|


 |
| CASE REPORT |
|
| Year : 2014 | Volume
: 6
| Issue : 1 | Page : 33-36 |
|
|
Massive spontaneous hemothorax, giant intrathoracic meningocele, and kyphoscoliosis in neurofibromatosis type 1
Ayodeji Salman Yusuf1, Ashok Pillai2, Sajesh K Menon2, Dilip Panikar2
1 Department of Surgery, Neurosurgery Unit, University of Ilorin and University of Ilorin Teaching Hospital, Ilorin, Nigeria,
2 Department of Neurosurgery, Amrita Institute of Medical Sciences and Research Centre, Cochin, Kerala, India,
| Date of Web Publication | 24-Jun-2014 |
Correspondence Address:
Ayodeji Salman Yusuf
Department of Surgery, Faculty of Clinical Sciences, University of Ilorin and University of Ilorin Teaching Hospital, Ilorin, Nigeria
 Source of Support: None, Conflict of Interest: None
DOI: 10.4103/2006-8808.135151

 Abstract Abstract | | |
Neurofibromatosis type 1 (NF-1) is a heterogeneous autosomal dominant disease with an incidence ranging from 1 in 2500 to 1 in 3000. Rare intrathoracic vascular disorders resulting in massive spontaneous hemothorax with fatal consequences may occur in these patients, so also are various types of skeletal dysplasia which may result in dramatic presentations, posing management challenges to the attending physicians. We report the case of a 43-year-old woman with NF-1 who developed spontaneous massive hemothorax and was discovered to have a concurrent giant intrathoracic meningocele and thoracic kyphoscoliosis with severe vertebral dysplastic changes. Surgical treatment via a right thoracotomy with primary repair of the meningocele and spinal fusion with fibula graft resulted in good outcome. This case represents an extreme manifestation of this otherwise indolent disease in clinical practice. Keywords: Hemothorax, kyphoscoliosis, meningocele, spinal fusion
How to cite this article:
Yusuf AS, Pillai A, Menon SK, Panikar D. Massive spontaneous hemothorax, giant intrathoracic meningocele, and kyphoscoliosis in neurofibromatosis type 1. J Surg Tech Case Report 2014;6:33-6 |
How to cite this URL:
Yusuf AS, Pillai A, Menon SK, Panikar D. Massive spontaneous hemothorax, giant intrathoracic meningocele, and kyphoscoliosis in neurofibromatosis type 1. J Surg Tech Case Report [serial online] 2014 [cited 2016 May 10];6:33-6. Available from: http://www.jstcr.org/text.asp?2014/6/1/33/135151 |
| Introduction | |  |
Neurofibromatosis type 1 (NF-1) is an autosomal dominant disease with an incidence ranging from 1 in 2500 to 1 in 3000. [1] The disease is clinically heterogeneous and most commonly affects the nervous system, skin, and skeletal tissues. Well-defined vascular lesions of small and large vessels also occur with a reported incidence of 3.6%. [2] The phenotypic heterogeneity results in numerous unpredictable complications. [2] There are few reports of spontaneous massive hemothorax in NF-1 with mortality as high as 36%. [3],[4] Scoliosis affects 10% of NF-1 and is the most common skeletal manifestation of the disease. [1],[5],[6] Neurological involvement with severe myelopathy and even acute paralysis has been reported. Intrathoracic meningoceles rarely occur and may be either asymptomatic or result in varying degrees of respiratory dysfunction. [7],[8]
We report the case of a 43-year-old woman with NF-1 who presented with massive spontaneous hemothorax and was found to have concurrent giant intrathoracic meningocele and thoracic kyphoscoliosis with severe vertebral dysplastic changes. She was treated surgically via a right thoracotomy with primary repair of meningocele and spinal fusion with fibula graft after initial stabilization. This represents an extreme manifestation of this otherwise indolent disease in clinical practice.
| Case report | | |
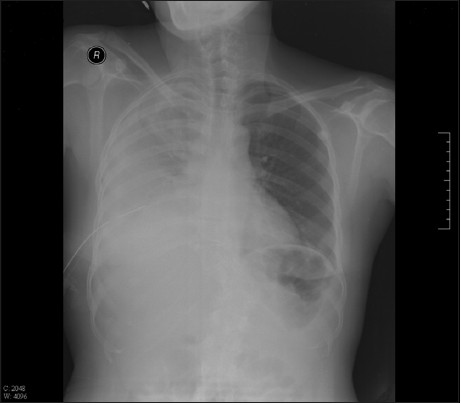
A 43-year-old woman with diagnostic features of NF-1 presented at a local hospital with sudden onset of dizziness, progressive breathlessness, and easy fatigability. There was associated excessive sweating and syncope. A chest radiograph revealed massive pleural effusion. An emergency tube thoracostomy drained large quantity of frank blood. She was resuscitated with intravenous crystalloids and blood transfusions and transferred to our hospital.
