|


 |
| LETTER TO EDITOR |
|
| Year : 2012 | Volume
: 4
| Issue : 2 | Page : 140-141 |
|
|
Portal Annular Pancreas: An Under-Reported Pancreatic Anomaly
Yashwant Patidar, Ankur Arora, Amar Mukund, Ankur Dev
Departments of Radiodiagnosis, Institute of Liver and Biliary Sciences, D 1 Vasant Kunj, New Delhi, India
| Date of Web Publication | 8-Apr-2013 |
Correspondence Address:
Ankur Arora
Departments of Radiodiagnosis, Institute of Liver and Biliary Sciences, D 1 Vasant Kunj, New Delhi
India
 Source of Support: None, Conflict of Interest: None  | 2 |
DOI: 10.4103/2006-8808.110272

How to cite this article:
Patidar Y, Arora A, Mukund A, Dev A. Portal Annular Pancreas: An Under-Reported Pancreatic Anomaly. J Surg Tech Case Report 2012;4:140-1 |
How to cite this URL:
Patidar Y, Arora A, Mukund A, Dev A. Portal Annular Pancreas: An Under-Reported Pancreatic Anomaly. J Surg Tech Case Report [serial online] 2012 [cited 2016 Jun 10];4:140-1. Available from: http://www.jstcr.org/text.asp?2012/4/2/140/110272 |
Sir,
Portal annular pancreas (PAP) is an uncommon and under-recognized congenital anomaly of the pancreas, which mostly remains asymptomatic but can have serious implications if a pancreatic surgery is being contemplated. In contrast to a conventional annular pancreas in which the pancreatic tissue encircles the second part of the duodenum, portal annular pancreas is characterized by encasement of the portal vein or the superior mesenteric vein (SMV) by a rind of pancreatic parenchyma. [1],[2],[3],[4],[5]
We noted, on an axial abdominal computed tomography study of a 69-year-old female with chronic liver disease, anomalous pancreatic parenchyma encircling the main portal vein [Figure 1]a. Subsequent magnetic resonance imaging (MRI); axial T2-weighted spin echo imaging confirmed these findings and in addition revealed the retroportal course of the main pancreatic duct, that is, the pancreatic duct was seen traversing posterior (white arrow) to the portal vein [Figure 1]b.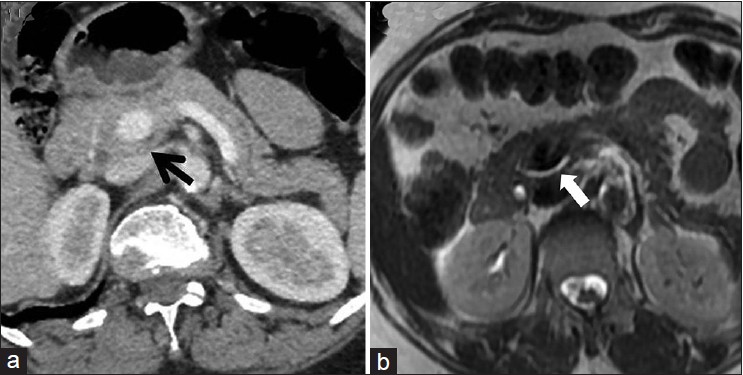 | Figure 1: (a) Axial contrast-enhanced abdominal computed tomography scan displays a rind of pancreatic tissue encircling the portal vein consistent with portal annular pancreas. (b) Axial T2-weighted magnetic resonance imaging in addition displays the retroportal main pancreatic duct traversing posterior to the portal vein
Click here to view |
The embryogenesis of pancreas is complex. It develops from a ventral and a dorsal bud of the duodenum. The ventral bud forms the major part of the head and the uncinate process, whereas the dorsal bud forms upper part of the head, the body, and tail of the pancreas. The ventral bud rotates posteriorly during the 7 th week of gestation to fuse with the dorsal bud so as to form the fully mature gland. Rarely, this fusion occurs to the left of the mesenteric or portal vein, resulting in a rind of pancreatic parenchyma encircling the portal vein. [4],[5] This has been referred to as the portal annular pancreas. Although anticipated to be extremely rare an incidence of 1.14%-2.5% has been reported by Karasaki et al. and Ishigami et al., respectively. [3],[5] The authors concluded that the prevalence of portal annular pancreas is not extremely low but is not readily recognized on preoperative imaging due to lack of adequate knowledge and awareness of this uncommon variant.
