|


 |
| SURGICAL TECHNIQUE |
|
| Year : 2012 | Volume
: 4
| Issue : 1 | Page : 19-21 |
|
|
Flap hitching technique to the teeth after oral cancer resection
Krishnakumar Thankappan1, Subramania Iyer1, Mayuri Rajapurkar1, Mohit Sharma1, Pramod Subash2
1 Department of Head and Neck Surgery, Amrita Institute of Medical Sciences, Kochi, Kerala, India
2 Mazumdar Shaw Cancer Center, Bangalore, Karnataka, India
| Date of Web Publication | 5-Sep-2012 |
Correspondence Address:
Krishnakumar Thankappan
Associate Professor, Head and Neck Institute, Amrita Institute of medical Sciences, Kochi, Kerala
India
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.100347

 Abstract Abstract | | |
Objectives: After resection of the tumors of oral cavity adjacent to the mandible, it is a common situation that the whole of one side of the gingival mucosal segment has to be stripped off the mandible to get an adequate margin. When a cutaneous flap is used for reconstruction, it has to be hitched to the teeth to get a watertight seal. We describe a technique to hitch the flap to the adjacent teeth in such an instance. Materials and Methods: The technique was applied in 10 patients with oral cancer, resected, and reconstructed with cutaneous flaps. Results: The technique was found to be effective in all 10 patients. Adequate seal was obtained in all patients. Oral diet was started within 7 days. Conclusion: An effective and simple technique to approximate a cutaneous flap to the teeth-bearing mandible, when all the mucosa is removed as part of oncological resection, is reported. Keywords: Free flap, flap-hitching stich, head and neck cancers, oral cancer, reconstruction
How to cite this article:
Thankappan K, Iyer S, Rajapurkar M, Sharma M, Subash P. Flap hitching technique to the teeth after oral cancer resection. J Surg Tech Case Report 2012;4:19-21 |
How to cite this URL:
Thankappan K, Iyer S, Rajapurkar M, Sharma M, Subash P. Flap hitching technique to the teeth after oral cancer resection. J Surg Tech Case Report [serial online] 2012 [cited 2016 Jun 10];4:19-21. Available from: http://www.jstcr.org/text.asp?2012/4/1/19/100347 |
| Introduction | |  |
Flap surgery for reconstruction is an integral part in the surgical management of head and neck tumors. After resection of the tumors of oral cavity adjacent to the mandible, but not requiring a marginal mandibulectomy (tumors of the tongue, on the labial side, and tumors of the buccal mucosa on the buccal aspect), it is a common surgical situation that the whole of one side of the gingival mucosal segment