|


 |
| SHORT TECHNIQUE |
|
| Year : 2012 | Volume
: 4
| Issue : 1 | Page : 22-23 |
|
|
A simple technique for safe mesenteric defect closure following bowel resection
Yahya A Al Abed, Kevin Lafferty, Vasilis Kosmoliaptsis
Department of General Surgery, Basildon and Thurrock University Hospitals, Essex SS16 5NL, United Kingdom
| Date of Web Publication | 5-Sep-2012 |
Correspondence Address:
Yahya A Al Abed
Department of General Surgery, Basildon and Thurrock University Hospitals, Essex SS16 5NL
United Kingdom
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.100348

 Abstract Abstract | | |
The closure of the mesenteric defect following bowel resection remains controversial. Proponents of the intervention cite the risk of bowel herniation through an open mesenteric defect and subsequent bowel obstruction whereas supporters of the opposing view advocate that such practice may lead to inadvertent compromise of the bowel blood supply. We describe a novel technique that enables efficient mesenteric defect closure while minimizing the risk of blood vessel injury. Keywords: Closure, mesenteric defect, bowel resection
How to cite this article:
Al Abed YA, Lafferty K, Kosmoliaptsis V. A simple technique for safe mesenteric defect closure following bowel resection. J Surg Tech Case Report 2012;4:22-3 |
How to cite this URL:
Al Abed YA, Lafferty K, Kosmoliaptsis V. A simple technique for safe mesenteric defect closure following bowel resection. J Surg Tech Case Report [serial online] 2012 [cited 2016 Jun 10];4:22-3. Available from: http://www.jstcr.org/text.asp?2012/4/1/22/100348 |
| Introduction | |  |
The closure of the mesenteric defect following bowel resection has traditionally been undertaken, especially in open surgery, in an attempt to prevent bowel herniation and subsequent strangulation. With the advent of laparoscopic surgery however, the value of this practice has been challenged and many surgeons do not routinely close the resultant mesenteric defect following laparoscopic bowel resection. Proponents of the former approach point to the risk of small bowel herniation through an open mesenteric defect, potentially leading to bowel obstruction and rarely to catastrophic mesenteric ischemia. [1] In support of this argument, several case studies have reported complications attributed to the nonclosure of the mesenteric defect; interestingly, these studies often relate to laparoscopy-assisted colostomies. [2],[3],[4],[5] Conversely, opponents of the mesenteric defect closure advocate that such practice may result in the constriction of the bowel mesentery, inadvertent ligation of blood vessels and/or mesenteric hematoma formation and could, therefore, compromise the blood supply to the bowel anastomosis and lead to anastomotic dehiscence. [6],[7] Here we propose a simple technique, applicable to both open and laparoscopy-assisted colectomies, that enables a quick closure of the mesenteric defect while minimizing the risk of blood vessel injury.
| Technique | | |
