|


 |
| CASE REPORT |
|
| Year : 2012 | Volume
: 4
| Issue : 2 | Page : 121-125 |
|
|
Arthroscopic Bullet Removal from the Acetabulum (Hip Joint)
Jamal Al-Asiri1, Ivan Wong2
1 Department of Surgery, Saudi Ministry of Higher Education, Division of Orthopaedic Surgery, McMaster University, Hamilton, Ontario, Canada
2 Department of Surgery, The Division of Orthopaedic Surgery, Dalhousie University, 1276 South Park Street, Halifax, NS B3H 2Y9, Canada
| Date of Web Publication | 8-Apr-2013 |
Correspondence Address:
Jamal Al-Asiri
34-7 Southside Place, Hamilton on Canada L9C 7W6
Canada
 Source of Support: None, Conflict of Interest: None  | 4 |
DOI: 10.4103/2006-8808.110260

 Abstract Abstract | | |
Hip arthroscopy has been shown to offer minimally invasive access to the hip joint compared with standard open arthrotomy. The use of arthroscopy for diagnosing and treating disorders about the hip continues to evolve. This study describes a case that involves arthroscopic removal of a bullet from a low-velocity gunshot wound. The patient sustained a gunshot wound that entered the abdomen and traversed the small bowel, sigmoid colon then penetrated the urinary bladder before ending up in the medial wall of the acetabulum. After surgical repair of the viscus, the bullet was retrieved from the hip joint using standard arthroscopic portals and a fracture table. A number of issues led to the decision to use arthroscopy. Most importantly was the need to minimize soft tissue dissection, which was required to access the bullet, without interfering with previous wound at the suprapubic area. The risks of potential bullet fragmentation and migration, as well as a possible abdominal compartment syndrome were considered before proceeding. Arthroscopy allowed adequate inspection of the articular surface, irrigation of the joint, and removal of the foreign body while avoiding an invasive arthrotomy with its associated morbidity and soft tissue disruption. This surgical technique afforded a very satisfactory outcome for this patient and serves as a model for others when encountering a similar injury pattern in a trauma patient. It is a procedure that can be performed safely, quickly, and with minimal complications for surgeons with experience in arthroscopy of the hip joint. Keywords: Acetabulum, arthroscopy, bullet, foreign body, gunshot, hip
How to cite this article:
Al-Asiri J, Wong I. Arthroscopic Bullet Removal from the Acetabulum (Hip Joint). J Surg Tech Case Report 2012;4:121-5 |
| Introducton | |  |
Access to the hip joint has historically been gained using an open arthrotomy. This approach typically requires a sizable dissection, which exposes the patient to considerable morbidity and requires significant recovery time. Hip arthroscopy was first described by Burman in 1931; [1] however, it has been popularized only recently, and its practical utility in diagnosing and treating hip pathology has been limited. Unlike routine arthroscopy of other major joints such as the knee and shoulder, arthroscopic techniques of the hip joint are technically more difficult. Owing to the less-accessible location and greater potential for neurologic and vascular complications, arthrotomy is often the preferred method for access to the joint. Although it was once infrequently used, many surgeons are now increasingly recognizing the potential advantages of a minimally invasive approach for treating various hip pathologies. Indications include debridement of labral tears and osteochondral lesions, synovectomy, biopsy, removal of loose bodies, and potentially staging the changes of avascular necrosis of the femoral head. [2],[3],[4] The primary advantage of using this procedure is avoiding a formal arthrotomy with prolonged rehabilitation and accompanying discomfort and complications. This case report illustrates the advantage of using this minimally invasive procedure instead of a formal arthrotomy for removing a bullet that got lodged in the medial wall of the acetabulum intra-articularly. The missile path was worrisome because it first traversed the urinary bladder through a suprapubic entrance wound and then passed through the colon till it penetrated the inner wall of the acetabulum.
