|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2014 | Volume
: 9
| Issue : 1 | Page : 15-18 |
|
Radiation dose measurements during hysterosalpingography
Mohamed Yousef1, Jumaa Yousif Tambul1, Abdelmoneim Sulieman2
1 Department of Diagnostic Radiologic Technology, College of Medical Radiologic Science, Sudan University of Science and Technology, Khartoum, Sudan; Department of Diagnostic Radiologic Technology, College of Medical Applied Sciences, Taibah University, Almadinah Almunawwarah, Saudi Arabia
2 Department of Diagnostic Radiologic Technology, College of Medical Radiologic Science, Sudan University of Science and Technology, Khartoum, Sudan; Department of Radiology and Medical Imaging, College of Applied Medical Sciences, Salman Bin Abdul Aziz University, Al Kharj, Saudi Arabia
| Date of Web Publication | 13-Nov-2014 |
Correspondence Address:
Mohamed Yousef
Department of Diagnostic Radiologic Technology, College of Medical Radiologic Sciences, Sudan University of Science and Technology, P.O. Box 1908, Khartoum, Sudan
  | Check |
DOI: 10.4103/1858-5000.144652 
Objectives: Hysterosalpingography (HSG) is an effective method to evaluate abnormalities of the uterus and fallopian tube using conventional X-ray or fluoroscopy. The aim of this study was to determine and evaluate the radiation dose for females undergoing HSG during the reproductive period. Materials and Methods: This study conducted in three radiology departments: Omdurman Teaching Hospital, Alneelain Diagnostic Center and Asia Specialized Hospital. A total of 50 patients was studied from three hospitals, 20 patients from Neelain Diagnostic Center in range of (25-40) years, 20 patients from Omdurman teaching Hospital in age range from (24 to 43) years. The study duration was carried out for a period of 3 months, from March 2011 to June 2011. Patient dose measurements were performed using unfors dosimeter. Organ dose and effective doses were estimated using National Radiological Protection Board software. Results: The mean patient dose was 20.1 and 28.9 and 13. 6 Omdurman Teaching Hospital, Neelain Diagnostic Center and Asia Specialized Hospital, respectively. Ovaries and uterus have the highest dose compared to other organs. Conclusion: The results of this study are higher compared with previous studies. Keywords: Dose measurements, hystrosalpingography, ovaries, radiation, uterus
How to cite this article:
Yousef M, Tambul JY, Sulieman A. Radiation dose measurements during hysterosalpingography. Sudan Med Monit 2014;9:15-8 |
| Introduction | |  |
Hysterosalpingography (HSG) is an important diagnostic method for the evaluation of the female reproductive tract that involves the exposure of patients to ionizing radiation. It is a relatively frequent radiogynecological procedure, generally used to assess the uterine cavity and patency of Fallopian tube More Detailss.
The common indication for the use of HSG is primary and secondary infertility. [1],[2],[3],[4] HSG is merely an initial step in gynecoradiological procedures. Depending on the findings, one may proceed with selective salpingography, tubal catheterization, or a similar therapeutic procedure. [5] In all radiological procedures in gynecology, their radiation of ovaries is unavoidable and one should, thus, consider both the radiation exposure of the patient and the radiological risks associated with it for the fetus and born child during the period of growth.
Concerns over radiation doses received by patients and the associated radiation risks have become a major issue in recent years. [6],[7] The contribution of HSG to the collective dose is not significant; [8],[9] however, good radiation protection is of utmost importance at the individual level, as the said examination involves the irradiation of females of reproductive capacity and of the gonadal region of relatively young patients, with a possibility for repeated examinations.
There are several studies on dose levels from HSG, mainly from screen-film radiological units. Assessed dose levels are commonly reported in terms of an easily measured entrance surface dose (ESD) or dose-area product. [10],[11] However, it is just as important to estimate organ and effective doses as quantities directly related to the radiological risk. In the available literature, reported entrance surface air kerma for the HSG procedure is in the range of 9.7-30 mGy while reported kerma-area product values range from 4 to 7 Gycm 2 . [1],[4],[8],[9],[12],[13] A typical effective dose to the patient undergoing HSG as a part of infertility work-up is 1.2 mSv to 3.1 mSv, with the ovarian dose in the range of 2.7-9.0 mGy. However, higher values of the effective dose (8 mSv) and corresponding ovarian dose (9-11 mG) were also reported. [1],[2],[13] Furthermore, the ovarian dose can be as high as 45 mGy, [1] which certainly requires careful analysis and application of dose reduction strategies.
