |
How to cite this URL:
Singh PK, Shrivastva D, Paddalwar S, Shetty N, Raut V, Patnaik S, Yadav A. Management of maternofetal emergency in shock with fracture of femur. J Surg Tech Case Report [serial online] 2011 [cited 2016 Jun 12];3:52-5. Available from: http://www.jstcr.org/text.asp?2011/3/1/52/78477 |
| Introduction | |  |
Trauma is one of the leading nonobstetric cause of maternal death in as many as 8% of pregnancies. [1] The principal causes of trauma in pregnancy include motor vehicle accidents. Domestic falls, domestic violence, and penetrating wounds are involved in 10% of trauma during pregnancy. [1] Paucity of literature about trauma and pregnancy makes it more debatable regarding anesthetic, obstetric, and surgical management of pregnant trauma victims. [2],[3] The difficulty level in the management of trauma victims with pregnancy increases from elective to emergent situations. [2] Moreover, diagnosis and treatment of fractures in pregnant patients has its own peculiar risk of exposing fetus to ionizing radiation during X-ray evaluation and image-intensifier-guided treatment, which may lead to abnormal embryogenesis and congenital anomaly. [4] Nonoperative modality for fracture femur has its own shortcomings and high complicated outcome. Deep vein thrombosis, malunion, and poor functional outcome are usual complications when treated conservatively. Very few cases of fracture shaft femur with pregnancy have been mentioned in literature. We feel that emergency clinical condition poses challenges for resuscitation team initially then surgeon who will be managing fracture and radiation exposure perioperatively and finally obstetrician who would be counseling and managing such stressed patients. The purpose of reporting this case is for better understanding of trauma management in pregnant women and to demonstrate usefulness of modified fixation technique of the fracture in pregnant woman to reduce excessive radiation.
| Case Report | | |
A 30-year-old female with short stature of 143.5 cm presented at 24-week gestation of pregnancy with fracture right femur. She was brought to the accident and emergency department with signs of hypovolaemic shock. She had cold clammy periphery with systolic blood pressure of 60 mmHg. Primary management and initial interventions were the ''ABCs'': airway, breathing, and circulation. Her airway was patent and breathing was labored. Nasal oxygen was started immediately. She was resuscitated with volume and blood transfusion. Fetal wellbeing was assured with ultrasonography thereafter. On examination of abdomen uterine fundus was palpable just above the level of the umbilicus. Ultrasonography confirmed a gravid uterus of 24 weeks gestational age, with fetal heart rate of 130 per minute. Primary X-ray taken after shielding the abdomen, revealed a displaced comminuted fracture of her right upper third of femur [Figure 1]. Her packed cell volume was 50% (hemoglobin concentration was 7.2 g/dl). Electrolytes and urea, and fasting blood sugar levels were normal. Her TORCH, HIV, and HBsAg status was normal. She denied any history of bleeding diathesis. Her Ante Natal Check up record showed fetal wellbeing. Patient and her relatives were counseled regarding management and its outcome stressing upon the radiation exposure and its subsequent sequel. | Figure 1: Preoperative radiograph of a 30-year old women who sustained trauma showing comminuted fracture of femur, primarily splinted
Click here to view |
Perioperative events
Hematologic and coagulation studies (platelet count, prothrombin time, and partial thromboplastin time) were normal. Patient was kept nil by mouth for 4 h with IV fluids supplements. She was given antiemetic and antacid as aspiration prophylaxis. The patient was positioned on Watson Jones table in a modified supine position tilting 20º toward left side to prevent hypotension by avoiding aortocaval compression due to gravid uterus.
All standard monitors were placed. The patient was given supplemental oxygen via a nasal cannula at a rate of 5 l/min. An epidural anesthesia was preferred over general anesthesia and spinal anesthesia. After giving 500 ml of ringer lactate as preload epidural anesthesia was instituted with 12 ml of 0.5% bupivacaine. Spinal anesthesia was avoided to prevent profound loss of sympathetic tone causing sudden hypotension and bradycardia. Third generation cephalosporin was given intravenously as prophylactic antibiotics.