| Case Report | | |
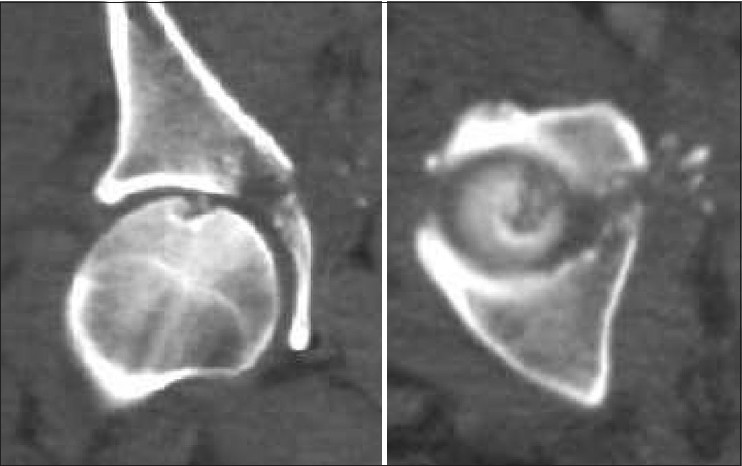
A healthy 36-year-old man sustained a close-range, low-velocity gunshot wound during an assault. The bullet length was 1.5 cm [Figure 1]. The patient was initially examined by the trauma team in the emergency room for a gunshot wound to the lower abdomen. The patient was hemodynamically unstable. The entrance wound was located in the left lower quadrant area but no identifiable exit wound was seen. Initial radiologic studies showed that the bullet was embedded in the acetabulum and possibly also intra-articularly [Figure 2]. The patient had a tense abdomen and there was a frank blood from the Foly catheter. He was immediately taken to the operating room and subsequently underwent a trauma laparotomy with small bowel repair, large bowel resection, primary anastomosis, and bladder repair with insertion of a suprapubic catheter. The major bullet fragment was not visible during pelvic exploration. Post-operatively, intravenous antibiotics were administered. The Department of Orthopedics was consulted for a retained intra-articular bullet fragment shown on a computed tomography (CT) scan [Figure 3], which was done because of ongoing low hemoglobin despite frequent blood transfusion. Physical examination revealed an intact soft tissue envelope around the hip and pelvis with an entrance wound as noted in the left suprapubic area. Neurologic status was intact. The patient did have some moderate hip pain with a range of motion but was able to perform a straight leg raise with the involved extremity, with only slight discomfort. Laboratory values including a white blood count were within normal limits, the patient was afebrile, and there were no signs of a septic joint. Patient was taken to the operating room for pelvic exploration versus hip arthroscopy. The decision was made to proceed with hip arthroscopy to remove intra-articular debris, assess the chondral surface to avoid any further damage to the femoral head by the retained fragment, and prevent the late sequelae of lead intoxication. Pelvic CT scan showed a major bullet fragment in the superomedial portion of the acetabulum, projecting into the joint. The femoral head was damaged significantly. | Figure 2: Anteroposterior view of the pelvis showing the bullet in the right acetabulum
Click here to view |
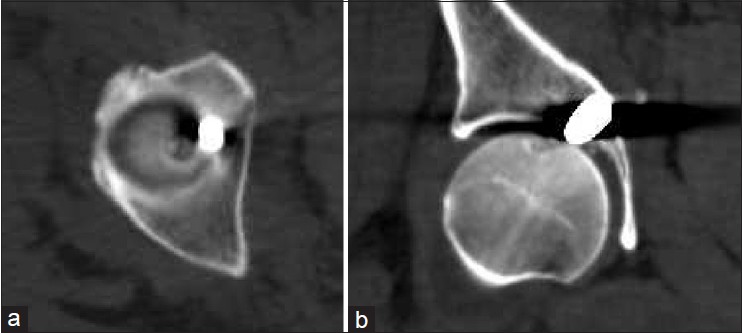 | Figure 3: (a) Axial computed tomography scan showing the bullet embedded in the medial acetabular wall intra-articularly, (b) Coronal computed tomography scan showing the bullet embedded in the medial acetabular wall intra-articularly
Click here to view |
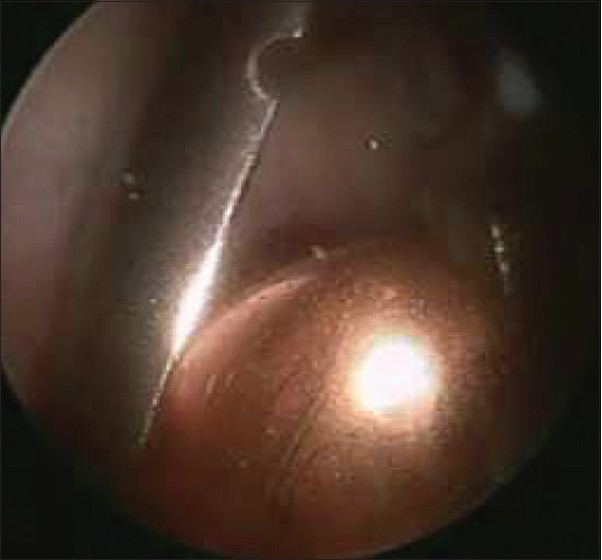
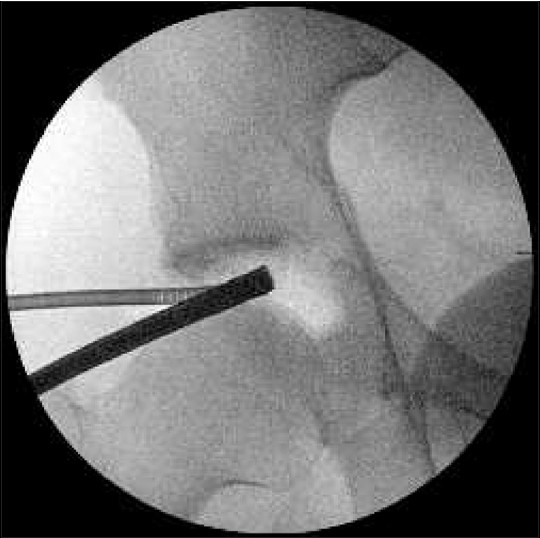
