|


 |
| REVIEW ARTICLE |
|
| Year : 2012 | Volume
: 4
| Issue : 2 | Page : 79-85 |
|
|
Diagnosis and Management of Adnexal Masses in Pregnancy
Ibrahim Adamu Yakasai, Lawal Abdullahi Bappa
Department of Obstetrics and Gynaecology, Royal Hampshire County Hospital, Winchester, Doncaster Royal Infirmary, Doncaster, United Kingdom
| Date of Web Publication | 8-Apr-2013 |
Correspondence Address:
Ibrahim Adamu Yakasai
Department of Obstetrics and Gynaecology, Royal Hampshire County Hospital, Winchester, Romsey Road SO22 5DG
United Kingdom
 Source of Support: None, Conflict of Interest: None  | 2 |
DOI: 10.4103/2006-8808.110249

 Abstract Abstract | | |
Widespread use of ultrasound in early pregnancy has led to the detection of incidental adnexal masses more frequently. This article reviews the diagnosis and management options for adnexal masses in pregnancy. The availability of high-resolution ultrasound has made observation to be a viable option in some cases. However, for those masses suspicious of malignancy, at risk of torsion, rupture, or clinically symptomatic, surgical treatment is warranted. Laparoscopy has been successfully used in pregnancy and is safe in experienced and trained hands in properly equipped units. Keywords: Adnexae, masses, pregnancy, review
How to cite this article:
Yakasai IA, Bappa LA. Diagnosis and Management of Adnexal Masses in Pregnancy. J Surg Tech Case Report 2012;4:79-85 |
| Introduction | |  |
Adnexa refer to the anatomical area adjacent to the uterus, and contains the fallopian tube, ovary, and associated vessels, ligaments, and connective tissue.
The reported incidence of adnexal masses in pregnancy ranges from 1 in 81 to 1 in 8000 pregnancies. [1] These cysts may be asymptomatic and may be coincidently found or until their size increases the abdominal girth. Pain due to rupture, hemorrhage into the cyst, infection, venous congestion, or torsion may be of sudden onset or of a more chronic nature. Most of these adnexal masses are diagnosed incidentally at the time of dating or first trimester screening ultrasound (USS). [2] The overall incidence of malignancy noted in adnexal masses is 1-8%. An adnexal mass in pregnancy can be complicated by torsion, rupture, or bleeding/infection, or labor obstruction. [3]
USS is of paramount importance in evaluating a pelvic mass. It is particularly important when the mass is not well defined or when pelvic examination is limited by discomfort. Both transabdominal scan and transvaginal scan (TVS) should be used together as complimentary techniques, though more detailed morphological assessment of the mass is better with TVS, especially in early pregnancy. In addition, color Doppler imaging has been shown to significantly improve the ability to distinguish benign from malignant masses. Prior to the widespread use of USS, adnexal masses in pregnancy were documented with less frequency on physical examination, especially if they were small and asymptomatic.
Management can be conservative or surgical depending on the size, gestational age, available resources, and possibly patient preference following careful evaluation.
This article will review the diagnosis of adnexal masses in pregnancy, evaluate the appropriate investigations to determine whether intervention is necessary, and recommend the most appropriate management.
| Methodology | | |
We based our review on Medline and PubMed search and our experience. We searched Medline and PubMed using the terms ovarian masses, adnexal masses, tumor markers, ultrasound, pregnancy, laparoscopy, and laparotomy for including articles by all authors. The bibliography of each article was reviewed in an effort to determine any further articles that could be included in this review. Original research articles were included if they dealt with diagnosis, evaluation, or treatment of adnexal masses in pregnancy.
| Classification | | |
Using USS, adnexal masses are classified into the following categories: Simple, solid, or complex.