The aim of this study was to determine and evaluate the radiation dose for females during the reproductive period undergoing HSG.
| Materials and methods | | |
A total of 50 patients was examined from three hospitals, 20 patient from Alneelain Diagnostic Center in range (25-40) years, 20 patient from Omdorman teaching Hospital in range from (24 to 43) years.
Materials
X-ray machines [Table 1]
Lead aprons for technologist, with 0.5 mm thickness which is made in Japan.
Hysterosalpingography procedure
Patient lies supine on the table in lithotomic position bends her knees and places her feet at the end of the table. A vaginal speculum inserted into the vagina, the vaginal walls and cervix are cleaned with antiseptic solution. A cannula inserted into the cervical canal, which attached with syringe fill with contrast media (CM), inject CM into the uterine cavity. If the uterine tubes are patent, CM will flow from distal end of the tubes to peritoneal cavity there are four images recorded during conventional radiography using 10 × 12 inch films with vertical center rays 5 cm superior to symphysis pubis (anteroposterior [AP] plain radiograph, AP film with CM to show the uterus. AP film with CM to show the uterine tubes. AP film with CM to show spill of CM in the peritoneal cavity).
Absorbed dose calculations
Entrance surface doses in this study were calculated using DoseCalc software {developer: BawDuction Software, 2014} developed by the radiological protection center of Saint George' Hospital, London, this software is extensively used to calculate patient dose in diagnostic radiology. For dose measurement using the software, the relationship between X-ray unit current time product (mAs) and the air kerma free in air was established at a reference point of 100 cm from tube focus for the range of tube potentials encountered in clinical practice, the X-ray tube output was measured in (mGy/mAs) using Unfors Xi Dosimeter (Unfors Inc., Billdal, Sweden) with accuracy better than 5%. ESD was calculated according to the following formula:
| Results | | |
The blockage of tubes is the most common indication in this study which was 24% of total number of patients (in Al neelain diagnostic center which 25%, 10% in Asia hospital and 30% in Omdurman teaching hospital), and recurrent abortion 12% in total number of patients (15% in Alneelain diagnostic center, 30% in Asia hospital) [Table 2] and [Table 3]. | Table 2: Patient body characteristics (age, height, BMI, and weight), screening time and number of radiographic images (mean and range in parentheses)
Click here to view |
The HSG indications are initial diagnosis for blockage of tubes, inversus uterus, salpingitis, blind external os, recurrent abortion, and bicornuate uterus.
| Discussion | | |
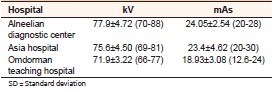
This study intended to provide a detailed evaluation of radiation dose during HSG and to analyze factors that might affect the radiation dose for patients. Patient body characteristics data (age, height, weight, and body mass index [BMI]) [Table 2] in this study, the patient age ranged (25-40) years in alneelain diagnostic center, (24-43) years in Omdurman teaching hospital and (27-43) years in Asia. The mean height, weight, and BMI in alneelian medical center were 1.7 m, 73.2 kg, 26.2 kg/m 2 , in Omdurman teaching hospital were 1.6 m, 72.9 kg, 27.6 kg/m 2 and in Asia hospital were 1.6 m, 74.3 kg, 28 kg/m 2 , respectively. The number of films depend on the pathologic conditions. The exposure factors (kVp, mAs) for all patients were comparable in three hospitals. In general, high kVp increase the scatter radiation thus also the patient's dose, while decreasing the contrast of the image. The quality of the radiation depends on the tube voltage and the total filtration of the X-ray beam. Radiographic exposure factors used in this study ranged 69-88 kVp and 12.6-30 mAs (the highest kVp used in Alneelain diagnostic center which is 88 kVp and the lowest kVp used in Omdurman teaching hospital which is 66 kVp, the highest mAs used in Asia which is30 mAs and the lowest mAs used in Omdurman teaching hospital which is12.6 mAs) [Table 3].
