|


 |
| ORIGINAL ARTICLE |
|
| Year : 2013 | Volume
: 5
| Issue : 2 | Page : 65-71 |
|
|
Facial fracture management in Northwest Nigeria
Abdurrazaq Olanrewaju Taiwo1, Olujide Oladele Soyele2, Ndubuizi Ugochukwu Godwin2, Adebayo Aremu Ibikunle3
1 Department of Surgery/Dental and Maxillofacial Surgery, College of Health Sciences, Usmanu Danfodiyo University/Usmanu Danfodiyo University Teaching Hospital, Sokoto, Nigeria
2 Department of Dental and Maxillofacial Surgery, Usmanu Danfodiyo University Teaching Hospital, Sokoto, Nigeria
3 Department of Oral and Maxillofacial Surgery, Lagos University Teaching Hospital, Lagos, Nigeria
| Date of Web Publication | 13-Mar-2014 |
Correspondence Address:
Abdurrazaq Olanrewaju Taiwo
Department of Surgery, College of Health Sciences, Usmanu Danfodiyo University, PMB 12003, Sokoto
Nigeria
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.128723

 Abstract Abstract | | |
Background: Facial fracture is gradually become a public health problem in our community due to the attendant morbidity and mortality. Hence, the aim of this study was to determine the pattern of facial fracture in Dental and Maxillofacial Surgery Department of Usmanu Danfodiyo University Teaching Hospital. This cross-sectional study was undertaken to provide information regarding gender, age, etiology, and diagnosis of patients with maxillofacial fractures. Materials and Methods: A 1-year review of patients diagnosed and treated for facial fractures in Usmanu Danfodiyo University Teaching Hospital between January 2011 and December 2011. The diagnosis was based on radiographic data and clinical examination. The main analysis outcome measures were etiology, age, gender, site, and treatment. Data were organized and presented by means of descriptive statistics and Pearson's Chi-square test. The level of significance adopted was 5%. Results: A total of 40 patients were treated in this period. Over 95% were male, 81% were caused by road traffic crash (RTC) and 86.4% were in the 21-30 years group. Most patients (52%) had mandibular fractures, and the most common site was the body. Most patients with midfacial fractures had fractures of the zygomaticomaxillary region (36%), while fractures of the parasymphyseal region were more common in the mandible 156 (31%). The most common treatment for jaw fractures was mandibulomaxillary fixation (MMF). Stable zygomatic complex fractures were reduced (elevated) intraorally, and unstable ones were supported by antral packs. Conclusions: This study highlights facial fractures secondary to RTC as a serious public health problem in our environment. Preventive strategies remain the cheapest way to reduce direct and indirect costs of the sequelae of RTC. It also bring to the fore the necessity to shift to open reduction and internal fixation (ORIF) of fractures. Keywords: Facial fracture, jaw fixation techniques, mandibulomaxillary fixation, maxillofacial injuries, motorcycle, open reduction and internal fixation, road traffic crash, traffic accidents
How to cite this article:
Taiwo AO, Soyele OO, Godwin NU, Ibikunle AA. Facial fracture management in Northwest Nigeria. J Surg Tech Case Report 2013;5:65-71 |
How to cite this URL:
Taiwo AO, Soyele OO, Godwin NU, Ibikunle AA. Facial fracture management in Northwest Nigeria. J Surg Tech Case Report [serial online] 2013 [cited 2016 May 25];5:65-71. Available from: http://www.jstcr.org/text.asp?2013/5/2/65/128723 |
| Introduction | |  |
Facial fracture often involves serious morbidity in our community and sometimes fatal consequence. It is a common sequel of blunt and penetrating trauma. [1] Blunt trauma includes road traffic crash (RTC), altercation, industrial/occupational accidents, sports, and falls. [1],[2],[3],[4] Penetrating injuries are results of gunshots, missiles, stabbing, and explosions. Pathological diseases such as tumors, osteomyelitis, cysts, osteoradionecrosis may also contribute to facial fracture. [1],[2],[3],[4],[5] RTCs have been reported as the most frequent reason for facial fractures in Nigeria, rural and developing world; [1],[5],[6],[7],[8] while altercations remains the leading causes in urban and developed countries. [9],[10] However, recent report on the war in Afghanistan by Breeze and associates have identified increasing facial fractures among British troops despite to protective armor worn and advances in on-field resuscitation and critical care that have increased survival in the battle field. [11] Falls are common in the very young and elderly. [12] Pattern of facial fracture is predicated on etiology, population density, socioeconomic, cultural, race, and time. [1],[5] Others include types of facilities available, regional government and geography. [12],[13]