[Table 1] shows a simple classification of adnexal masses in pregnancy. Functional cyst is the most common adnexal mass in pregnancy, similar to the nonpregnant state. A corpus luteum persisting into the second trimester accounts for 13-17% of all cystic adnexal masses. [3] However, the differential diagnosis throughout pregnancy also includes the following: benign masses such as dermoid cyst (7-37% incidence), serous cystadenoma (5-28% incidence), mucinous cystadenoma, ovarian malignancy accounting for approximately 1-8% of adnexal masses in pregnancy, endometrioma, hydrosalpinx, heterotopic pregnancy, and leiomyoma with an incidence of 1-2.5%. [4]
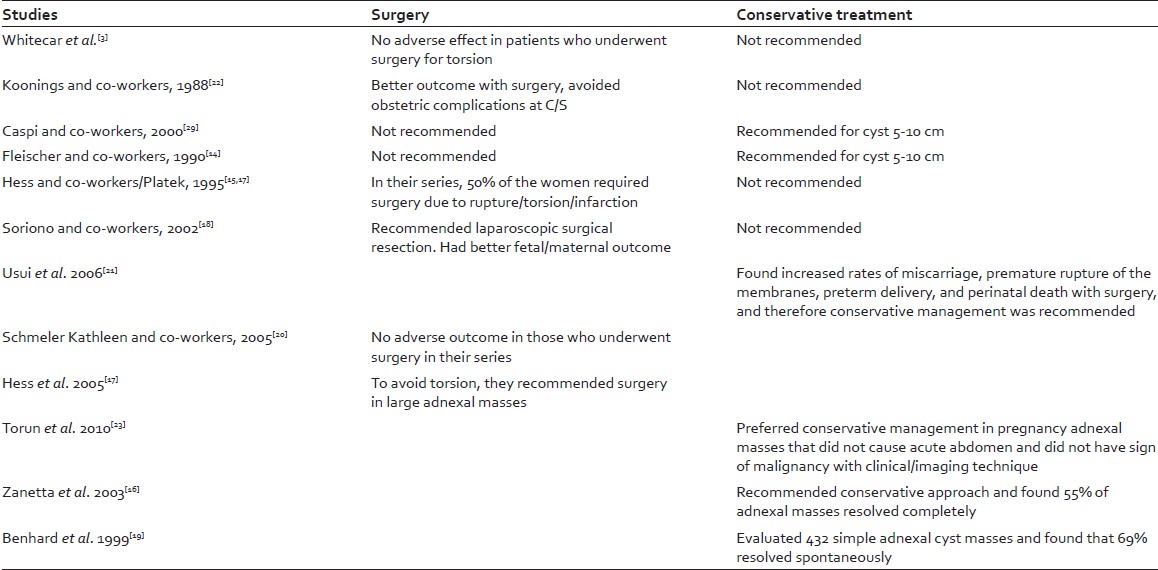
[Table 2] shows the studies comparing surgical versus conservative approaches in the management of adnexal masses .
| Assessment | | |
USS screening during the first trimester has led to the discovery of many adnexal masses in pregnancy. If an adnexal mass is palpated during examination, USS is the preferred radiological method of confirmation because of its ability to differentiate morphology and categorize the mass. This will ultimately allow stratification of risk without compromising maternal or fetal safety. [5] The aim of an USS evaluation is to aid the physician in determining those masses in which conservative management with observation is possible versus those requiring surgical intervention.
USS has been found to be accurate in determining the malignant potential of an adnexal mass; the more complex a tumor (i.e. the more septa and solid components it contains), the higher the risk of malignancy. [6],[7] Granberg et al. found the frequency of malignancy in the unilocular cyst to be 0.3%, while in multilocular cyst it was 73%. [7] In a study by Whitecar et al., [3] 89 of 91 masses diagnosed as simple cyst on USS were confirmed to be benign cysts on pathology. Color flow Doppler has been shown to be a useful adjunct in assessing the possibility of malignancy in ovarian tumor. The Doppler criteria show that malignant tumors will generally have lower blood flow impedance and higher blood flow velocity; [4] these findings can also be seen in inflammatory lesions. A similar study by Bromley and Benacerraf [4] found that USS alone was accurate in the diagnosis of dermoid tumors 97% of the time, endometrioma 80% of the time, and the diagnosis of simple cysts 71% of the time.
