|


 |
| CASE REPORT |
|
| Year : 2012 | Volume
: 4
| Issue : 2 | Page : 112-114 |
|
|
Follicular Thyroid Carcinoma Presenting as Massive Skull Metastasis: A Rare Case Report and Literature Review
Sanjay N Koppad, Vaibhav B Kapoor
Department of General Surgery, Rural Medical College, Pravara Medical Trust, Loni, Maharashtra, India
| Date of Web Publication | 8-Apr-2013 |
Correspondence Address:
Sanjay N Koppad
Department of General Surgery, Rural Medical College, Pravara Medical Trust, Loni, Rahata, Ahmednagar, Maharashtra
India
 Source of Support: None, Conflict of Interest: None  | 3 |
DOI: 10.4103/2006-8808.110252

 Abstract Abstract | | |
Follicular carcinoma of thyroid is a well differentiated thyroid malignancy. It is slow growing in nature and tends to metastasize to remote organs in advanced stage by hematogenous route. Lung and bone are the two most common sites of metastasis. In most of the reported cases of follicular thyroid carcinoma metastasizing to the skull, metastases occurred long after the diagnosis and institution of treatment for primary cancer. Very few cases have been reported with occult follicular thyroid carcinoma presenting as skull metastasis. A 48-year-old female patient presented with massive swelling in the frontal region of skull associated with swellings in occipital region. Evaluation confirmed that it is multiple metastases to skull bones from follicular thyroid carcinoma. This is a very rare presentation with such a large size of metastasis. We report this case of a metastatic follicular thyroid carcinoma presenting as massive skull tumor at our institution. Keywords: Follicular thyroid carcinoma, radio iodine, skull metastasis, thyroid malignancy
How to cite this article:
Koppad SN, Kapoor VB. Follicular Thyroid Carcinoma Presenting as Massive Skull Metastasis: A Rare Case Report and Literature Review. J Surg Tech Case Report 2012;4:112-4 |
How to cite this URL:
Koppad SN, Kapoor VB. Follicular Thyroid Carcinoma Presenting as Massive Skull Metastasis: A Rare Case Report and Literature Review. J Surg Tech Case Report [serial online] 2012 [cited 2016 Jun 10];4:112-4. Available from: http://www.jstcr.org/text.asp?2012/4/2/112/110252 |
| Introduction | |  |
Metastatic tumors to skull are most often from lung, breast, and prostate malignancies and rarely from thyroid cancers. In a series of 473 patients with thyroid cancers, Nagamine et al. reported skull metastases in only 2.5% of cases. [1] In most of the reported cases of follicular thyroid carcinoma, metastases occurred long after institution of treatment for primary cancer. There have been only a handful of cases reported in literature with skull metastasis as the presenting feature of an occult follicular thyroid carcinoma. [2],[3],[4] We report a 48-year-old female presenting with massive skull metastasis from follicular thyroid carcinoma.
| Case Report | | |
A 48-year-old female presented with swelling in the frontal region of the skull since 2 years and another swelling in parieto-occipital region since 4 months. Both the swellings over skull have been painless and gradually progressive in size, thus the delay in presentation. No significant past medical history. On examination, swelling in frontal region measured 18 cm in sagital and 13 cm in coronal directions and 7 cm in vertical dimension. The veins over swelling were distended and it was pulsatile in nature, firm in consistency and fixed to skull. The skin over the swelling was stretched but otherwise normal. Left orbit appeared distorted by the swelling but vision was normal [Figure 1]. The second swelling was located in parieto-occipital region right side and measured 3×4 cm pulsatile in nature and firm in consistency [Figure 2]. Incidentally a thyroid swelling was noted involving mainly right lobe around 3×2 cm, firm and not associated with any pressure symptoms [Figure 1]. Patient did not have any neurological deficit or psychological illness. The patient was clinically euthyroid with normal general physical, systemic, and neurological examination. Routine blood tests and thyroid function tests were normal. Ultrasound study of neck revealed 2 × 1.5 cm neoplastic solid nodule in right lobe of thyroid. Rest of the thyroid gland and neck was normal. X-ray of skull showed lytic lesion in frontal and occipital region of skull. Contrast