has to be stripped of the mandible to get an adequate margin [Figure 1]. The mucosa on the other side of the mandible in these situations is usually intact. When a cutaneous flap is used for reconstruction, either a pedicled flap like pectoralis major myocutaneous flap or a free flap like radial forearm flap, it has to be hitched to the teeth with a watertight seal to prevent a fistula into the neck. There may not be a mucosal fringe attached to the mandible in many instances. We describe a technique to hitch the flap to the adjacent teeth in such an instance. An informed consent was given by the patient for publishing this article and the photographs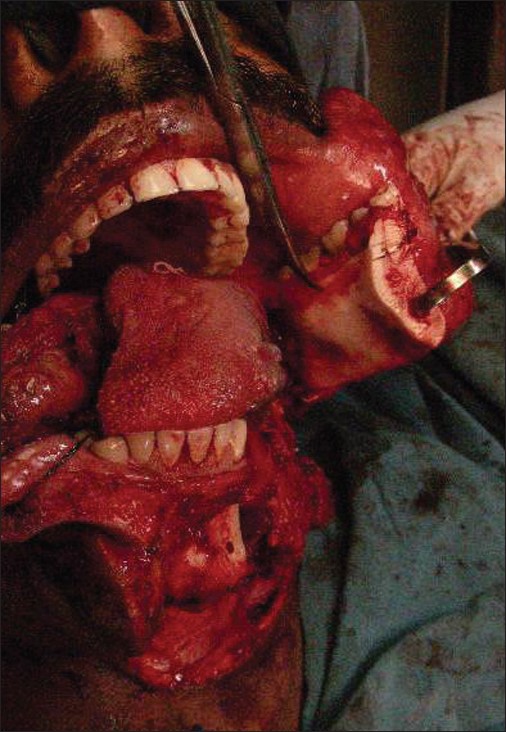 | Figure 1: Intraoperative photograph showing the mandible where the gingival mucosa is removed as part of the margin of resection
Click here to view |
| Surgical Technique | | |
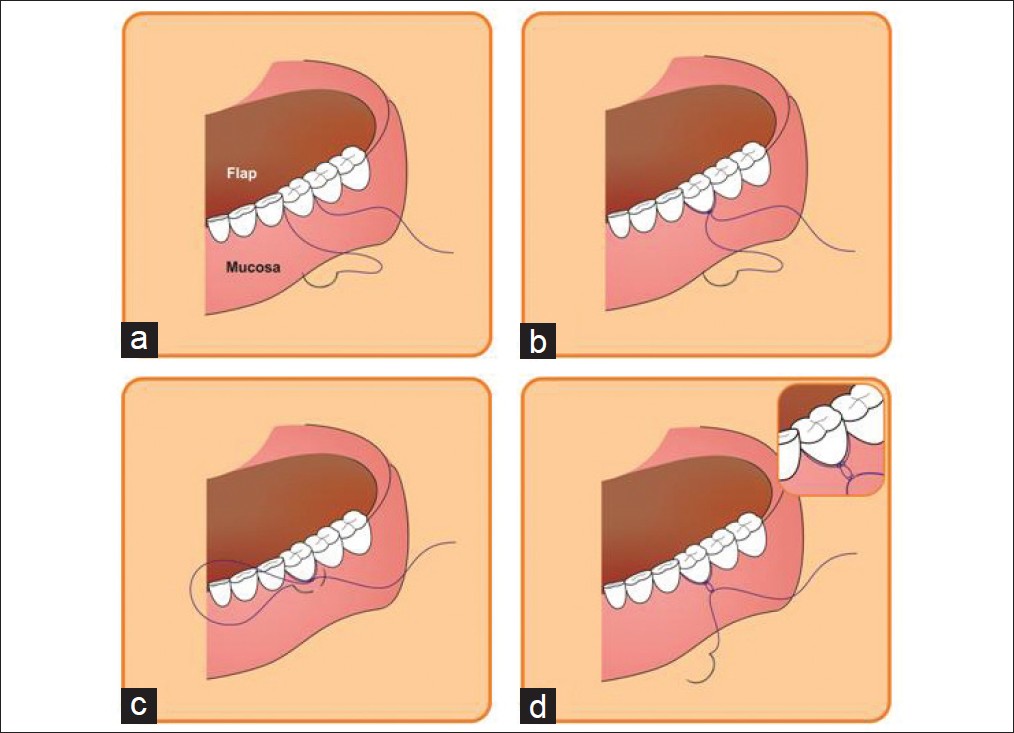
2-0 polypropylene suture with 26 mm ½ C taper-cut needle is passed, from the side with the retained mucosa, between two teeth, through the intergingival papilla. [Figure 2]a This needle has the adequate curvature allowing an easy pass between the teeth space. A taper-cut needle is preferred as it allows the tougher penetration through the skin of the flap. Once through to the side without the mucosa, a bite is taken through the flap and then coming out through the adjacent space, passing out again through the intergingival papilla. A knot is then made on the side with the retained mucosa, making sure that the suture lies along the neck of the tooth. [Figure 2]b This first loop around the neck of the tooth holds the flap firmly against the mandible and the tooth. As a next step, another bite is taken through the gingival mucosa adjacent to the knot [Figure 2]c and a second ligature is made. This second knot prevents the slipping of the suture from the tooth [Figure 2]d. Multiple such stitches may have to be taken corresponding to each tooth, depending upon the length of the defect with absent mucosa adjacent to the mandible [Figure 3]. 2-0 polypropylene material is used for adequate strength for the stay around the tooth. But this has to be removed later per-orally after proper healing. [Figure 4] shows the final outcome after 6 months.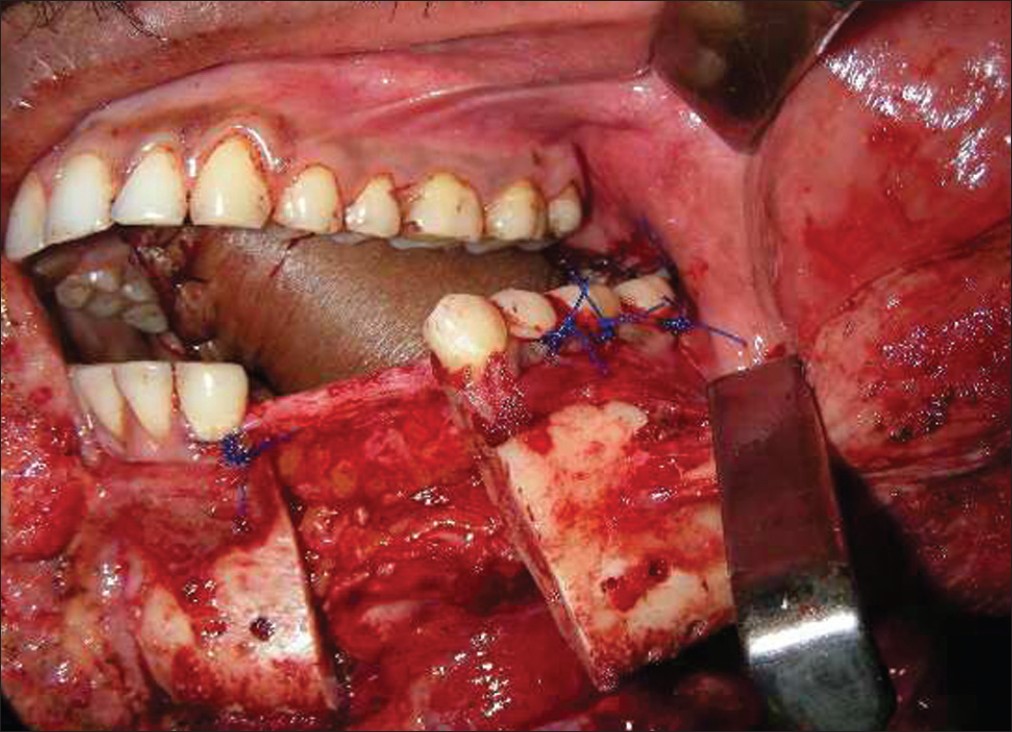 | Figure 3: Intraoperative photograph showing the stitches taken on multiple adjacent teeth
Click here to view |