Endometriomas have features in common with neoplasia, such as clonal proliferation, which is consistent with the endometriosis disease theory, and are associated with subtypes of ovarian malignancy, such as endometroid and clear cell carcinoma. [8] Each of these studies uses their own form of risk assessment based on complexity of features seen on USS. All demonstrated that USS characterization of an ovarian mass complexity and size can assist with the prediction of malignancy. Characteristic features suggestive of malignancy were masses with septations, solid component nodules, papillary components, or an average diameter of greater than 5 cm. [9]
Recent studies have evaluated the utility of adding Doppler flow evaluation to gray scale USS in an effort to improve the sensitivity of antenatal diagnosis of malignancy. Wheeler and Fleischer [10] studied 34 pregnant patients with complex adnexal masses in the second trimester and found considerable overlap of Doppler blood flow pattern between benign and malignant processes with a positive predictive value of 42% and a false-positive rate of 48%. In a review article by De Priest and DeSimone, [2] they concluded that Doppler did not further aid in diagnosis compared with gray scale sonography alone, with a similar false-positive rate of 49% for the prediction of malignancy. However, three-dimensional Doppler studies may aid gray scale examination in the stratification of adnexal masses.
Computerized tomography (CT) and magnetic resonance imaging (MRI) can be useful adjuncts when USS imaging is inconclusive. CT imaging provides better resolution for identifying non-obstetric causes of abdominal pain. Although CT imaging is relatively safe in pregnancy, it does expose the mother and fetus to 2-4 rads in a single examination. [10] Contrast material can pass the placental barrier and should be used with caution because its effect is not clearly known. [10]
MRI is generally considered safe in pregnancy and is the procedure of choice in certain conditions. It is better at distinguishing paraovarian cystic lesions, which can then be managed conservatively, and also can provide better tissue characterization, allowing for more accurate evaluation of the large masses that are difficult to completely visualize by USS. MRI can also determine the possible extent of malignancy and aid in the diagnosis of acute bowel processes such as appendicitis and inflammatory bowel disease. [11] However, use of MRI in pregnancy should be judicious and solely for the clarification of an inconclusive USS result.
Certain adnexal masses may have additional features when making diagnosis by USS. Leiomyosarcomas are the malignant counterpart of benign fibroids and USS cannot reliably be used to determine sarcomatous change, although a change within the vascular pattern may be detected using Doppler.
Similarly, torsion in an ovarian cyst has no specific USS features and the diagnosis relies on comparison with the opposite ovary. The ovary may appear congested and edematous, and multiple small cysts may be seen at the periphery of the markedly enlarged ovary. However, Doppler may show the absence of blood flow in case of torsion, though this is not universal as torsion may be complete or intermittent.
The level of CA125, a glycoprotein in serum, may also be elevated with other benign disease processes such as menses, uterine fibroid, and endometriomas. CA125 is typically elevated during the first trimester, but may be useful during later assessment or follow-up. [8],[12] Other tumor markers helpful in stratifying germ cell malignancy, such as alpha-feto prtien (AFP), Beta humanchorionic gonadotrophin (BHCG), and lactate dehydrogenase (LDH), are of limited value because they may be significantly altered by pregnancy alone. [8] In general, tumor markers should be used with caution during pregnancy, particularly in the first trimester, because of the wide variation in results and interpretation. [13]
A pyosalpinx is an unlikely presentation in pregnancy where there is problem with differentiating this mass - a pyosalpinx on USS has a very typical appearance of a thick wall cystic "sausage"-shaped structure with the an incomplete septum. We should not forget the clinical features of different presentation of the adnexal masses in pregnancy where they can present with features of torsion, rupture, or bleeding into the cyst [Table 3]. [11]
| Management | | |
The major questions to be answered once an adnexal mass is discovered during pregnancy are: What is the nature of the mass? What is the likelihood that it is malignant? Secondly, is there a possibility that the mass may regress? And finally, will the mass undergo torsion, possible rupture, or will it cause obstruction during delivery?