At presentation, she was pale, dyspneic, and tachypneic. Chest tube was in situ draining altered blood. There was clinical evidence of right-sided massive pleural effusion, which was confirmed subsequently with chest roentgenogram [Figure 1]. She had been having low back pain and scoliotic deformity for 15 years, but had never sought any medical advice. The diagnostic features of NF-1 in her included: (1) Multiple café-au-lait spots, (2) multiple cutaneous neurofibromas, (3) Lisch nodule on slit-lamp examination, and (4) positive family history (daughter). There were no motor or sensory deficits and she had no other co-morbidity.
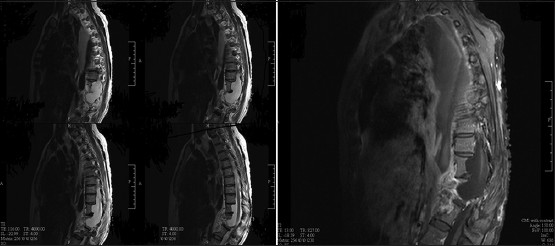
She was further evaluated with thoracolumbar plain radiograph, computed tomography, and magnetic resonant imaging. These revealed a kyphoscoliotic deformity involving D10-D12, thinning of adjacent ribs [Figure 2]a and b], and a large anterolateral meningocele at D11-D12 level with severe posterior vertebral body scalloping and spinal canal widening at the same level [Figure 3]. | Figure 2: (a) Thoracolumbar plain radiograph; (b) chest computed tomography scan
Click here to view |
She was managed surgically via a right thoracotomy. Intraoperative findings included large amount of clotted blood in the pleural cavity and a large meningocele entering into the pleural space through a large lateral defect in the dysplastic vertebral bodies. The meningocele was covered by thickened layer of clotted blood products and surrounded by numerous dysplastic vessels (arterial and venous) leading to intercostal vessels. The involved vertebral bodies and adjoining ribs were soft and dysplastic. There were no actively bleeding vessels.
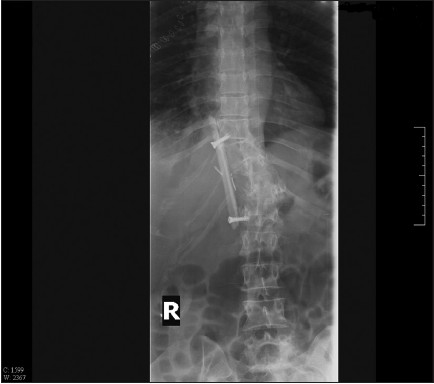
After primary repair of the meningocele, the spine was fused with right lateral strut graft using fibula bone graft from D9 to L1 vertebrae [Figure 4]. Decortication of the pleural cavity was done for long-term pleurodesis. The postoperative period was uneventful, and patient was symptom-free at the last follow-up 4 years after surgery with evidence of fusion on X-ray.
| Discussion | | |
Vascular lesions in NF-1 are rare but sometime fatal, with a reported incidence of 2-3.6%. [2] Spontaneous hemothorax with fatal consequences may arise from bleeding of dysplastic small vessels or rupture of an aneurysm of a major intrathoracic artery. Mortality rate of up to 36% and surgical mortality of 33% have been reported from such events. [3],[4] Among the intrathoracic vessels, the intercostal and subclavian arteries are the most commonly involved. Lynn et al. have reported a case of massive spontaneous hemothorax and have summarized 25 previous cases reported in literature. [3] Rarely, spontaneous hemothorax may result from benign and malignant thoracic tumors. [9]
There are multiple mechanisms described in the pathogenesis of a hemothorax in patients with NF-1. However, two distinct categories in relation to the diameter of the vessels are defined. Direct invasion of large vessels by adjacent tumors such as schwannomas, neurofibromas or neurofibrosarcomas resulting in intimal proliferation, thinning of the media, and fragmentation of elastic tissue, in turn leading to stenosis or aneurysm formation is thought to be responsible. Smaller vessels are thought to have a dysplasia in the wall itself, consisting of fibrohyaline thickening of the intima and muscularis which causes stenotic narrowing and subsequent significant weakening of the arterial wall. [3],[4],[10]
The treatment of spontaneous hemothorax depends on the hemodynamic stability of the patient. If the patient is in shock, immediate thoracotomy is required to control the intrathoracic hemorrhage after initial resuscitation. For a patient who is hemodynamically stable, an initial angiography to reveal the ruptured vessel and subsequent percutaneous embolization or coiling of aneurysms has shown superior outcome to surgery. [3] Although successful conservative treatment has been reported, the treatment modality suffers from limitations such as reported incidences of rebleeding and mortality in patients treated nonoperatively. [3],[10]
Intrathoracic meningocele in association with NF-1 is another relatively rare condition which was first described in 1933. [11] It is probably due to the generalized mesenchymal dysplasia in this disorder. A spinal meningocele is a saccular herniation of the meninges through a dilated intervertebral foramen or a defect in the vertebral column. In the thorax, lateral meningoceles are more frequent because the paravertebral muscles are relatively weak and the pressure gradient between cerebrospinal fluid and thorax is high. Most patients with anterior meningocele are asymptomatic; few patents present with back pain, cough, or dyspnea due to compression of the lung and mediastinal structures. [7],[8],[11] Symptoms depend on the size and location of the meningocele within the thorax. The spinal cord is rarely involved. Rupture of a giant meningocele resulting in hydrothorax has also been reported. [12] Occasionally, the cyst may be mistaken for a mediastinal tumor.