The technique described was used in 10 patients. Four patients had tongue or floor of the mouth primary adjacent to the buccal side of the mandible. Five patients had a buccal mucosal lesion adjacent to the mandible and two other patients had buccal mucosal primary adjacent to the maxillary alveolus. A firm and watertight closure could be achieved in all patients. None of the patients developed fistula into the neck. Oral diet was started within 7 days.
| Discussion | | |
Oncological resection usually includes a rim of normal tissue around the tumor. A marginal mandibulectomy [1],[2] is required to get an adequate clearance for the tumor of the oral cavity abutting the mandible but not involving it. But many a time, when there is at least a centimeter of uninvolved mucosa between the tumor and the mandible, the gingival mucosa can be stripped of the mandible to get an adequate clearance without including a part of the mandible bone. This can occur in the case of a tumor arising from the buccal mucosa, floor of the mouth or a tongue tumor involving the floor of the mouth. Reconstruction after resection in oral cavity tumors usually requires cutaneous flaps. [2] Free flaps [3] or pedicled myocutaneous flaps [4] are commonly used. In these instances, the flap has to be hitched to the adjacent teeth to get an adequate seal. Surgical textbooks do not describe a technique of doing this nor could a literature search find one. The reported technique was used in 10 patients of oral cavity tumors who required flap reconstruction and was found to be useful. The commonly done technique of hitching the flap is with a single loop around the tooth and a single knot. Our technique is innovative in the second bite on the adjacent mucosa and the knot which prevents the slipping of the suture from the tooth.
| Conclusion | | |
An effective and simple technique to approximate a cutaneous flap to the teeth-bearing mandible, when all the mucosa is removed as part of oncological resection, is reported.
| References | | |
| 1. | Pathak KA, Shah BC. Marginal mandibulectomy: 11 years of institutional experience. J Oral Maxillofac Surg 2009;67:962-7. 
[PUBMED] |
| 2. | Shah JP, Gil Z. Current concepts in management of oral cancer-surgery. Oral Oncol 2009;45:394-401.
[PUBMED] |
| 3. | Wong CH, Wei FC. Microsurgical free flap in head and neck reconstruction. Head Neck 2010;32:1236-45.
[PUBMED] |
| 4. | Pinto FR, Malena CR, Vanni CM, Capelli Fde A, de Matos LL, Kanda JL. Pectoralis major myocutaneous flaps for head and neck reconstruction: Factors influencing occurrences of complications and the final outcome. Sao Paulo Med J 2010;128:336-41.
[PUBMED] |
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
|