Early in pregnancy, ovarian enlargement less than 6 cm diameter is usually due to corpus luteum formation. Resection of all suspected cysts at risk of rupture or undergoing torsion is recommended. Cysts measuring 10 cm in diameter should be resected due to increased risk of cancer in the large cysts, while cysts less than 5 cm could be left alone, and indeed, most undergo spontaneous resolution. Management of cysts between 5 and 10 cm in diameter remains controversial. Some clinicians recommend that these cysts be managed expectantly if they have cystic appearance. Others believe that if they contain septae, nodules, papillary excrescences, or solid component, resection is recommended [Table 2]. [14],[15],[16],[17],[18],[19],[20],[21],[22],[23]
In certain cases, intervention can be delayed until the second trimester, usually 14-16 weeks, when access to the mass is much easier. Where oophorectomy is done for an adnexal mass prior to this time, progesterone supplement should be administered.
Generally, there is disagreement among authors concerning the best management of adnexal masses in pregnancy, with some recommending observation and others favoring surgical management. [24] Most ovarian masses identified in pregnancy will spontaneously resolve and aggressive surgical management is not required. Characteristic features favorable for resolution are: masses that are simple in nature by USS, less than 5 cm in diameter, and diagnosed before 16 weeks. [25],[26] Larger masses or those with more complex morphology are less likely to spontaneously resolve and may represent a neoplastic process. Similarly persistent adnexal masses into pregnancy are more likely to be malignant or may result in complications in pregnancy, like torsion, rupture, or obstruction of labor. [11]
Surgical management is encouraged when there is concern that the persistent or larger ovarian mass will place the patient at higher risk for an acute abdomen, ovarian torsion, or rupture. [27] Up to 10% of persistent complex ovarian masses will ultimately be diagnosed as malignancy, implying that observation may not be appropriate. Where cancer of the ovary is found, treatment should be individualized and consideration should be given to the type and stage of the cancer, women desire to continue with the pregnancy, and the risk of modifying or delaying treatment.
Conservative management
Several small retrospective, observational studies support observational management of adnexal masses in pregnancy. [28],[29] These studies demonstrate good maternal and fetal outcomes comparable to those seen in older studies. [13],[30] Conservative management is also supported by the fact that up to 71% of benign ovarian masses will either decrease in size or resolve spontaneously.
The Royal College of Obstetricians and Gynaecologists (RCOG) in one of its guidelines stated, "Simple, unilateral, unilocular, ovarian cysts less than 5 cm in diameter have a low risk of malignancy. It is recommended that in the presence of a normal serum CA125, they can be managed conservatively." [31]
The American Society of Radiologists issued guidance for management of incidental adnexal masses noted on imaging nonpregnant, asymptomatic women. The intent was to determine which masses do not require follow-up imaging, which ones require follow-up imaging, and which ones require surgical intervention. Using sonographic assessment, stratification for further evaluation was done. Simple cysts (anechoic, smooth, thin wall, no septations) of 5-7 cm size in a premenopausal woman should be reimaged yearly. [5]
Hemorrhagic cyst of size greater than 5 cm in premenopausal women should be reimaged in 6-12 weeks. A hemorrhagic cyst of any size in early menopause (within 1-5 years since last menses) should be reimaged in 6-12 weeks; however, a hemorrhagic cyst of any size in late menopause (>5 years since last menses) warrants surgical evaluation. [5]
Endometriomas or dermoid cysts should be followed up yearly, if not surgically removed at any age. Hydrosalpinx and peritoneal inclusion cyst should be retained if clinically significant. Cysts with thin-walled septations should be reimaged in 6-12 weeks or, if stable, can be followed up yearly premenopausal. However, surgical evaluation should be considered in menopause. Cysts containing nodules with blood flow or thick septations (>3 mm) should warrant surgical management at any age. These recommendations are intended for the non-pregnant women with an incidental finding on USS and are reserved for those cysts that are truly worrisome for malignancy.