Hip arthroscopy was performed using the supine position with the involved extremity in traction on a fracture table. A spinal needle was used for localization, following which an anterolateral portal was established first using the Seldinger technique with fluoroscopic guidance [Figure 4]. A hemarthrosis was evacuated and an anterior portal was established using the same technique. A large capsulotomy was performed with the shaverand ablation devices to facilitate bullet removal. The bullet was found embedded in the medial acetabular wall [Figure 5]. It was dislodged and then removed from the inferior acetabulum with an angled pituitary grasper [Figure 6]. The surface of the femoral head was damaged by the projectile [Figure 7]. Intraoperative fluoroscopy verified removal of the entire fragment [Figure 8]. Post-operative plain-film radiographs showed very small bony fragments beside the entry point [Figure 9]. The joint was irrigated utilizing 6 liters of normal saline. We used low-pressure flow (20 mm Hg) and a series of suctioning to minimize the risk of abdominal compartment syndrome and its consequences. [5] The portals were closed in the routine fashion. The patient's abdomen remained soft following the procedure. No complications were encountered. A first-generation cephalosporin was administered post-operatively, and physical therapy was commenced on the next few days, with weight bearing for tolerance and gait training with crutches. Post-operative computed tomography scan showed very small bony fragments beside the entry point [Figure 10].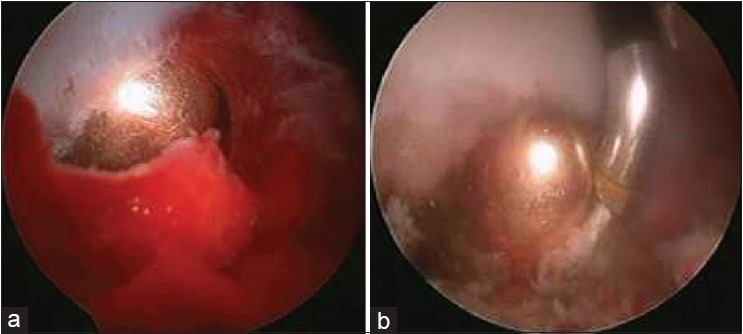 | Figure 5: (a) Arthroscopic view showing the bullet embedded in the medial acetabular wall, (b) Arthroscopic view showing the bullet embedded in the medial acetabular wall
Click here to view |
 | Figure 8: Intraoperative fluoroscopy verified removal of almost the entire fragment
Click here to view |
 | Figure 9: Post-operative plain-film radiographs showed very small bony fragments beside the entry point
Click here to view |
 | Figure 10: Post-operative computed tomography scan showed very small bony fragments beside the entry point
Click here to view |
| Discussion | | |
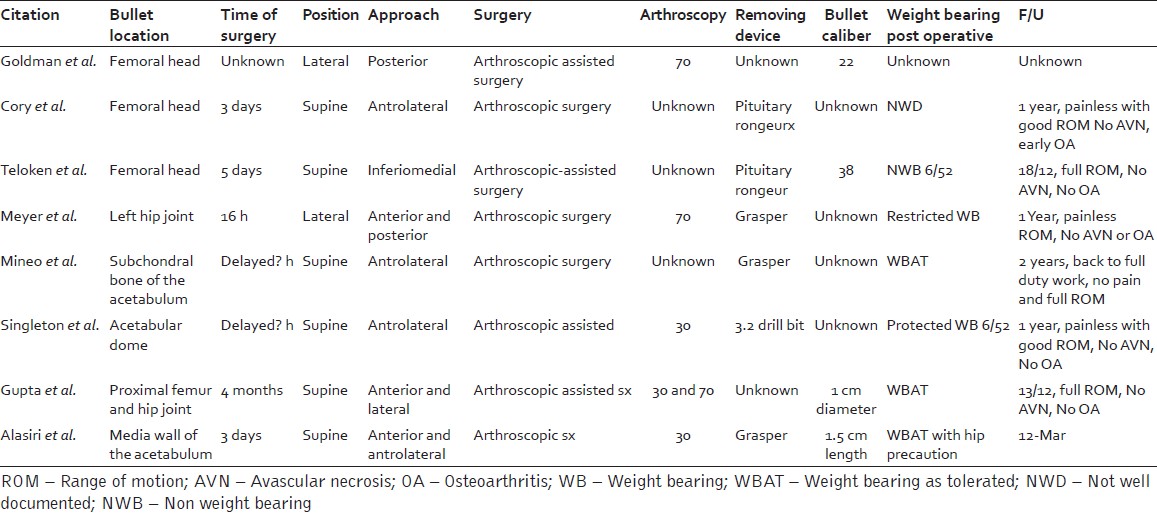
Seven previous reports of arthroscopic-assisted retrieval of bullets [Table 1] within a few days of injury from the hip joints have been reported in the English language literature. [6],[7],[8],[9],[10],[11],[12] Out of these, only four - including our case - have been retrieved purely by arthroscopy. [6],[9],[12]
Hip arthroscopy has been used successfully by many authors for treating various pathologic conditions of the hip. Removal of foreign bodies from major joints using arthroscopy has been described in sporadic case reports. [6],[7],[13],[14] Intra-articular bullets have also been retrieved with good results from major joints, to avoid the possible sequelae of lead intoxication. [6],[7],[15],[16],[17] Similarly, we report our case using arthroscopy to retrieve an intra-articular bullet. The interesting feature of this particular case was the unusual path the bullet traversed through the urinary bladder and inner wall of the acetabulum before becoming embedded intra-articularly within the acetabulum. In this case, we believed