Facial fractures and other maxillofacial injuries have high clinical significant because the anatomical specificity of face provides protection to important vital organs such as the brain and eyes and others like the digestive and respiratory systems. [12] The facial skeleton is one of the most complex arrangements of curving bony structures in the body and consists of bones of the mandible, maxilla, zygoma, bony walls of the nasal cavities, paranasal sinuses, and orbit. [12],[13] Injuries to this region can result in serious dysfunctions of sight, smell, breathing; eating and talking which impact negatively on the victim's quality of life. Moreover, owing to high premium placed on facial appearance in many societies esthetic disturbance could results in adverse psychological consequence. [13] Unfortunately, limited specialized manpower needed to treat this injuries and the considerable treatment cost imposes huge burden and demand on the ever dwindling healthcare recourses of developing nation like ours. [5],[6],[7],[8]
Owing to the forgoing, it is necessary to explore the etiology and pattern of fractures of facial skeleton. Such periodic verification of the etiology of maxillofacial injuries will facilitates the assessment of proficiency of road safety measures such as speed limit, drunk driving, crash helmets, and seat belt laws. It will also help to identified the behavioral patterns of commuters in the locality and helps to recommend ways in which injuries to the face can be averted. [5]
It will also guide the future funding of public health programs geared towards prevention, provision of facilities, training of manpower; and aid the healthcare provider to optimize treatment of maxillofacial injuries. [3] However, such information is lacking from northwestern Nigeria especially Sokoto. Hence, this study is aimed at reporting the etiology, pattern, and treatment of facial fractures at our Oral and Maxillofacial Surgery Department in Usmanu Danfodiyo University Teaching Hospital, Sokoto.
| Materials and Methods | | |
Case records of 40 patients who presented with facial fracture at the Dental and Maxillofacial Surgery Department of Usmanu Danfodiyo University Teaching Hospital, Sokoto between January, 2011 and December, 2011 were retrieved by the first author and the following variables etiology, age, gender, site, and treatment were obtained.
This hospital is the only tertiary and referral center in the state and it is strategically located in the state capital, Sokoto.
Sokoto is a city located in the extreme northwest of Nigeria, near to the confluence of the Sokoto River and the Rima River. Sokoto is the modern day capital of Sokoto State (and its predecessor, the northwestern state). It is situated in northwestern of the country between latitudes 4°N to 14°N and longitudes 2°E and 15°E. Kebbi state border to the southwest, Katsina state to the east, Zamfara state to the southeast, and Republic of Niger to the northwest with a land mass of approximately 25,973 km 2 . [14]
Sokoto state has a projected population of 3.7 million people based on 2006 census made up of two ethnic groups namely, Hausa and Fulani. Sokoto town, the capital of Sokoto state, has a population of approximately 2.5 million. The population is largely rural with farming, cattle rearing, and fishing as the predominant occupations (>80%). [14]
The diagnosis of fracture was based on clinical history, signs and symptoms, visual findings, manual examination, and correct interpretation of plain radiographs. The pattern of facial fracture is determined according to the fractures of mandible, midface, and alveolar bone. Fractures of the middle third of the facial skeleton were classified according to the Le Fort classification. Treatment modalities given were highlighted. Fractures including the base of the skull and frontal bone were not included in the present study.
Closed reduction and dental wiring with arch bars, direct wires, and eyelet wires combine with mandibulomaxillary fixation (MMF) were routine mode of treatment for mandibular fractures. Open reduction and internal fixation (ORIF) with intraosseous wire of mandibular fractures were employed when indicated. Fractures of the maxillae/Le Fort fractures were reduced and fixed by eyelets/arch bars combined with MMF and with/without suspension wires. Stable zygomatic complex fractures were reduced (elevated) intraorally, and unstable ones were supported by antral packs.
All patients were placed on oral or intravenous antibiotics for 5-7 days except those with established infections who had their antibiotics regimen appropriately extended. Follow-up period was 6 weeks-6 months.
Data analyses for age, sex, etiology, site of fracture, and treatment given were performed using Analyse-it for Microsoft Excel 2012. Simple frequencies were computed and cross tabulations of some variables were made. Pearson's Chi-square test was used to compare the frequency distribution and statistical significance was set at P ≤ 0.05.