Several studies are available supporting that similar management would be reasonable for masses found in pregnant patients. [28],[30] Schmeler et al. [30] reviewed 59 pregnant patients from 1999 to 2003, who underwent either surgical or observational management for an adnexal mass of 5 cm or greater. In the study, 17 patients underwent antepartum surgery (15 laparotomies, 2 laparoscopies) and 42 patients were observed during pregnancy with their surgery performed intrapartum at the time of cesarean section or postpartum. All five malignancies (four malignant, one borderline) were in the antepartum surgery group (5/17 or 29%). All patients with an ovarian malignancy were diagnosed with stage 1 disease. No malignancies were diagnosed on final pathology in the observational group. Of note, one of the surgical management patients experienced preterm premature rupture of membranes at 23 weeks and delivered prematurely at 28 weeks. No other adverse fetal outcomes were noted in either group of patients. [30]
In an earlier observational trial by Zanetta et al., [13] complete or near-complete resolution was observed in 69% of simple cysts, 77% of endometrioid-appearing cysts, and 57% of simple cyst with minimal complex components. No resolution occurred in masses with features of mature teratoma or in borderline-appearing mass. In the 31 masses that persisted after pregnancy, 3 were borderline tumors and no other malignancies were noted to have been present. These observations certainly make conservative management a viable option for those masses of low complexity noted on USS. [13],[32]
Pregnant women may have a very low rate of ovarian cancer. Ovarian malignancies are rare during pregnancy, and when they do occur are likely to be of early stage and have favorable outcome. [2] A small retrospective study by Kumari et al. [8] did, however, report a malignancy rate as high as 10%. Malignancies in all of these observational studies suggest that with the use of TVS for risk stratification and due to the low likelihood of malignancy in the pregnant population, one may choose to advocate postponing surgery of even complex masses found in the asymptomatic pregnant patient until postpartum.
| Surgical Approach | | |
Surgery is indicated when physical examination or imaging of a pregnant woman reveals an adnexal mass that is suspicious of malignancy, but the physician must weigh the benefit of prompt surgery against the risk to the pregnancy. Traditionally, surgery for adnexal masses in pregnancy has been performed by laparotomy to provide the best exposure to the pelvis as well as upper abdomen, should surgical staging be indicated. Disadvantages to laparotomy include increased postoperative recovery time, and increased incisional pain and discomfort that may limit a patient's mobility, thereby potentiating the risk of postoperative thromboembolism in a patient population that is already at high risk.
These factors raise the question as to the feasibility and safety of laparoscopy in pregnancy. In a retrospective comparative review of 88 pregnant women undergoing surgical intervention for adnexal pathology, 39 patients underwent laparoscopy in the first trimester compared to 54 patients undergoing laparotomy (25 in the first trimester and 29 in the second trimester). No operative or postoperative maternal complications occurred in either group, with five women having first trimester miscarriages and two newborns having congenital malformations in the laparoscopy group compared to two first trimester miscarriages and one congenital malformation in the laparotomy group, illustrating that laparoscopy is safe and should be considered if technically feasible.
The advantages of laparoscopy are evident in a randomized comparison of laparoscopy versus laparotomy for benign adnexal masses, in which laparoscopy was associated with significantly lesser operative time, lesser perioperative morbidity, reduced length of hospital stay, and decreased postoperative pain resulting in faster postoperative ambulation and return to regular activity, which is very important in pregnancy because of the increased thrombotic events. [11],[26],[32] Laparoscopy is now widely used in most gynecological malignancies including staging of ovarian cancer.
Currently, there are no prospective studies comparing laparotomy and laparoscopy to determine which approach is superior. Studies comparing techniques are unlikely because of the limited number of pregnant patients requiring surgery for such a mass. However, multiple observational studies have demonstrated that laparoscopic management of adnexal masses in pregnancy is technically feasible and should no longer be considered contraindicated in pregnancy. [32]
Yuen et al. [11] reported a series of 67 women undergoing laparoscopic surgery for an adnexal mass in pregnancy. In this series, 2 of 67 (3%) laparoscopies were converted to an open procedure secondary to dense adhesive disease. One patient miscarried 6 weeks after her laparoscopy with no identifiable cause. Given the delayed timing of the miscarriage, it is unlikely that it was secondary to her laparoscopic procedure. Mo maternal or fetal complications were observed.