Operative procedure
The patient was placed in supine position on a Watson Jone's fracture table under epidural anesthesia. Conventional cleaning and draping of operative site was done. Abdomen was covered with lead sheet from all around to avoid radiation exposure. Entry site for nail was obtained by locating the piriform fossa with the gloved finger and an awl was used to gain access to the proximal end of the intramedullary canal. Limited shots of fluoroscopy were used to locate entry point of nail. A blunt tipped 2 mm guide wire was introduced into the proximal fragment. Closed reduction of fracture was done with help of guarded fluoroscopy. Guide wire was advanced to the distal fragment. The intramedullary canal was reamed over the guide wire with hand-held, hollow reamers to size 10. Interlock Intramedullary nail size 9 mm/34 cm was inserted over the guide wire. Distal interlocking holes were localized by keeping same size nail externally over lateral aspect of thigh. An incision was made to expose lateral cortex of the distal femur. Lateral cortex was drilled after confirming the localized distal holes of the nail. Then a 2 mm K wire was passed through the cortex and distal interlock hole of the nail. Position of the K wire in the hole was checked by putting guide wire which should abut K wire in the hole. Then distal locking bolt was put after drilling both the cortices across the hole with K wire. Position of bolt was again checked with the help of a guide wire that abutted at the interlock bolts producing an audible and palpable metallic sound. Proximal locking was done using Jig. Postoperative radiograph showed good reduction and implant position [Figure 2]. Intra and postoperatively patient's vitals were stable. Blood loss was minimum.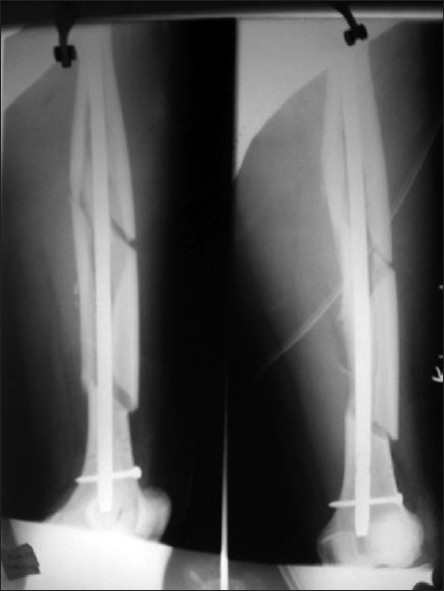 | Figure 2: Postoperative radiograph shows fixation of fracture with closed intramedullary interlocking nail
Click here to view |
We protected the patient and the fetus from radiation exposure by draping a lead sheet over her abdomen. Excess radiation exposure was prevented by using minimum number of shots of image intensifier as distal interlocking was done without fluoroscopy. Postoperative recovery was uneventful and she was discharged for home on fourth postoperative day with prescribed physiotherapy. She recovered and rehabilitated satisfactorily as radiograph revealed signs of union. Obstetrician delivered the baby by doing elective caesarean section at completion of 39 weeks of gestation. Baby and mother were normal at the time of discharge from the obstetrics ward.
| Discussion | | |
Trauma in pregnancy is currently a leading cause of nonobstetrical maternal death and maternal death remains the most common association of fetal demise. [1],[5],[6] The most common etiology of trauma in pregnancy includes motor vehicle accident, fall, assault, and other injuries. [1] Women of childbearing age are at greater risk for trauma. [6]
The anatomic and physiologic changes of pregnancy such as increased oxygen demand, altered pulmonary function, and full stomach may increase the difficulty of perioperative management, when mother and fetus need utmost prompt treatment action. The pregnant trauma victim presents a unique spectrum of challenges to the trauma healthcare team. The piece of information may not be known to the health care team (at the scene of transportation accidents, in the emergency room, or in the operating room) additionally complicates the situation.
Modern orthopedics advocates operative management of fracture femur and mobilization of patient as early as possible. However, for better obstetrical care, good functional outcome of the limb is mandatory. Constant worry and hesitation on behalf of surgeon to use radiation in a pregnant woman makes them to limit the number of exposures during surgery which can adversely affect the course of procedure. Perioperative challenges for the surgeon and anesthesiologist includes risk of induced abortion and radiation related hazards to the fetus. In radiographic studies such as plain film X-ray, computed tomography, and angiography the uterus should be shielded to avoid radiation exposure. [7]
Femoral interlocking nail, most of the radiation exposure occurs during distal interlocking nailing, making entry portal for the nail at piriform fossa, and closed reduction and guide wire negotiation across the fracture site. [8] Locking of femoral nail requires more fluoroscopic time (7.60 min) as compared to femoral nail without interlocking (1.33 min). [8] This extra fluoroscopic time for locking of femoral nail carries greater significance when radiation hazards to the fetus of pregnant woman are major concern. There are techniques in literature that demonstrates distal interlocking of femoral nail without the use of fluoroscopy. [9] We can reduce radiation while distal interlocking bolt as we did in present case. Retrograde femoral nailing is a viable option in order to reduce radiation while making entry portal and distal locking. It has been studied that amount of radiation exposed for making entry point in retrograde nailing is far less than antegrade nailing. [10] However, fracture of femur in pregnant woman is now considered as relative indication for retrograde femoral nailing owing to less amount of radiation exposure involved. [10],[11] Rationale of implant selection in similar clinical meeting should include level and type of fracture. However, we could not chose retrograde nail in our case as length of the nail was constrain because fracture was in upper third of the femur.