| Results | | |
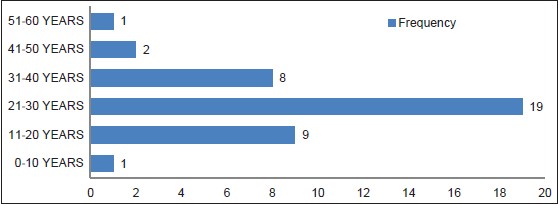
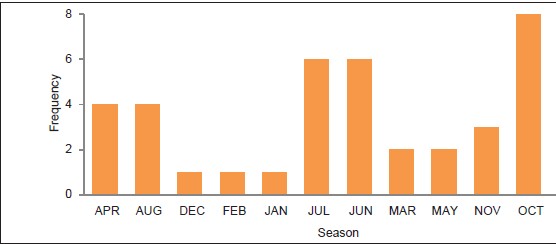
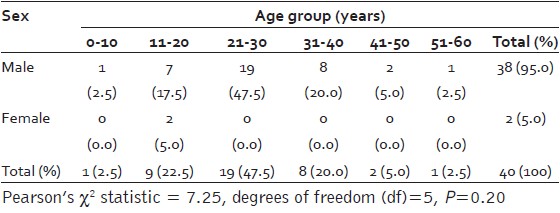
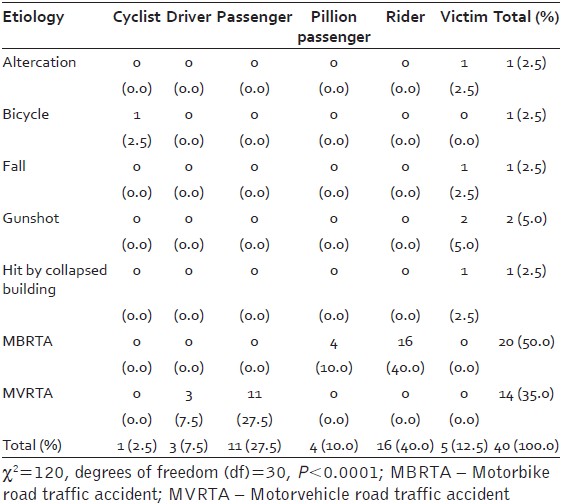
Patients' age ranged from 8 to 60 years (27.6 ± 10.4 years). There was an overwhelming male dominance in all age groups (male: female (M:F) =19:1, odds ratio = 380) [Table 1]. The most susceptible age group was 21-30 years (47.5%) and the least were 0-10 years and 51-60 years (2.5%) [Figure 1]. The most common cause of fracture was RTCs (87.5%) of which 58.3% were motorcycles related and mostly involved riders (80.9%) [Table 2]. There was 15.0% associated head injury (P = 0.68). Maxillofacial trauma was highest in the months of October (20%) and June/July (15%) [Figure 2].
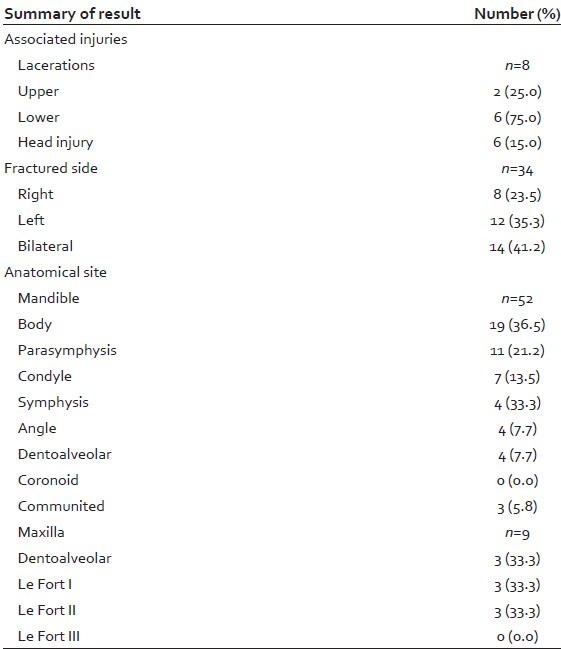
Isolated mandibular fractures were most frequent (60%) and least fractured bone was maxilla (7.5%) [Figure 3]. Among mandibular fractures, the body was more regularly involved (36.5%) followed by parasymphyseal (21.2%) [Table 3]. For midfacial fractures, zygomatic bone and arch were most frequently involved (68.4%) [Table 3]. There were associated soft tissue injuries with the lower lip mostly affected (75%) especially in RTCs (P < 0.05). In 14 (41.2) cases there were bilateral fractures.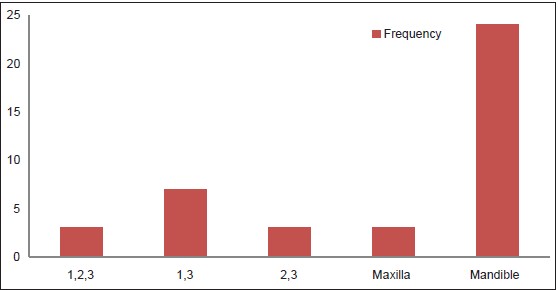 | Figure 3: Facial fracture distribution according to involved bone.1 – Mandible; 2 – Maxilla; 3 – Zygoma
Click here to view |
Closed reduction and dental wiring with arch bars, direct wires, and eyelet wires combined with MMF were the most common form of treatment for mandibular fractures [Figure 4]. Wire osteosynthesis is employed for ORIF of mandibular fractures in few cases. Fractures of the maxillae/Le Fort fractures were reduced and fixed by eyelets/arch bars combined with suspension wires and MMF. Zygomatic complex fractures were treated either conservatively or by either closed or open reduction with Gillies' temporal or buccal approaches.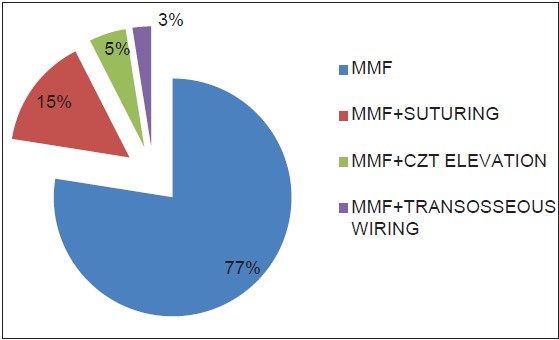 | Figure 4: Treatment of facial fracture's patients. MMF-Mandibulomaxillary fixation, CZT-zygoma
Click here to view |
| Discussion | | |
Facial fracture has become a public health issue in many parts of Nigeria and globally owing to the attendant mortality, morbidity, and huge socioeconomic consequences. [6] There is paucity of epidemiologic data from Sokoto, northwest region of Nigeria. Hence, this study was primarily undertaken to look at the pattern of facial fracture and treatment modalities at our relative young center offering maxillofacial trauma services. We hoped that this will help to provide baseline information to guide in prevention and proper planning of maxillofacial trauma care in our hospital and in the region.
