|


 |
| CASE REPORT |
|
| Year : 2013 | Volume
: 5
| Issue : 1 | Page : 51-53 |
|
|
Laparoscopic colectomy for a patient with congenital renal agenesis
Hiroyuki Tanishima, Tetsuya Horiuchi, Yoshiharu Shono, Masamichi Kimura
Department of Surgery, National Hospital Organization, Osaka Minami Medical Center, Osaka, Japan
| Date of Web Publication | 21-Sep-2013 |
Correspondence Address:
Hiroyuki Tanishima
Department of Surgery, National Hospital Organization, Osaka Minami Medical Center, 2?1 Kidohigashimachi, Kawachinagano-Shi, Osaka 586-8521
Japan
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.118631

 Abstract Abstract | | |
We present a very rare case of laparoscopic colectomy for a patient with ascending colon cancer and an agenetic right kidney. A 57-year-old man visited our institute for further evaluation for a positive fecal occult blood test. Approximately, 20 years earlier, the right kidney of the patient was found to be congenitally absent. A physical examination indicated no anatomical anomalies in his genitourinary system, and the renal function was within the normal range. Total colonoscopy revealed a cancer of the ascending colon and laparoscopic colectomy was performed. The right colon was mobilized by lateral-to-medial extension of a retroperitoneal dissection between the fusion fascia and the anterior renal fascia. The right testicular vessels were preserved without injury to the anterior renal fascia; however, the right ureter could not be detected. The operation was performed safely. Thus, we believe that in patients with congenital unilateral renal agenesis, the anterior renal fascia is present, and laparoscopic ipsilateral colectomy can be safely performed in such patients. Keywords: Anterior renal fascia, laparoscopic colectomy, renal agenesis
How to cite this article:
Tanishima H, Horiuchi T, Shono Y, Kimura M. Laparoscopic colectomy for a patient with congenital renal agenesis. J Surg Tech Case Report 2013;5:51-3 |
How to cite this URL:
Tanishima H, Horiuchi T, Shono Y, Kimura M. Laparoscopic colectomy for a patient with congenital renal agenesis. J Surg Tech Case Report [serial online] 2013 [cited 2016 May 25];5:51-3. Available from: http://www.jstcr.org/text.asp?2013/5/1/51/118631 |
| Introduction | |  |
Congenital unilateral renal agenesis is a rare condition. In patients with the congenital absence of the kidney, the renal fascia is also absent. [1] Here, for the first time, we report the case of a patient with cancer of the ascending colon and right renal agenesis who was treated by laparoscopic colectomy, and discussed the presence of the anterior renal fascia in such cases based on our experience and from a review of the literature.
| Case Report | | |
A 57-year-old man presented to our institute for further evaluation following a positive result in an fecal occult blood test. Approximately 20 years earlier, he was diagnosed with congenital agenesis of the right kidney. He was otherwise entirely healthy without any other significant past or current medical problems. A physical examination showed no abnormalities of the genitourinary system. A contrast-enhanced computed tomography of the abdomen indicated the absence of the right kidney and a hypertrophic left kidney [Figure 1]a, and indicated the presence of the right testicular vessels located behind the renal fascia [Figure 1]b, but no other anomalies were observed. Total colonoscopy revealed the presence of a tumor, measuring 1.5 cm × 1.0 cm in the ascending colon; the tumor could not be elevated by injection of saline into the submucosal layer. Because endoscopic treatment was impossible, we performed laparoscopic colectomy and lymph node dissection.