Maximal permissible ionizing radiation from X-rays for limb is 100 mGy units. Exposure beyond 100 mGy may cause cancerous or noncancerous effects on fetus during first trimester of pregnancy. Noncancerous effects on the embryo or fetus include miscarriage, fetal growth restriction, congenital malformation, mental retardation. [5],[12] However, radiation-induced noncancerous health effects are not detectable for fetal doses below 50 mGy (1 mGy = 100 mrad). [13] Though some amount of mental retardation and loss of IQ (approximately 13--21) may occur if pregnancy is exposed to radiation in second trimester. [14] Surprisingly, the estimation of radiation dose in fluoroscopic-guided orthopedics procedure and consequences has not been elaborated clearly in literature. Ioannis et al, estimated entrance surface dose by using mathematical method for interlocking femoral nailing. [15] Furthermore, probability of scattered radiation will be approximately 24 times less behind the lead screen. [8] Thus the use of lead sheet as drape in a pregnant woman reduces the chance of direct and scattered radiation to the fetus. Modification of operative technique can further reduce amount of radiation exposure to the pregnant patient.
In summary trauma in pregnant women requires early intervention at all stages. Aggressive multidisciplinary approach is the safest way to save two lives. Modification of surgical technique can be practiced in similar clinical setting to reduce amount of radiation to the fetus.
| References | | |
| 1. | D′Amico CJ. Trauma in pregnancy. Top Emerg Med 2002;24:26-39. 
|
| 2. | Kuczkowski KM, Ispirescu JS, Benumof JL. Trauma in pregnancy: Anesthetic management of the parturient with multiple gun shot wounds to the gravid uterus and fetal injury. J Trauma 2003;54:420.
[PUBMED] [FULLTEXT] |
| 3. | Daponte A, Khan N, Smith MD, Gegiannis E. Trauma in pregnancy. S Afr J Surg 2003:41:51-4.
|
| 4. | An excellent and comprehensive review of surgical management of the pregnant trauma patient. In: Valentin J, editor, Annals of the ICRP, Publication 84: Pregnancy and Medical Radiation, International Commission on Radiological Protection. Vol. 30. Pergamon, Tarrytown, New York: Elsevier Science, Inc.; 2000. p. 1.
|
| 5. | Baker BW. Trauma. In: Chestnut DH, editor. Obstetric Anesthesia: Principles and Practice. Mosby: St. Louis; 1999. p. 1041-50.
|
| 6. | El-Kady D, Gilbert WM, Anderson J, Danielsen B, Towner D, Smith LH, et al. Trauma during pregnancy: An analysis of maternal and fetal outcomes in a large population. Am J Obstet Gynecol 2004;190:1661-8.
[PUBMED] [FULLTEXT] |
| 7. | Barraco RD, Chiu WC, Clancy TV, Como JJ, Ebert JB, Hess LW, et al. Practice management guidelines for the diagnosis and management of injury in the pregnant patient: The EAST practice management guidelines work group. J Taruma 2010;69:211-4. Chicago: Eastern Association for the Surgery of Trauma. Available from: http://www.east.org/tpg/pregnancy.pdf. [Last accessed on 2005].
|
| 8. | Lo NN, Goh PS, Khong KS. Radiation dosage from use of the image intensifier in orthopaedic surgery. Singapore Med J 1996;37:69-71.
[PUBMED] |
| 9. | Kanellopoulos AD, Yiannakopoulos CK, Vossinakis L, Badras LS. Distal locking of femoral nails under direct vision through a cortical window. J Ortho Trauma 2003;17:574-7.
|
| 10. | Moed BR, Watson JT. Retrograde nailing of the femoral shaft. J Am Acad Orthop Surg 1999;7:209-16.
[PUBMED] [FULLTEXT] |
| 11. | Ostrum RF, DiCicco J, Lakatos R, Poka A. Retrograde intramedullary nailing of femoral diaphyseal fractures. J Orthop Trauma 1998:12:464-8.
|
| 12. | Brent RL, Gorson RO. Radiation exposure in pregnancy. In: Current Problems in Radiology. Technic of pneumoencephalography. Chicago: Year Book Medical; 1972. p. 1-47.
|
| 13. | Prenatal Radiation Exposure: A Fact Sheet for Physicians (CDC) Available from: http://www.bt.cdc.gov/radiation/prenatalphysician.asp [Last accessed on 2010 Aug 21].
|
| 14. | Kramer MS. Determinants of low birth weight: Methodological assessment and meta-analysis. Bull World Health Organ 1987;65:663-737.
[PUBMED] [FULLTEXT] |
| 15. | Tsalafoutas IA, Tsapaki V, Kaliakmanis A, Pneumaticos S, Tsoronis F, Koulentianos ED, et al. Estimation of radiation doses to patients and surgeons from various fluoroscopically guided orthopaedic surgeries Radiat Prot Dosimetry 2008;128:112-9.
|
[Figure 1], [Figure 2]
|
