In this present study, more males were affected than females with a very high odd ratio; this is the highest reported figure from Nigeria and worldwide. [1],[3],[4],[5],[6],[7],[8],[9] Kadkhodaie; Al Ahmed et al., and other studies from Middle East reported similar high ratio. [15],[16],[17],[18],[19] Our finding, is however, not in concordance with most studies from Nigeria, western Europe, and Japan that showed much narrower gender ratio. [5],[6],[7],[8],[9],[10],[11],[12],[20],[21] Fasola et al., and Tanaka et al., found a 3:1 male-to-female ratio. [7],[21] There had been several postulations in the literature regarding the high male bias. Sing et al., suggested that higher level of physical activities among males might be the reason. [13] Others include more male exposure to certain risky situations, for example, there are more male drivers on the roads, especially on highways; men are more likely to practice contact sports; and men attend bars more often and consequently are more likely to use alcohol and other drugs prior to driving. [3],[5] In addition, culturally in many traditional African and Islamic societies, male are often the bread winner of the family and women predominantly take care of the home and only occasionally involved in other activities outside. In works with narrower or equal gender ratio, the female lived a more outdoor life and share similar jobs with their male counterpart, thereby being exposed to similar risk factors. [5],[6],[7],[8],[9],[10],[11]
Maxillofacial fracture incidence in the present study was highest in October followed by June and July. Kontio et al., [9] in his study found an increase in incidents in June and August, while Ravindra and Ravindra Nair [1] reported significant high in April and May. Ogundare et al., and Paes et al., [3],[22] suggested that increased maxillofacial trauma during summer holiday is due to availability of more leisure time and high alcohol consumption. However, our own data indicates that the months of June and July are peak of raining season, while October is the harvesting time. Hence, road travel might be compromised especially with increased density of people plying these roads.
The modal age group of 21-30 years seen in this present cohort is consistent with the literature. [1],[2],[3],[4],[5],[6],[7],[8],[9],[10],[13] Paes et al., pointed out that this age group reflects people at the prime of their life. They have zest, increased physical energy, and adventurousness, but lack experience and often impetuous; hence, are likely to disregard traffic regulations. [2],[5],[6],[23] In the present study, the maximum age was 60 years. The reason in this cohort is unknown; however, we speculate that owing to preponderance of RTC and its severity, elderly patients might not have survived. We wish to examine this observation in future prospective study.