Following bowel resection, the ligatures used for mesenteric vessel ligation are left long [Figure 1]. Once the bowel anastomosis is completed, the long ligatures on either side of the mesenteric defect are tied together closing the defect [Figure 2]. The ties are subsequently cut. Placement of extra sutures is not routinely required.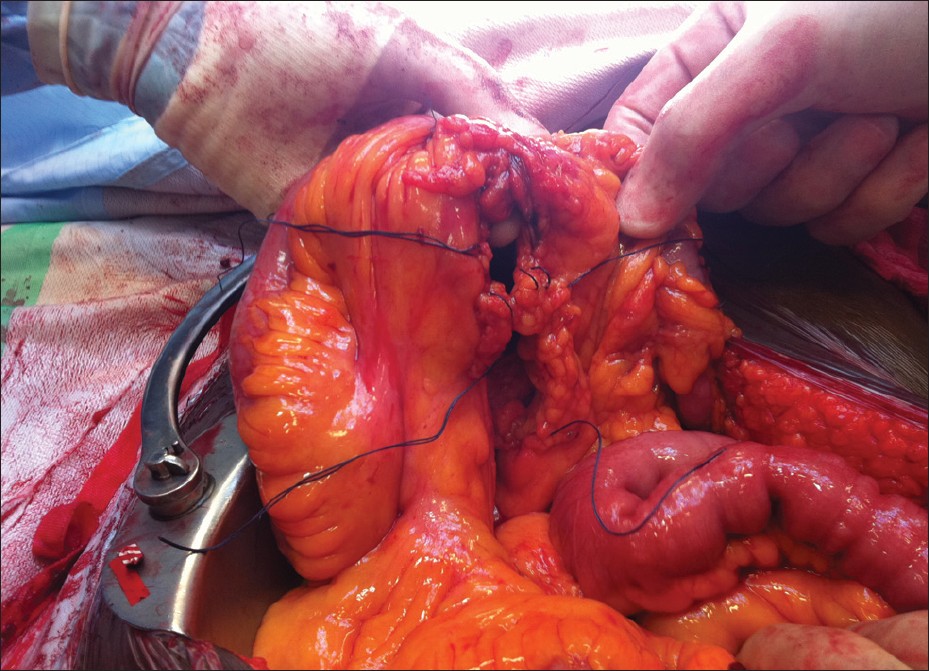 | Figure 1: Following bowel resection, mesenteric vessels are ligated and the ligatures are left long
Click here to view |
 | Figure 2: Long ligatures on either side of the mesenteric defect are tied together closing the defect
Click here to view |
| Discussion | | |
The handling of the mesenteric defect following bowel resection remains a subject of debate. Unfortunately, there is paucity of high-quality data to inform surgical practice on this topic with much of the available evidence based on case reports and nonrandomized, observational studies. This report describes a simple technique that enables the closure of the mesenteric defect while minimizing the risk of inadvertent damage to the blood vessels supplying the bowel anastomosis. Our mesenteric defect closure technique represents an alternative to those previously reported in the literature, such as stapled closure or closure using a continuous running suture, [8],[9] and is currently being evaluated in a prospective study undertaken in our unit.
| References | | |
| 1. | Sereno Trabaldo S, Anvari M, Leroy J, Marescaux J. Prevalence of internal hernias after laparoscopic colonic surgery. J Gastrointest Surg 2009;13:1107-10. 
[PUBMED] |
| 2. | Elio A, Veronese E, Frigo F, Residori C, Salvato S, Orcalli F. Ileal volvulus on internal hernia following left laparoscopic-assisted hemicolectomy. Surg Laparosc Endosc 1998;8:477-8.
[PUBMED] |
| 3. | Hosono S, Ohtani H, Arimoto Y, Kanamiya Y. Internal hernia with strangulation through a mesenteric defect after laparoscopy-assisted transverse colectomy: Report of a case. Surg Today 2007;37:330-4.
[PUBMED] |
| 4. | Jimi S, Hotokezaka M, Eto TA, Hidaka H, Maehara N, Matsumoto K, et al. Internal herniation through the mesenteric opening after laparoscopy-assisted right colectomy: Report of a case. Surg Laparosc Endosc Percutan Tech 2007;17:339-41.
[PUBMED] |
| 5. | Kawamura YJ, Sunami E, Masaki T, Muto T. Transmesenteric hernia after laparoscopic-assisted sigmoid colectomy. JSLS 1999;3:79-81.
[PUBMED] |
| 6. | Causey MW, Oguntoye M, Steele SR. Incidence of complications following colectomy with mesenteric closure versus no mesenteric closure: Does it really matter? J Surg Res 2011;171:571-5.
[PUBMED] |
| 7. | Cabot JC, Lee SA, Yoo J, Nasar A, Whelan RL, Feingold DL. Long-term consequences of not closing the mesenteric defect after laparoscopic right colectomy. Dis Colon Rectum 2010;53:289-92.
[PUBMED] |
| 8. | Coleman MH, Awad ZT, Pomp A, Gagner M. Laparoscopic closure of the Petersen mesenteric defect. Obes Surg 2006;16:770-2.
[PUBMED] |
| 9. | Cohen SM, Clem MF, Wexner SD, Jagelman DG. An initial comparative study of two techniques of laparoscopic colonic anastomosis and mesenteric defect closure. Surg Endosc 1994;8:130-4.
[PUBMED] |
[Figure 1], [Figure 2]
|