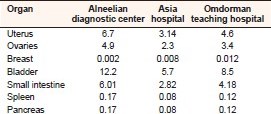
The mean ESD and E resulting from HSG procedure has been estimated to be 20.9 mGy and 1.94 mSv, respectively, for the total patient population table. The mean ESD result for all patients is higher than the previous study [Table 5]. This result indicates that a low degree of patient dose achieved in the previous studies. The effective dose in this study estimated to be 1.94 mSv higher than Sulieman et al. 0.43 mSv. [2] As HSG involves direct irradiations of some of the internal and radiosensitive organs, effective doses for specific organs were estimated are illustrated in [Table 4]. Ovaries, uterus, and bladder dose which receives radiation was estimated as 4.9, 6.7, 12.2 mGy in Alneelian diagnostic center, 2.3, 3.14, 5.7 mGy in Asia hospital and 3.4, 4.6, 8.5 mGy, respectively, in Omdurman teaching hospital. The equivalent dose for the breast is very low value because the breast too far away field of view "pelvis region." The bladder doses is the highest one.
| Conclusions | | |
This study measured the patient doses during HSG in three hospitals in Khartoum state. The mean ESD result for all patients is higher than the previous studies. The dose values showed wide variation in the three hospitals. This can be attributed to the machine characteristics, technique, and operator experiences. Optimization technique is important in order to reduce patient doses to the international levels.
| References | | |
| 1. | Gregan AC, Peach D, McHugo JM. Patient dosimetry in hysterosalpingography: A comparative study. Br J Radiol 1998;71:1058-61.  |
| 2. | Sulieman A, Theodorou K, Vlychou M, Topaltzikis T, Roundas C, Fezoulidis I, et al. Radiation dose optimisation and risk estimation to patients and staff during hysterosalpingography. Radiat Prot Dosimetry 2008;128:217-26. |
| 3. | Kramer R, Khoury HJ, Lopes C, Vieira JW. Equivalent dose to organs and tissues in hysterosalpingography calculated with the FAX (Female Adult voXel) phantom. Br J Radiol 2006;79:893-9. |
| 4. | Perisinakis K, Damilakis J, Grammatikakis J, Theocharopoulos N, Gourtsoyiannis N. Radiogenic risks from hysterosalpingography. Eur Radiol 2003;13:1522-8. |
| 5. | Karande VC, Pratt DE, Balin MS, Levrant SG, Morris RS, Gleicher N. What is the radiation exposure to patients during a gynecoradiologic procedure? Fertil Steril 1997;67:401-3. |
| 6. | Rehani M, Frush D. Tracking radiation exposure of patients. Lancet 2010;376:754-5. |
| 7. | Holmberg O, Malone J, Rehani M, McLean D, Czarwinski R. Current issues and actions in radiation protection of patients. Eur J Radiol 2010;76:15-9. |
| 8. | UNSCEAR. United Nations Scientific Committee on the Effects of Atomic Radiation 2008 Report to General Assembly. New York: UNSECAR; 2010. |
| 9. | NCRP. Ionizing Radiation Exposure of the Population of the United States, NCRP Report 160. Bethesda, Md, USA: The National Council on Radiation Protection and Measurements; 2009. |
| 10. | International Atomoc Energy Agency. Dosimetry in Diagnostic Radiology: An International Code of Practice. Technical Report Sertiea No. 457, Vienna: IAEA; 2007. |
| 11. | Stankovi K, Vujisi M. Influence of Radiation Energy and Angle of Incidence on the Uncertainty in Measurements by GM Counters. Nucl Technol Radiat Prot 2008;23:41-2. |
| 12. | Fife IA, Wilson DJ, Lewis CA. Entrance surface and ovarian doses in hysterosalpingography. Br J Radiol 1994;67:860-3. |
| 13. | Fernández JM, Vañó E, Guibelalde E. Patient doses in hysterosalpingography. Br J Radiol 1996;69:751-4. |
[Table 1], [Table 2], [Table 3], [Table 4], [Table 5]
| This article has been cited by | | 1 |
Two-dimensional and three-dimensional imaging of uterus and fallopian tubes in female infertility |
|
| Patricia Carrascosa,Carlos Capuñay,Javier Vallejos,Jimena Carpio,Mariano Baronio,Sergio Papier | | Fertility and Sterility. 2016; | | [Pubmed] | [DOI] | | | 2 |
Estimation of effective dose during hystrosalpingography procedures in certain hospitals in Sudan |
|
| K. Alzimami,A. Sulieman,E. Babikir,K. Alsafi,M. Alkhorayef,Hiba Omer | | Applied Radiation and Isotopes. 2015; 100: 2 | | [Pubmed] | [DOI] | |
|




 |
|
|
|




 Search Pubmed for
Search Pubmed for