The etiology of maxillofacial injuries varies from one country to another and even within the same country depending on the prevailing socioeconomic, cultural, and environmental factors. [5],[6] Recent works had established RTC as the leading agent of facial fractures in most developing countries of Africa, Middle East, Asia, and some parts of Europe. [5],[6],[7],[8],[9],[16],[18],[19],[20],[24] In contrast to Zimbabwe, South Africa; northeastern Nigeria and economically advance nations of Europe, Australia, and United State of America; [1],[2],[17],[21],[23],[25],[26],[27] interpersonal violence in the form of physical assaults and gunshots has replaced RTC as the predominant cause of facial fracture. According to Taher and Olasoji et al., fractures caused by firearm bullets and assault appear to be the most usual cause of facial fracture in Iran and northeastern Nigeria. [20],[28]
RTCs are among the major factor of maxillofacial injuries and according to the results of previous studies the reason of 14.8-90.2% of all the skeletal and soft tissues injuries of the face. [1],[2],[3],[4],[5],[6],[7],[8],[9],[10],[12],[26] Adeyemo et al., and Fasola et al., noted that RTCs were major cause of death and injury, especially in low and middle-income countries. [6],[7] It is estimated that road traffic injuries will have risen from ninth to third in world disease burden rankings by 2020, accounting for 2.3 million deaths globally. In developed nations, progress in technology has resulted in more personal and vehicle protective measures being implemented coupled with access to proper medical care, good road and transport facilities; and regular enforcement of traffic rules and regulations. [9],[10],[23] The reverse scenario exists in developing countries especially of sub-Saharan Africa which has led to an increase in mortality and morbidity associated with RTCs. [5],[16],[17],[18]
The other significant etiologic factors of injuries to the maxillofacial region are assaults/interpersonal violence, falls, sport, industrial, gunshot/warfare, animal, iatrogenic, and suicide/self-inflicted. [1],[2],[5],[23],[29]
Reported frequency of facial fractures due to RTC varies from 14.8 to 90.2%. [1],[2],[3],[4],[5],[6],[7],[8],[9],[16],[17],[18] The current study finding of 87.5% of road traffic collision is similar to that of Kadkhodaie [15] in a recent Iranian study that found 91% of their facial fracture attributed to RTC. This result also comparable with many Nigerian [5],[6],[7],[8] and Middle Eastern studies [16],[17],[18] that demonstrated RTCs as the most frequent cause of facial fractures. [1],[2],[5],[6] Our finding of over 50% of RTC involved head-to-head collision of motorcycles and is reflected by the high frequency of riders involved than pillion passengers which confirmed the works of Oginni et al., [30] and Ramli et al. [27] In Sokoto metropolis and state as a whole, there is no established public transport system. Transport within the city (when not by foot) is mainly by motorcycles which operate as one-person taxis. This is quite lucrative and required low start-up capital and has subsequently, attracted many; particularly unskilled, illiterate, and unemployed youth who flock the city from many rural areas. Huelke and Compton stated that motorbike accidents are usually more serious than car accidents. [24] Increase in the use of motorbikes has led to a greater number of accidents and, consequently, multiple facial fractures. Adeyemo et al., [5] and other Nigerian authors [7],[30],[31] have raised alarm on the increasing menace of commercial motorcyclists on Nigerian roads. Saheeb and Etetafia and earlier Nigerian studies repeatedly cautioned that many commercial motorcyclists and motorists ignore the crash helmets/seatbelt regulations [5],[7],[30],[32] despite Nigerian Traffic Code imposition of stiff penalties against noncompliance with seat belts and crash helmet use. Additional problems mentioned are the overloading of passengers/pillions and goods, high speed, and imprudence among commercial motorcyclists (Okada) and motorists. [5],[30]
A recent Brazilian study [2] attributed their high frequency of RTCs to the fact that there population are largely rural and are farmers. Therefore, they travel great distance to transport their produce to the city most often in vehicles overloaded and not road worthy. We also face a similar scenario with our study population. Buses and taxis are infrequent and are generally only used for transport between cities. Other reasons postulated for the high frequency of RTCs include lack of street lights, inadequate road safety awareness, unsuitable road conditions without expansion of the motorway network, violation of speed limits, and old vehicles without safety features such as anti-burst locks and energy absorbing materials. [33] Furthermore, entry into opposite traffic lane without regard, violation of the right of the way, violation of the highway code, use of alcohol or other intoxicating agents, behavioral disorders, and poor socioeconomical conditions of some drivers. [2],[5],[23] Street lighting has been suggested as a relatively low cost intervention with the potential to prevent traffic crashes. [34]
In this study, for diagnosis of facial fracture we relied on clinical examination and conventional plain radiography. Adeyinka et al., noted that midfacial skeleton is much more difficult to assess using plain films than is the mandible. [35] The presence of thin bones, fluid-filled spaces (e.g., congested sinuses), and soft tissues (e.g., orbital contents) make accurate assessment difficult with images that do not offer a high degree of contrast. [5],[6] Our low utilization of advance imaging for maxillofacial fractures (e.g., computed tomography (CT) scan) is due to poor socioeconomic condition of the study population as health is paid for out of pocket. An average CT scan in Sokoto costs 25,000 Naira (about $160) which is quite exorbitant for most categories of our patients who are predominantly low socioeconomic class.