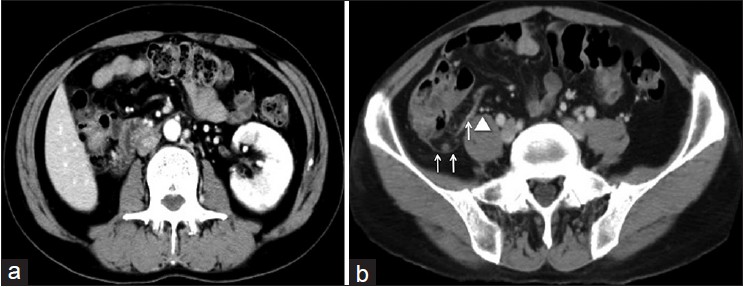 | Figure 1: (a) Abdominal computed tomography showed that the right kidney was absent and the left kidney was hypertrophic and (b) the right testicular vessels (arrow head) were present behind the renal fascia (arrow)
Click here to view |
The operative procedures and findings are as follows. The subumbilical trocar was initially placed using the open laparoscopic technique. After CO 2 pneumoperitoneum was established, three other ports were placed. No particular findings such as ascites, adhesion, peritoneal seeding, or anatomical anomalies were noted in the abdominal cavity. The right colon was mobilized to the root of mesocolon by lateral-to-medial extension of retroperitoneal dissection between the fusion fascia and the anterior renal fascia. This procedure was performed in the usual manner. The right testicular vessels were observed behind the anterior renal fascia; however, the right ureter could not be detected [Figure 2]. Furthermore, we could not detect the right renal and adrenal vessels within the operative field. The ileocolic and right colic vessels were ligated near these origins using endoscopic clips, and were mobilized divided. After the segment of the colon was completely mobilized, the ileum and colon were extracted from the abdominal cavity via a right pararectal incision and were then divided. After Gambee's hand-sewn end-to-end anastomosis was performed, the intestine was placed back into the abdominal cavity. During laparoscopy, the abdominal cavity was irrigated, a drain tube was placed at the paracolic gutter, and all other ports were removed. The incisions were closed using absorbable sutures and staples. Histological examination showed a well-differentiated adenocarcinoma that invaded to the submucosal layer without infiltration to the vessels or lymph ducts. No lymph node metastases were detected. The postoperative course was uneventful except for ileus, which was treated conservatively. The patient is currently healthy; he is receiving regular follow-up examination, and has no signs of recurrence and other malignancies.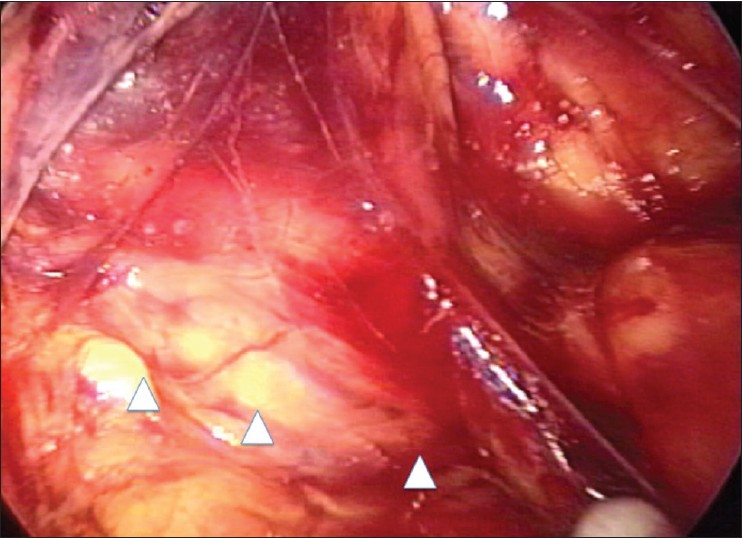 | Figure 2: The right testicular vessels (arrow head) were preserved under the anterior renal fascia, but the right ureter was not identified
Click here to view |
| Discussion | | |
Developmental anomalies of the genital and urinary tract are well-known to occur simultaneously. This is a result of the common embryologic origin of these two organ systems. Between the 4 th and 7 th weeks of embryonic life, the ureteral bud develops from the caudal end of the mesonephric duct and meets the metanephric cap and then moves cranially. The cranial end of ureteral bud develops into the pelvis and calyces. Cranial growth of the ureteral bud toward the metanephrogenic blastema stimulates renal development. The incomplete interaction of the ureteral bud and the metanephrogenic blastema results in a dysplasia or a complete absence of the kidney.