Lenglet et al. [33] reported that 26 of 26 patients had no complications related to surgery. Ko et al. [27] reported 11 patients with no complications from laparoscopy and have shown favorable outcomes for laparoscopy, even in the first trimester.
Soriano et al. [24] performed a retrospective review comparing 454 patients undergoing laparotomy with 34 patients having laparoscopy. The miscarriage rate was similar between the two groups, but was higher when surgery was performed by either route in the first trimester. However, Reedy et al. published an observational study of patients in Swedish Health Registry, comparing the outcomes of laparotomy and laparoscopy for the management of adnexal masses in pregnancy. During the 20-year span from 1973 to 1993, a total of 2181 laparoscopies and 1522 laparotomies were evaluated. This study did not identify any difference in birth weight, gestational age, intrauterine growth restriction, infant survival, or fetal malformation. [34]
These reports and observations demonstrate that the benefits of laparoscopic surgery with respect to lesser pain, reduced length of hospital stay, earlier ambulation, decreased blood loss, and the lower rate of infection may outweigh those of open traditional laparotomy.
In spite of the availability of these facts, there is still controversy over the effect of pneumoperitoneum on the fetus. The literature includes reports of more than 500 laparoscopic procedures on pregnant women; only one publication includes reports of adverse fetal events over the rate anticipated with laparotomy. [3] Amos et al. [32] observed four fetal deaths in seven women undergoing laparoscopic surgery, as compared to no fetal death in concurrent laparotomy group. The authors postulated that fetal demise might have been related to acidosis despite the fact that maternal CO2 levels were maintained within the standard physiological range. [33]
Laparoscopy for an adnexal mass during pregnancy should be undertaken by those well-trained in the art. Certain guidelines and recommendations must be adhered to, such as non-urgent cases should optimally be scheduled at 16-20 weeks, open Hassan technique is the preferred route of initial entry, and trocars should be placed at least 6 cm above the fundus or left upper quadrant. [35]
A guideline from the Society of American Gastrointestinal and Endoscopic Surgeons, published in 2011, makes the following recommendation: "Laparoscopy is safe and effective treatment in gravid patients with symptomatic ovarian cystic masses. Observation is acceptable for all other cystic lesions provided USS is not concerning for malignancy and tumor markers are normal. Initial observation is warranted for more cystic lesions less than 6 cm in size." [36]
When considering surgery for an adnexal mass in pregnancy, the surgeon must optimize both maternal outcome and fetal well-being while performing an expeditious removal of the mass. Pregnant women undergoing surgery are at overall risk of prematurity (up to 22%) compared with pregnant women not undergoing surgery, regardless of the route of the procedure. [37] The main disadvantage of delaying surgery during pregnancy is the risk of the mass undergoing torsion, rupture, or infarction, acute abdomen, and most importantly the risk of malignant change in case of ovarian mass. If the mass turns out to be ovarian cancer, the treatment of the pregnant woman is similar to that of the non-pregnant women depending on the stage, gestational age, as well as staging and grade of the tumor. [21] In certain circumstances, it may be justified to remove the tumor only and await fetal maturation, while in some cases chemotherapy may even be given while awaiting pulmonary maturation. [33],[38]
| Conclusion | | |
Widespread use of antenatal USS has made the diagnosis of adnexal masses in pregnancy more common. It seems reasonable to remove all ovarian masses over 10 cm in diameter because of the substantial risk of malignancy. Tumors 6-10 cm in diameter should be carefully evaluated for the possibility of neoplastic disease by the use of USS or MRI or both. Majority of the adnexal masses diagnosed in pregnancy are benign and will resolve spontaneously. Consequently, in the absence of symptoms or sonographic findings concerning malignancy, patients should be managed expectantly. If the evaluation suggests neoplasm, then surgery is indicated, either by laparotomy or laparoscopy. Laparoscopy is safe and feasible, and both maternal and perinatal outcomes are favorable. If corpus luteum is removed before 8 weeks, then progesterone supplement should be given.