Reports in the literature noted that the pattern, incidence, and severity of facial fractures due to RTC often depend on mechanism of injury and mode of transportation predominant in that region. [2],[5] Over half of the proportion of facial fractures in this study were mandibular fractures followed by fractures of the zygomatic complex and maxillary bones. This is in agreement with most studies, [2],[3],[4],[5],[6],[7],[8],[9] but contradicts that of Ravindra and Ravindra Nair [1] and others from economically advanced countries where midfacial fractures were more frequently diagnosed. [9],[10],[12],[36] It is mentioned in the maxillofacial literature that the mandible is more vulnerable to fracture owing to its mobility, open arch, atrophy after dental loss and conspicuousness in the lower part of the face. [5],[13] Hence, it takes part in the mechanism of hyperextension and hyperflexion of the head in traffic crashes.
The present series showed that the body is the most fractured site in the mandible followed by parasymphysis. This is in accordance with recent Nigerian studies, [5],[6],[7],[8] but at variance with that of Ogundare [22] and elsewhere [13] that demonstrated angle and parasymphyseal fractures as the most common jaw fracture. This has been linked to the changing trends of etiology of facial fractures globally.
Analysis of our finding showed that the zygoma was the more commonly fractured midfacial bone which is comparable to the literature. [5],[7],[36] However, it contradicts the works of Gassner et al., that reported Le Fort and orbital fractures as the most frequently affected midfacial bone. [26] It should be highlighted that our result might be affected by the limitations of plain film in assessing midfacial fracture due to low contrast owing to presence of thin bones, fluid-filled spaces (e.g., congested sinuses), and soft tissues (e.g., orbital contents).
We found in this study high multiple facial injuries and concomitant head injury which is similar to the study of Posnic et al., but contrary to that of Singh et al. [13],[37] Severity of craniofacial injuries are directly related to the etiological agents. [1] RTCs have potentially lead to multiple facial and system injuries.
Our study revealed that the mandibular fracture treatment is by closed reduction with MMF and on a few occasion open reduction with transosseous wiring was employed. Stable zygomatic fractures were reduced by elevation, and unstable ones supported by antral packs. This treatment modality was chosen as in previous Nigerian reports [5],[6],[7],[8] based on affordability, availability, simplicity, and safety; and plethora of skill and armamentarium. Titanium plate osteosynthesis for facial fracture treatment has gained popularity worldwide and is the gold standard. [38],[39],[40],[41] In resource challenged environment however, adopting this trend has been quite difficult owing to the low socioeconomic status of our patients, high cost of acquisition, specialized training and skilled needed, and limited theater space for treatment under general anesthesia especially with other competing surgical specialties. [5],[42],[43] However, a recent review by Akadiri and Omitola [44] demonstrated that despite the drawbacks of closed reduction results obtained are satisfactory and quite comparable with titanium plate osteosynthesis of ORIF.
Limitations of the study
We had included in our study only those patients who were treated by the Oral and Maxillofacial Surgery unit. Those patients who were fatally injured did not figure in our study. Isolated nasal fractures are treated by the ear, nose, and throat (ENT) surgeons in our hospital which resulted in is none featuring in this article. Other parameters pertaining to maxillofacial injuries such as malocclusion, infections, and pseudoarthrosis were missing from our records; hence, making their analysis impossible. This we hope to correct in a future long-term cohort study.
| Conclusion | | |
In summary, RTC was the most frequent cause of facial fracture in our study cohort. A preponderance of male aged 21-30 years is in agreement with the literature. Furthermore, this current study highlights mandibular fractures as the most common in our environment and low utilization of ORIF in facial fracture treatment.
For a developing economy like ours, the burden of management of facial fractures can be enormous and unbearable. Hence, prevention is the best measure to reverse this scenario. These include road safety and traffic education to create awareness among our road users with the desire to achieve paradigm behavioral shift that will reduce accidents and carnage on our highways.
Transportation and traffic services affect all parts of the society and all individuals daily. Therefore, a multisectoral strategy that will involve the media, road safety and traffic managers, engineers, town planners, politicians, policy makers, road and motorcycle workers' unions, private companies, nongovernmental organizations, and civil associations will facilitate these preventive measures and help to educate road users to be thoughtful and conscious in traffic and to have a responsible and civil attitude to avoid accidents.