Surgical intervention is not required in isolated asymptomatic cases of intrathoracic meningoceles, although this case of severe manifestations from a spontaneous hemothorax would support operating on radiologically significant but clinically asymptomatic meningoceles. For symptomatic meningoceles, the treatment depends on the size and can be challenging because of underlying skeletal dysplasia.
Spinal deformity is the most common skeletal abnormality in NF-1. Scoliosis affects 10% of NF-1 patients and most commonly involves the lower cervical and upper thoracic spine. [1],[7] It can be either idiopathic or dystrophic. Dystrophic changes including rib penciling, vertebral scalloping, severe apical wedging and rotation, enlargement of the foramina, and paravertebral tumors are also classic abnormalities found in neurofibromatosis. [13] Spinal dislocation with development of neurological deficits has been reported in these patients. [14] An optimal surgical procedure for severe scoliosis in NF-1 has not been established. Early surgical fusion via an anterior or combined anterior and posterior approach has been advocated to prevent progression and spinal dislocation.
In our patient, multiple dysplastic small vessels were identified, but there were no actively bleeding vessels or aneurysms at surgery. Hemothorax may have resulted from rupture of any of these dysplastic vessels. Although the patient was hemodynamically stable after initial resuscitation, surgery was unavoidable given the extent of hemothorax.
Thoracotomy also allowed for excision and repair of the giant meningocele and simultaneous reinforcement of spinal stability by fusion with fibula graft. The fibular graft was used for spinal fusion in order to reinforce the soft dysplastic vertebral bone and hopefully prevent future dislocation and subsequent development of neurological deficit. The patient has remained symptom-free now for 4 years.
| References | | |
| 1. | Ferner RE. Neurofibromatosis 1 and neurofibromatosis 2: A twenty first century perspective. Lancet Neurol 2007;6:340-51. 
[PUBMED] |
| 2. | Miura H, Taira O, Uchida O, Usuda J, Hirai S, Kato H. Spontaneous haemothorax associated with von Recklinghausen's disease: Review of occurrence in Japan. Thorax 1997;52:575-8.
|
| 3. | Fedoruk LM, English J, Fradet GJ. Spontaneous hemothorax and neurofibromatosis: A review of a lethal combination. Asian Cardiovasc Thorac Ann 2007;15:342-4.
|
| 4. | Conlon NP, Redmond KC, Celi LA. Spontaneous hemothorax in a patient with neurofibromatosis type 1 and undiagnosed pheochromocytoma. Ann Thorac Surg 2007;84:1021-3.
|
| 5. | Tsirikos AI, Saifuddin A, Noordeen MH. Spinal deformity in neurofibromatosis type-1: Diagnosis and treatment. Eur Spine J 2005;14:427-39.
|
| 6. | Martín-Fuentes AM1, Pretell-Mazzini J, Curto de la Mano A, Viña-Fernández R. High-grade spondyloretrolisthesis in a 12-year-old girl with neurofibromatosis type 1: A case report and literature review. J Pediatr Orthop B 2013;22:110-6.
|
| 7. | Ebara S, Yuzawa Y, Kinoshita T, Takahashi J, Nakamura I, Hirabayashi H, et al. A neurofibromatosis type 1 patient with severe kyphoscoliosis and intrathoracic meningocele. J Clin Neurosci 2003;10:268-72.
|
| 8. | Sakamoto H1, Hoshino A, Ito K, Sakuraya M, Sato M, Sawada Y, et al. Intrathoracic giant meningocele associated with neurofibromatosis. Intern Med 2003;42:767-8.
[PUBMED] |
| 9. | Vaziri M, Mehrazma M. Massive spontaneous hemothorax associated with Von Recklinghausen's disease. Ann Thorac Surg 2006;82:1500-1.
|
| 10. | Pezzetta E, Paroz A, Ris HB, Martinet O. Spontaneous hemothorax associated with von Recklinghausen's disease. Eur J Cardiothorac Surg 2003;23:1062-4.
|
| 11. | Vanhauwaert DJ, Deruytter MJ. Cystoperitoneal shunt as alternative treatment for a giant thoracic meningocele in a patient with neurofibromatosis. Surg Neurol 2008;69:535-7.
|
| 12. | Mizuno J, Nakagawa H, Yamada T, Watabe T. Intrathoracic giant meningocele developing hydrothorax: A case report. J Spinal Disord Tech 2002;15:529-32.
|
| 13. | Singh K, Samartzis D, An HS. Neurofibromatosis type I with severe dystrophic kyphoscoliosis and its operative management via a simultaneous anterior-posterior approach: A case report and review of the literature. Spine J 2005;5:461-6.
|
| 14. | Rockower S, McKay D, Nason S. Dislocation of the spine in neurofibromatosis: A report of two cases. J Bone Joint Surg Am 1982;64:1240-2.
[PUBMED] |
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
|