| References | | |
| 1. | Kumari I, Kaur S, Mohan H, Huria A. Adnexal masses in pregnancy: A 5 year review. Aust N Z Obstet Gynecol 2006;46:52-4. 
|
| 2. | DePriest PD, deSimone CP. Ultrasound screening in the detection of ovarian cancer. J Clin Oncol 2003;21(Suppl):194s-9s.
|
| 3. | Whitecar P, Turner S, Higby K. Adnexal masses in pregnancy: A review of 130 cases undergoing surgical amangement. Am J Obstet Gynecol 1999;181:19-24.
|
| 4. | Bromley B, Benacerraf B. Adnexal masses in pregnancy: Accuracy of sonographic diagnosis and outcome. J Ultrasound Med 1997;16:447-52.
|
| 5. | Lerner JP, Timor-Tritsch IE, Federman A, Abramovich G. Transvaginal ultrsonographic characterization of ovarian masses with improved, weighted scoring system. Am J Obstet Gynecol 1994;170 (1Pt1):81-5.
|
| 6. | Timmerman D, Schwarzler P, Collins WP, Claerhuut P, Coenen M, Aman F, et al. Subjective assessment of Adnexal masses using ultrasonography: An analysis of intra observer variability and experienced. Ultrasound Obstet Gynecol 1999;13:11-6.
|
| 7. | Granberg S, Wikland M, Jansson T. Macroscopic characterization of ovarian tumours and the relation to the histological diagnosis criteria to be used in ultrasound evaluation. Gynecol Oncol 1989;35:139-44.
|
| 8. | McCarthy A. Miscellaneous medical disorders Dewhurst's textbook of Obstetrics and gynaecology. 7 th ed. United States: Blackwell Publishing; 2007. p. 283-8.
|
| 9. | Jeremy K, Luise C, Bourne T. The characteristics of common ovarian cysts in premenopausal women. Ultrasound Obstet Gynecol 2001;17:140-4.
|
| 10. | Wheeler TC, Flesischer AC. Complex Adnexal mass in pregnancy predictive value of colour Doppler sonography. J Ultrsound Med 1997;16:425-8.
|
| 11. | Yuen P, Ng P, Leung P, Rogers M. Outcome of laparoscopic management of persistent Adnexal mass during the second trimester of pregnancy. Surg Endosc 2004;18:1345-7.
|
| 12. | Aslam N, Ong C, Woelfer B, Nicolaides K, Jurkovic D. Serum CA125 at 11-14 weeks of gestation in women with morphologically normal ovaries. BJOG 2000;107:689-90.
|
| 13. | Zanetta G, Rota S, Chiari S, Bonazzi C, Mangioni C, Bratina G. Behavior of borderline tumors with particular interest to persistence, recurrence and progression to invasive carcinoma: A prospective study. J Clin Oncol 2001;19:2658-64.
|
| 14. | Fleischer AL, Dimesh MS, Entman SS. Sonograhic evaluation of maternal disorders during pregnancy. Radiol Clin North Am 1990;28:51
|
| 15. | Platek DN, Henderson CE, Goldberg GL: The management of a persistent adnexal mass in pregnancy.Am J Obstet Gynecol 1995;173:1236.
|
| 16. | Zanetta G, Mariani E, Lisson A. A prospective study of the role of ultrasound in the management of Adnexal masses in pregnancy. Br J Obstet Gynaecol 2003;110:578.
|
| 17. | Hess LW, Peaceman A, O'Brien WF. Adnexal mass occurring with intrauterine pregnancy:Report of fifty-four patients requiring lalparotomy for Definitive management. Am J Obstet gynecol 1988;158:1029.
|
| 18. | Soriono D, Yefet Y, Seidman DS: Laparoscopy versus laparotomy in the management of adnexal masses during pregnanacy. Fertil Steril 1999;71:955.