Recommendations
This study recommends the following:
- Establishment of functional and affordable intra- and intercity public transport system
- Incorporation of teaching of traffic rules and regulations in our school curriculum at all level of our educational system
- Education and training of road users on adoption of road safety measures such as seatbelt, crash helmet, drunk/drug driving, overspeeding; and strict reenforcement of road traffic regulations
- Making computer tomography scan more affordable to the generality of the public and extending health insurance coverage both in scope and persons
- Increasing facilities and provision of theater spaces for facial fractures management. Making titanium plates and screws affordable; thereby, facilitating the adoption of ORIF in the treatment of facial fractures.
| References | | |
| 1. | Ravindran V, Ravindran Nair KS. Metaanalysis of maxillofacial trauma in the northern districts of kerala: One year prospective study. J Maxillofac Oral Surg 2011;10:321-7. 
|
| 2. | Krishnaraj S, Chinnasamy R. A 4-year retrospective study of mandibular fractures in a South Indian city. J Craniofac Surg 2007;18:776-80.
|
| 3. | Paes JV, de Sá Paes FL, Valiati R, de Oliveira MG, Pagnoncelli RM. Retrospective study of prevalence of face fractures in southern Brazil. Indian J Dent Res 2012;23:80-6.
[PUBMED]  |
| 4. | Naveen Shankar A, Naveen Shankar V, Hegde N, Sharma, Prasad R. The pattern of the maxillofacial fractures-A multicentre retrospective study. J Craniomaxillofac Surg 2012;40:675-9.
|
| 5. | Adeyemo WL, Iwegbu IO, Bello SA, Okoturo E, Olaitan AA, Ladeinde AL, et al. Management of mandibular fractures in a developing country: A review of 314 cases from 2 Urban Centres in Nigeria. World J Surg 2008;32:2631-5.
|
| 6. | Adeyemo WL, Ladeinde AL, Ogunlewe MO, James O. Trends and characteristics of oral and maxillofacial injuries in Nigeria: A review of literature. Head Face Med 2005;1:7.
|
| 7. | Fasola AO, Nyako EA, Obiechina AE, Arotiba JT. Trends in the characteristics of maxillofacial fractures in Nigeria. J Oral Maxillofac Surg 2003;61:1140-3.
|
| 8. | Ugboko VI, Odusanya SA, Fagade OO. Maxillofacial fractures in a semi-urban Nigerian teaching hospital. A review of 442 cases. Int J Oral Maxillofac Surg 1998;27:286-9.
|
| 9. | Kontio R, Suuronen R, Ponkkonen H, Lindqvist C, Laine P. Have the causes of maxillofacial fractures changed over the last 16 years in Finland? An epidemiological study of 725 fractures. Dent Traumatol 2005;21:14-9.
|
| 10. | Dimitroulis G, Eyre J. A 7-year review of maxillofacial trauma in a central London hospital. Br Dent J 1991;170:300-2.
|
| 11. | Breeze J, Gibbons AJ, Hunt NC, Monaghan AM, Gibb I, Hepper A, et al. Mandibular fractures in British military personnel secondary to blast trauma sustained in Iraq and Afghanistan. Br J Oral Maxillofac Surg 2011;49:607-11.
|
| 12. | Haug RH, Prather J, Indresano AT. An epidemiologic survey of facial fractures and concomitant injuries. J Oral Maxillofac Surg 1990;48:926-32.
|
| 13. | Sing G, Mohammad S, Pal US, Hariram, Malkunje LR, Sing N. Pediatric facial injuries: It's management. Natl J Maxillofac Surg 2011;2:156-62.
|
| 14. | Available from: www.wikipedia.org/wiki/Sokoto_state. [Last accessed date on 2013 Apr 11].
|
| 15. | Kadkhodaie MH. Three-year review of facial fractures at a teaching hospital in northern Iran. Br J Oral Maxillofac Surg 2006;44:229-31.
[PUBMED] |
| 16. | Al Ahmed HE, Jaber MA, Abu Fanas SH, Karas M. The pattern of maxillofacial fractures in Sharjah, United Arab Emirates: A review of 230 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2004;98:166-70.
|
| 17. | Klenk G, Kovacs A. Etiology and patterns of facial fractures in the United Arab Emirates.J Craniofac Surg 2003;14:78-84.
|
| 18. | Al-Khateeb T, Abdullah FM. Craniomaxillofacial injuries in the United Arab Emirates: A retrospective study. J Oral Maxillofac Surg 2007;65:1094-101.
|
| 19. | Ansari MH. Maxillofacial fractures in Hamedan province, Iran: A retrospective study (1987-2001). J Craniomaxillofac Surg 2004;32:28-34.
|
| 20. | Olasoji HO, Tahir A, Arotiba GT. Changing picture of facial fractures in northern Nigeria. Br J Oral Maxillofac Surg 2002;40:140-3.
|
| 21. | Tanaka N, Tomitsuka K, Shionoya K, Andou H, Kimijama Y, Tashiro T, et al. Aetiology of maxillofacial fractures. Br J Oral Maxillofac Surg 1994;32:19-23.
|
| 22. | Ogundare BO, Bonnick A, Bayley N. Pattern of mandibular fractures in an urban major trauma center. J Oral Maxillofac Surg 2003;61:713-8.