that the bullet should be removed and the joint irrigated for two reasons. First, the missile had traversed the rectum before lodging in the acetabulum and appeared to communicate with the hip joint through a fracture line, which substantially increased the risk of septic contamination of the hip joint. One might argue that the joint could be aspirated, cultures checked, and appropriate antibiotics administered. However, an analogy may be drawn to reports detailing osteomyelitis of the spine after bullets that had traversed the viscera were retained. Most spine surgeons recommend operative irrigation and debridement with subsequent bullet removal in these cases. The second rationale for surgical intervention is the well-described long-term complications of lead toxicity. [16],[17],[18],[19],[20]
Synovial fluid acts as a solvent to lead, allowing it to diffuse throughout the joint as well as enter the systemic circulation. Cory and Ruch [6] reported on the arthroscopic removal of a bullet imbedded in a femoral head by using a pituitary rongeur to grasp the missile after manipulating the femur into the appropriate position. Goldman et al. [7] published a report on bullet extraction from the hip joint using a limited posterior approach followed by the insertion of an arthroscope through the posterior capsule under direct vision.
With successful arthroscopic retrieval, we could avoid several disadvantages of an open procedure including significantly diminished blood loss, cosmetic incisions, decreased risk of osteonecrosis of the femoral head, and shortened recovery time. [6],[7] All the potential complications of hip arthroscopy were discussed with the patient before undertaking the procedure. There is a report of cardiac arrest resulting from extravasation of the irrigation fluid through the fracture line into the abdomen during the arthroscopic removal of a loose body from the hip joint of a patient with an acetabular fracture. [5] A theoretic risk of developing the same complication by introduction of the fluid through the bullet tract has also been expressed. [8]
Arthroscopy provided excellent visualization of the articular surface, allowed removal of the foreign object, and permitted a minimally invasive alternative to irrigate and debride the joint. The advantages include minimal soft tissue disruption, less post-operative discomfort, and immediate mobilization.
| Conclusion | | |
Hip arthroscopy is a minimally invasive procedure that proved, in this particular case, to be an excellent alternative to open arthrotomy. Potential complications do exist, but are reported infrequently in the literature and were not encountered in this case.
| References | | |
| 1. | Burman MS. Arthroscopy or the direct visualization of joints. J Bone Joint Surg 1931;4:669-95. 
|
| 2. | Hunter DM, Ruch DS. Hip arthroscopy. J South Orthop Assoc 1996;5:243-50.
|
| 3. | Byrd JW, Jones KS. Prospective analysis of hip arthroscopy with 2-year follow-up. Arthroscopy 2000;16:578-87.