|
| 19. | Benhard LM, Klebba PK, Gray DL, Mutch DG. Prediction of persistence of adnexal masses in pregnanacy. Obstet Gynecol 1999;93:585-9.
|
| 20. | Schemeler KM. adnexal masses in pregnancy: a review of 130 cases undergoing surgical management. Obstet Gynecol 2005;105:1098-103.
|
| 21. | Usui R. A retrospective survey of clinical, pathological and prognostic features of adnexal masses operated during pregnancy. J Obstet Gynecol Res. 2008;26:89-93.
|
| 22. | Koonings PP, Platt LD, Wallace R. Incidental adnexal neoplasms at cesarean section. Obstet Gynecol 1988;72:767-9.
|
| 23. | Nick AM, Schmeler K. Adnexal masses in pregnancy. Perinatology 2010;2:13-21.
|
| 24. | Soriano D, Yuval Y, Saidman D, Goldenberg M, Sholmo M, Oessner G. Laparoscopy versus laparotomy in the management of Adnexal masses in pregnancy. Fertil Steril 1999;71:955-60.
|
| 25. | Mazze RI, Kallen B. Reproductive outcome after anaesthesia and operation during pregnancy: A registry of 5,405 cases. Am J Obstet Gynecol 1989;161:178-85.
|
| 26. | Whiteside J, Keup H. laparoscopic management of the ovarian mass: Practical approach. Clin Obstet Gynecol 2009;52:327-34.
|
| 27. | Ko ML, Lai T, Chen S. Laparoscopic management of complicated Adnexal masses in the first trimester of pregnancy. Fertil Steril 2009;92:283-7.
|
| 28. | Platek DN, Henderson CE, Golderberg GL. The management of persistent Adnexal mass in pregnancy. Am J Obstet Gynecol 1995;173:1236-40.
|
| 29. | Caspi B, Levi R, Appleman Z. conservative management of ovarian cystic tereatome during pregnancy and labor. Am J Obstet Gynecol 2000;182:503.
|
| 30. | Schemeler KM, Mayo-Smith WW, Peipert JF, Wetzen S, Manuel MD, Gordinier ME. Adnexal masses in pregnancy: Surgery compared with observation. Obstet Gynecol 2005;105:1098-103.
|
| 31. | Royal College of Obstetricians and Gynaecologists (RCOG). Ovarian cyst in post-menopausal women. Greentop Guidelines(34), 2003.
|
| 32. | Amos J, Schorr S, Norman P, Poole GV, Thomae KR, Mancino AT, et al. Laparoscopic surgery during pregnanacy. Am J Surg 1996;171:435-7.
|
| 33. | Lenglet Y, Roman H, Robishong B, Bourdel N, Bonnin M, Bolandard F, et al. Laparoscopic management of ovarian cyst in pregnancy. Gynecol Obstet Fertil 2006;34:101-6.
|
| 34. | Reedy M, Kallen B, Kuehl T. Laparoscopy during pregnancy: A study of five fetal outcome parameters, with use of Swedish Health Registry. Am J Obstet Gynecol 1997;177:673-80.
|
| 35. | Guidelines Committee of the Society of American Gastrointestinal and Endoscopic Surgeons, Yumi H. Guidelines for diagnosis, traetment and use of laparoscopy for surgical problems in pregnancy. Surg Endosc 2000;10:511-5.
|
| 36. | Society of American Gastrointestinal and Endoscopic Surgeons (SAGES). Guidelines for diagnosis, treatment, and use of laparoscopy for surgical problems during pregnancy. Los Angeles (CA): Society of American Gastrointestinal and Endoscopic Surgeons (SAGES); 2011.
|
| 37. | Rizzo A. Laparoscopic surgery in pregnancy: Long-term follow up. J laparosc Adv Surg Tech A 2003;13:11-5.
|
| 38. | Schemeler K, William W, Jeffrey PF, Weitzen SW, Misty MD, Gordiner ME. Adnexal masses in pregnancy: Surgery compared with observation. Obstet Gynecol 2005;105:1098-103.
|
[Table 1], [Table 2], [Table 3]
|