enhanced computed tomography (CT) demonstrated a 13 × 18 cm size expansile osteolytic lesion in the fronto-parietal region on both right and left side of anterior half of skull. The lesion was extending intracranialy and causing compression of the underlying fronto-parietal lobes on both sides. Similar expansile osteolytic lesion of smaller size are seen in the occipital region on both sides largest measuring 4×3 cm on right side. On postcontrast study, these lesions showed significant enhancement suggesting increased vascularity and also areas of necrosis were present at centre [Figure 3]. Fine needle aspiration cytology (FNAC) from thyroid nodule was reported as follicular neoplasm. FNAC from skull swelling obtained was stained with Leishman stain. Smears showed many syncytial sheets of thyroid follicular cells having monotonous enlarged, hyper chromatic nuclei, and microfollicles containing colloid [Figure 4]. Patient was advised total thyroidectomy and radioiodine therapy but was not willing, hence was administered supraphysiological dose of thyroxine. Till date the patient is on follow-up and able to carry out her routine activities. | Figure 1: A 13 × 18 cm metastasis follicular thyroid carcinoma in frontal region of skull swelling with distended and engorged veins suggesting increased vascularity and also showing incidentally noted 3 × 2 cm thyroid swelling the primary lesion involving right lobe of thyroid
Click here to view |
 | Figure 2: Metastasis from follicular thyroid carcinoma in right parietooccipital region of skull
Click here to view |
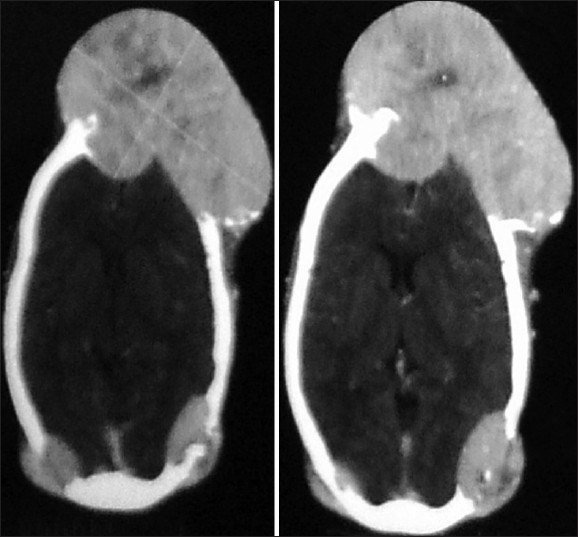 | Figure 3: CT scan showing multiple osteolytic lesions with contrast enhancement and central necrosis
Click here to view |
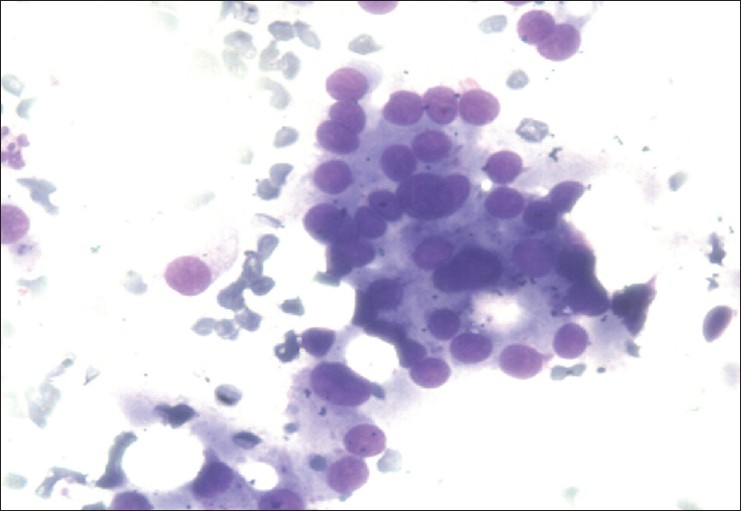 | Figure 4: FNAC from skull swelling showing presence of thyroid cells confirming the metastatic nature of swellings from follicular carcinoma thyroid
Click here to view |
| Discussion | | |
Follicular thyroid carcinoma is a subtype of thyroid cancer, which is slow growing and is associated with a good prognosis. However, in the presence of distant metastasis the prognosis is often poor. [5] Lung and bone are the two most common sites of metastases. [6] Bone metastases from follicular thyroid carcinoma tend to be multiple and more often to the ribs, vertebrae, and sternum. [7] Skull is a rare site for metastases; and if this occurs, are most commonly located in the occipital region presenting as a soft, painless lump. Presenting features of skull metastasis usually include a palpable scalp tumor, though unusual presentations with exophthalmos, disturbance of consciousness, hemiparesis, and headache have also been reported. These lesions are osteolytic on skull X-ray and CT scan and highly vascular on angiographic assessment. [1],[2] The largest case series of skull metastases from all types of thyroid cancers consists of 12 cases reported by Negamine et al. [1] In this series, mean time from the diagnosis of thyroid tumor until discovery of skull metastasis was 23.3 years. Prognosis in case of metastasis is generally poor and the 10-year survival with bone metastases from differentiated thyroid cancers is reported to be 27%. [6] However the reported mean survival in patients who present with skull metastases in the case series by Negamine et al. is only 4.5 years, suggesting that these subset of patients tend to do even worse. [1] Radioactive iodine therapy is essential to treat such metastatic disease. Lung metastases usually respond to radioactive iodine treatment. However bone metastases uncommonly respond to radioactive iodine therapy and are associated with poor prognosis [6] because of the low remission rate in radioactive iodine therapy and poor prognosis in patients with bone metastases, the surgical approach should be considered as one of the treatments of choice for bone metastasis, if possible. Curative resection of solitary bone metastasis is associated with improved survival, especially in younger patients. [7],[8]
| Conclusion | | |
It is a very unusual and rare presentation of follicular thyroid carcinoma metastasis to multiple sites in skull with such large size of metastasis from an occult primary tumor. Differential diagnosis of follicular thyroid carcinoma must be kept in mind whenever a skull bone tumor is evaluated.