|
| 23. | Malara P, Malara B, Drugacz J. Characteristics of maxillofacial injuries resulting from road traffic accidents: A 5 year review of the case records from Department of Maxillofacial Surgery in Katowice, Poland. Head Face Med 2006;2:27.
|
| 24. | Huelke DF, Compton CP. Facial injuries in automobile crashes. J Oral Maxillofac Surg 1983;41:241-4.
|
| 25. | Adebayo ET, Ajike OS, Adekeye EO. Analysis of the pattern of maxillofacial fractures in Kaduna, Nigeria. Br J Oral Maxillofac Surg 2003;41:396-400.
|
| 26. | Gassner R, Tuli T, Hachl O, Rudisch A, Ulmer H. Cranio-maxillofacial trauma: A 10 year review of 9,543 cases with 21,067 injuries. J Craniomaxillofac Surg 2003;31:51-61.
|
| 27. | Ramli R, Abdul Rahman R, Abdul Rahman N, Abdul Karim F, Krsna Rajandram R, Mohamad MS, et al. Pattern of maxillofacial injuries in motorcyclists in Malaysia. J Craniofac Surg 2008;19:316-21.
|
| 28. | Taher AA. Management and complications of middle and upper-third facial compound injuries: An Iranian experience. J Craniofac Surg 1993;4:153-61.
[PUBMED] |
| 29. | Bamjee Y, Lownie JF, Cleaton-Jones PE, Lownie MA. Maxillofacial injuries in a group of South Africans under 18 years of age. Br J Oral Maxillofac Surg 1996;34:298-302.
|
| 30. | Oginni FO, Ugboko VI, Ogundipe O, Adegbehingbe BO. Motorcycle-related maxillofacial injuries among Nigerian intracity road users. J Oral Maxillofac Surg 2006;64:56-62.
|
| 31. | Adegbehingbe BO, Oluwadiya KS, Adegbehingbe OO. Motorcycle associated ocular injuries in Ile-Ife, Nigeria. Afr J Trauma 2004;2:35-9.
|
| 32. | Saheeb BD. Influence of positions on the incidence and severity of maxillofacial injuries in vehicular crashes. West Afr J Med 2003;22:146-9.
|
| 33. | Subhashraj K, Nandakumar N, Ravindran C. Review of maxillofacial injuries in Chennai, India: A study of 2748 cases. Br J Oral Maxillofac Surg 2007;45:637-9.
|
| 34. | Beyer FR, Ker K. Street lighting for preventing road traffic injuries. Cochrane Database Syst Rev 2009:CD004728.
|
| 35. | Adeyinka AO, AgunloyeAkintoye AM, Osuagwu YU, Okoje V. Classification of Mid-facial fractures on a computed Tomography following head injury in a Nigerian population. West Afr J Radio 2011;18:25-37.
|
| 36. | Yoffe T, Shohat I, Shoshani Y, Taicher S. Etiology of maxillofacial trauma: A 10-year survey at the Chaim Sheba Medical Center, Tel-Hashomer. Harefuah 2008;147:192-6.
|
| 37. | Posnick JC, Wells M, Pron GE. Pediatric facial fractures: Evolving patterns of treatment. J Oral Maxillofac Surg 1993;51:836-44.
|
| 38. | Saluja H, Kini Y, Mahindra U, Kharkar V, Rudagi BM, Dehane V. A comparative evaluation of different treatment modalities for parasymphysis fractures: A pilot study. Int J Oral Maxillofac Surg 2012;41:906-11.
|
| 39. | Cawood JI. Small plate osteosynthesis of mandibular fractures. Br J Oral Maxillofac Surg 1985;23:77-91.
[PUBMED] |
| 40. | Dodson TB, Perrott DH, Kaban LB, Gordon NC. Fixation of mandibular fractures: A comparative analysis of rigid internal fixation and standard fixation techniques. J Oral Maxillofac Surg 1990;48:362-6.
|
| 41. | Andreasen JO, Storgard Jensen S, Kofod T, Schwartz O, Hillerup S. Open or closed repositioning of mandibular fractures: Is there a difference in healing outcome? A systematic review. Dent Traumatol 2008;24:17-21.
|
| 42. | Dillon JK, Christensen B, McDonald T, Huang S, Gauger P, Gomez P. The financial burden of mandibular trauma. J Oral Maxillofac Surg 2012;70:2124-34.
|
| 43. | Al-Belasy FA. A short period of maxillo-madibular fixation for treatment of fractures of the mandibular tooth-bearing area. J Oral Maxillofac Surg 2005;63:953-6.
[PUBMED] |
| 44. | Akadiri OA, Omitiola OG. Maxillo-mandibular fixation: Utility and current techniques in modern practice. Niger J Med 2012;21:125-33.
|
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
[Table 1], [Table 2], [Table 3]
|