|
| 4. | Hawkins RB. Arthroscopy of the hip. Clin Orthop Relat Res 1989;249:44-7.
|
| 5. | Bartlett CS, DiFelice GS, Buly RL, Quinn TJ, Green DS, Helfet DL. Cardiac arrest as a result of intraabdominal extravasation of fluid during arthroscopic removal of a loose body from the hip joint of a patient with an acetabular fracture. J Orthop Trauma 1998;12:294-9.
|
| 6. | Cory JW, Ruch DS. Arthroscopic removal of a.44 caliber bullet from the hip. Arthroscopy 1998;14:624-6.
|
| 7. | Goldman A, Minkoff J, Price A, Krinick R. A posterior arthroscopic approach to bullet extraction from the hip. J Trauma 1987;27:1294-300.
|
| 8. | Singleton SB, Joshi A, Schwartz MA, Collinge CA. Arthroscopic bullet removal from the acetabulum. Arthroscopy 2005;21:360-4.
|
| 9. | Meyer NJ, Thiel B, Ninomiya JT. Retrieval of an intact, intraarticular bullet by hip arthroscopy using the lateral approach. J Orthop Trauma 2002;16:51-3.
|
| 10. | Lee GH, Virkus WW, Kapotas JS. Arthroscopically assisted minimally invasive intraarticular bullet extraction: Technique, indications, and results. J Trauma 2008;64:512-6.
|
| 11. | Teloken MA, Schmietd I, Tomlinson DP. Hip arthroscopy: A unique inferomedial approach to bullet removal. Arthroscopy 2002;18:E21.
|
| 12. | Mineo RC, Gittins ME. Arthroscopic removal of a bullet embedded in the acetabulum. Arthroscopy 2003;19:E121-24.
|
| 13. | Vakili F, Salvati EA, Warren RF. Entrapped foreign body within the acetabular cup in total hip replacement. Clin Orthop Relat Res 1980;150:159-62.
|
| 14. | Williams MS, Hutcheson RL, Miller AR. A new technique for removal of intraarticular bullet fragments from the femoral head. Bull Hosp Jt Dis 1997;56:107-10.
|
| 15. | White RR. Arthroscopic bullet retrieval. J Trauma 1987;27:455-6.
|
| 16. | Windler EC, SMith RB, Bryan WJ, Woods GW. Lead intoxication and traumatic arthritis of the hip secondary to retained bullet fragments. A case report. J Bone Joint Surg Am 1978;60:254-5.
|
| 17. | Switz DM, Elmorshidy ME, Deyerle WM. Bullets, joints, And lead intoxication. A remarkable and instructive case. Arch Intern Med 1976;136:939-41.
|
| 18. | DeMartini J, Wilson A, Powell JS, Powell CS. Lead arthropathy and systemic lead poisoning from an intraarticular bullet. AJR Am J Roentgenol 2001;176:1144.
|
| 19. | Leonard MH. The solution of lead by synovial fluid. Clin Orthop Relat Res 1969;64:255-61.
|
| 20. | Otero F, Cuartas E. Arthroscopic removal of bullet fragments from the subacromial space of the shoulder. Arthroscopy 2004;20:754-6.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4], [Figure 5], [Figure 6], [Figure 7], [Figure 8], [Figure 9], [Figure 10]
[Table 1]
| This article has been cited by | | 1 |
Artroscopia de cadera en patología traumática |
|
| Víctor M. Ilizaliturri,Carlos Suárez-Ahedo | | Revista Española de Artroscopia y Cirugía Articular. 2016; | | [Pubmed] | [DOI] | | | 2 |
Arthroscopic Bullet Removal From the Central and Peripheral Compartments of the Hip Joint |
|
| Elizabeth A. Howse,Jason P. Rogers,Austin V. Stone,Sandeep Mannava,Allston J. Stubbs | | Arthroscopy Techniques. 2016; | | [Pubmed] | [DOI] | | | 3 |
A Comparison of Supine and Lateral Decubitus Positions for Hip Arthroscopy: A Systematic Review of Outcomes and Complications |
|
| Darren de SA,Kellee Stephens,Daniel Parmar,Nicole Simunovic,Marc J. Philippon,Jon Karlsson,Olufemi R. Ayeni | | Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2016; | | [Pubmed] | [DOI] | | | 4 |
Hip Arthroscopy in Trauma: A Systematic Review of Indications, Efficacy, and Complications |
|
| Gavinn Niroopan,Darren de SA,Austin MacDonald,Sarah Burrow,Christopher M. Larson,Olufemi R. Ayeni | | Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2016; | | [Pubmed] | [DOI] | |
|




 |
|
|
|