| References | | |
| 1. | Nagamine Y, Suzuki J, Katakura R, Yoshimoto T, Matoba N, Takaya K. Skull metastasis of thyroid carcinoma. Study of 12 cases. J Neurosurg 1985;63:526-31. 
|
| 2. | Akdemir I, Erol FS, Akpolat N, Ozveren MF, Akfirat M, Yahsi S. Skull metastasis from thyroid follicular carcinoma with difficult diagnosis of the primary lesion. Neurol Med Chir (Tokyo) 2005;45:205-8.
|
| 3. | Ozdemir N, Senoðlu M, Acar UD, Canda MS. Skull metastasis of follicular thyroid carcinoma. Acta Neurochir (Wien) 2004;146:1155-8.
|
| 4. | Inci S, Akbay A, Bertan V, Gedikoðlu G, Onol B. Solitary skull metastasis from occult thyroid carcinoma. J Neurosurg Sci 1994;38:63-6.
|
| 5. | Cobin RH, Gharib H, Bergman DA, Clark OH, Cooper DS, Daniels GH, et al. Thyroid carcinoma task force. AACE/AAES medical/surgical guidelines for clinical practice: Management of Thyroid Carcinoma. American Association of Clinical Endocrinologists. American College of Endocrinilogy. Endocr Pract 2001;7:202-20.
|
| 6. | Schlumberger M, Tubiana M, De Vathaire F, Hill C, Gardet P, Travagli JP, et al. Long-term results of treatment of 283 patients with lung and bone metastases from differentiated thyroid carcinoma. J Clin Endocrinol Metab 1986;63:960-7.
|
| 7. | Zettinig G, Fueger BJ, Passler C, Kaserer K, Pirich C, Dudezak R, et al. Long term follow-up of patients with bone metastases from differentiated thyroid carcinoma-surgery or conventional therapy? Clin Endocrinol (Oxf) 2002;56:377-82.
|
| 8. | Bernier MO, Leenhardt L, Hoang C, Aurengo A, Mary JY, Menegaux F, et al. Survival and therapeutic modalities in patients with bone metastases ofdifferentiated thyroid carcinomas. J Clin Endocrinol Metab 2001;86:1568-73.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
| This article has been cited by | | 1 |
Thyroid follicular carcinoma presenting as metastatic skin nodules |
|
| Asad Jehangir,Ranjan Pathak,Madan Aryal,Anam Qureshi,Qasim Jehangir,Richard Alweis,Raymond Truex,William Kimmel | | Journal of Community Hospital Internal Medicine Perspectives. 2015; 5(1) | | [Pubmed] | [DOI] | | | 2 |
Propuesta de estadificación de las lesiones inflamatorias de la región frontal |
|
| Galo S. Soberón,Héctor M. Prado,Andrés Sadek,Olga Plowes,José R. Arrieta,Vladimir Figueroa | | Acta Otorrinolaringológica Española. 2015; | | [Pubmed] | [DOI] | | | 3 |
Occult papillary microcarcinoma of the thyroid presenting as large cervical node metastases |
|
| George H Sakorafas,George Goutis,Agapi Elvanidou,Konstantina K Katseni,Nena Deskoulidou,Dimitrios Thanos | | International Journal of Endocrine Oncology. 2014; 1(1): 39 | | [Pubmed] | [DOI] | |
|




 |
|
|
|