The incidence of unilateral renal agenesis based on the results of the autopsy studies ranges from 1 in 600 to 1 in 1900, and is slightly higher in men than in women. [2],[3] Moreover, the rate of incidence of simultaneous genital anomalies and unilateral renal agenesis is 22% of all patients, and is 3 times greater in women (40%) than in men (12%). [3] The most common the genital anomalies in patients with unilateral renal agenesis include cryptorchidism and seminal vesicle cyst in men and duplication of the uterus and double vagina in women. [3] To our knowledge, no studies have reported a relationship between renal agenesis and the development of carcinoma in the genitourinary tract or the gastrointestinal tract.
The renal fascia was first documented by Zuckerkandl in his article entitled "Supporting Structures of Kidney" in 1888. [4] After 12 years, Gerota described, in the article entitled "Report on the Discovery of the Attachment Apparatus of the Kidneys," the presence of anterior renal fascia and clearly assigned Zuckerkandl's name to the fascia retrorenalis. [5] Thus, Gerota's fascia refers to the anterior renal fascia, whereas Zuckerkandl's fascia refers to the posterior renal fascia. [6] The anterior and posterior layers of the renal fascia fuse and continue with the inferior fascia of diaphragm on the cranial side, with the iliac fascia on the caudal side. Moreover, these fascias merge into the lateroconal fascia on the lateral side and medially into periaortocaval connective tissue. [7] These fascia planes separate the perirenal fat from the pararenal fat in the retroperitoneal space. The gonadal vessels and ureters run through the space enveloped by these renal fascias.
The embryonal development of the renal fascia begins toward the end of the 2 nd month of embryonic life, and continues during the 3 rd month. However, the mechanism underlying this development remained unclear. The renal fascia does not develop in the situation of congenital renal agenesis. [1],[8],[9] Tobin indicated the absence of the renal fascia on the same side as renal agenesis in a newborn infant; furthermore, when the ureter was found to be partially presented, the fascia was poorly developed and ended with the cephalic tip of the ureter. [1],[9] However, in the present case, we were able to identify a thin membrane behind the dorsal side of mesocolon and mobilized the ascending colon along the easily dissectible plane between the fusion fascia and this membrane. The right testicular vessels were not directly visualized, but were observed through this membrane. We regarded this membrane as the anterior renal fascia on the basis of its anatomical location.
In conclusion, we detected the presence of the anterior renal fascia in our patients who had renal agenesis. The presence of the anterior renal fascia and the absence of the ureter facilitate the safe treatment of patients with congenital unilateral renal agenesis with laparoscopic colectomy.
| References | | |
| 1. | Benjamin JA, Tobin CE. Abnormalities of the kidneys, ureters, and perinephric fascia: Anatomic and clinical study. J Urol 1951;65:715-33. 
[PUBMED] |
| 2. | Felding C. Obstetric studies in women with histories of urinary infections. Acta Obstet Gynecol Scand 1965;44:304-16.
[PUBMED] |
| 3. | Thompson DP, Lynn HB. Genital anomalies associated with solitary kidney. Mayo Clin Proc 1966;41:538-48.
[PUBMED] |
| 4. | Zuckerkandl E. Supporting structures of the kidney. Med Jahr 1883;13:59-67.
|
| 5. | Gerota D. Report on the discovery of the attachment apparatus of the kidneys. Arch Anat Entwicklungsgeschichte Leipzig 1895:265-85.
|
| 6. | Chesbrough RM, Burkhard TK, Martinez AJ, Burks DD. Gerota versus Zuckerkandl: The renal fascia revisited. Radiology 1989;173:845-6.
[PUBMED] |
| 7. | Wolfram-Gabel R, Kahn J, Rapp E. Is the renal space closed? Clin Anat 2000;13:168-76.
[PUBMED] |
| 8. | Amin M, Blandford AT, Polk HC Jr. Renal fascia of Gerota. Urology 1976;7:1-3.
[PUBMED] |
| 9. | Tobin CE. The renal fascia and its relation to the transversalis fascia. Anat Rec 1944;89:295-311.
|
[Figure 1], [Figure 2]
|