Imaging plays a pivotal role in the diagnosis of portal annular pancreas and contrast-enhanced multi-detector computed tomography (MDCT) is considered sufficient enough to establish the diagnosis. Joseph et al. have classified PAP into 3 types [Figure 2]. [4] In type I the ventral bud of the pancreas fuses with the dorsal bud posterior to the portal vein with a retroportal pancreatic duct (as is seen in the present case); type II has concomitant pancreas divisum; and type III is when the uncinate process alone is involved and the pancreatic duct is seen anterior to the portal vein (anteportal pancreatic duct). MRI, is especially useful for depicting the major as well as the accessory duct systems and thus can aid in differentiating anteportal and retroportal pancreatic duct. [2]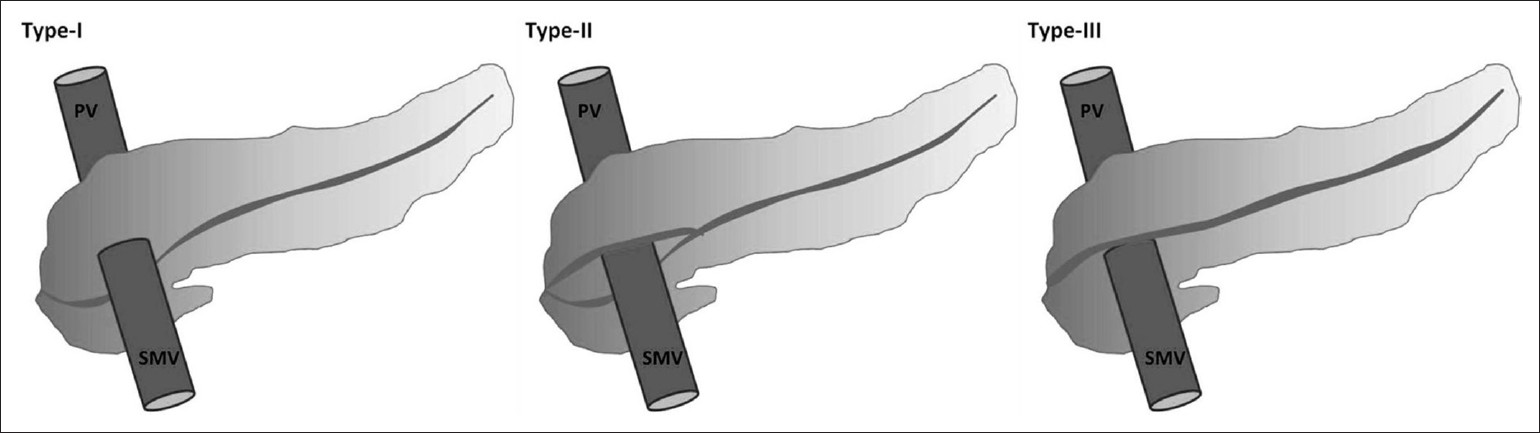 | Figure 2: Schematic representation of portal annular pancreas classification proposed by Joseph et al.
Click here to view |
The clinical importance lies in accurately identifying portal annular pancreas on preoperative imaging, especially in patients where a pancreatic surgery is being contemplated so as to avert inadvertent pancreatic injury and the attendant risk of postsurgical pancreatic fistula. [1],[2],[3],[4],[5] It is thus imperative to be aware of and carefully search for uncommon pancreatic anomalies, such as portal annular pancreas, in patients planned for pancreatic head resection, so as to avoid and minimize any surgical complications.
 References References | |  |
| 1. | Matsumoto I, Shinzeki M, Fukumoto T, Ku Y. An extremely rare portal annular pancreas for pancreaticoduodenectomy with a special note on the pancreatic duct management in the dorsal pancreas. Surgery 2011 [Epub ahead of print]. 
|
| 2. | Gonoi W, Akahane M, Akai H, Hagiwara K, Kiryu S, Hayashi N, et al. Retroportal main pancreatic duct with circumportal pancreas: Radiographic visualization. Clin Imaging 2011;35:442-6.
|
| 3. | Ishigami K, Tajima T, Nishie A, Asayama Y, Kakihara D, Nakayama T, et al. The prevalence of circumportal pancreas as shown by multidetector-row computed tomography. Insights Imaging 2011;2:409-14.
|
| 4. | Joseph P, Raju RS, Vyas FL, Eapen A, Sitaram V. Portal annular pancreas. A rare variant and a new classification. JOP 2010;11:453-5.
|
| 5. | Karasaki H, Mizukami Y, Ishizaki A, Goto J, Yoshikawa D, Kino S, et al. Portal annular pancreas, a pancreatic malformation: Frequency, morphology, and implications for pancreatic surgery. Surgery 2009;146:515-8.
|
[Figure 1], [Figure 2]
|















