|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 10
| Issue : 1 | Page : 11-16 |
|
A comparative study between ropivacaine 30 ml (0.75%) and ropivacaine 30 ml (0.75%) with clonidine 150 μg as an adjuvant in brachial plexus block through supraclavicular approach
Shobhana Gupta1, Hina Niraj Gadani1, HG Thippeswamy2
1 Department of Anaesthesiology, GMERS Medical College, Gandhinagar, Gujarat, India
2 Department of Anaesthesiology, SDMCMSH, Sattur, Dharwad, Karnataka, India
| Date of Web Publication | 21-May-2015 |
Correspondence Address:
Hina Niraj Gadani
Department of Anaesthesiology, GMERS Medical College, Gandhinagar, Gujarat
India
  | Check |
DOI: 10.4103/1858-5000.157504 
Background: Ropivacaine is a novel alternative to bupivacaine with the less cardiovascular system and central nervous system toxicity. Clonidine, an alpha 2 agonist, may have benefited patients when it is injected at peripheral nerve sites with local anesthetic ropivacaine. Clonidine is second only to epinephrine as a useful adjuvant for brachial plexus blockade. Objective: A clinical study was carried out to compare the anesthetic effects of ropivacaine alone and clonidine as an adjuvant to ropivacaine in brachial plexus block for upper limb surgeries. Materials and Methods: A comparative, double-blind, prospective, randomized, clinical study was carried out on 60 patients of either sex of American Society of Anesthesiologist physical status I and II, with age group 25-65 years undergoing various orthopedic surgeries of upper limb under supraclavicular brachial plexus block. Patients were randomly allocated to either of the two groups of 30 each. Group-R: Injection ropivacaine 30 ml (0.75%) with 1 ml normal saline. Group-ropivacaine clonidine (RC): Iinjection ropivacaine 30 ml (0.75%) with injection clonidine 1 ml (150 μg). Heart rate, mean arterial pressure, onset and duration of motor and sensory blockade were observed during preoperative, intraoperative and postoperative period. At the end of the study, the data were analyzed using Chi-square test for qualitative data and Student t-test. P < 0.05 was considered significant and P < 0.01 was considered as highly significant. Results: Demographic and hemodynamic data were comparable. Onset of sensory and motor block was significantly earlier in Group-R. Duration of analgesia and motor blockade was prolonged in the RC group. Both groups were observed for the side-effects, which were not significant. Conclusions: Addition of clonidine 150 μm to ropivacaine 0.75% 30 ml delays the onset of sensory and motor blockade while prolongs the postoperative motor blockade and analgesia significantly without producing any clinical significant side-effects in brachial plexus block through supraclavicular approach. Keywords: Brachial plexus block, clonidine, ropivacaine, supraclavicular approach
How to cite this article:
Gupta S, Gadani HN, Thippeswamy H G. A comparative study between ropivacaine 30 ml (0.75%) and ropivacaine 30 ml (0.75%) with clonidine 150 μg as an adjuvant in brachial plexus block through supraclavicular approach. Sudan Med Monit 2015;10:11-6 |
How to cite this URL:
Gupta S, Gadani HN, Thippeswamy H G. A comparative study between ropivacaine 30 ml (0.75%) and ropivacaine 30 ml (0.75%) with clonidine 150 μg as an adjuvant in brachial plexus block through supraclavicular approach. Sudan Med Monit [serial online] 2015 [cited 2018 Sep 5];10:11-6. Available from: http://www.sudanmedicalmonitor.org/text.asp?2015/10/1/11/157504 |
| Introduction | |  |
Brachial plexus block for upper limb surgeries is an advantageous, as the effect of the drug is limited to the part of the body to be operated upon. It is devoid of complications associated with general anesthesia like nausea, vomiting, aspiration pneumonitis, urinary retention, etc. It also provides early enteral feeding and ambulation, thereby reducing postoperative complications and hospital stay. It produces dense anesthesia with good muscle relaxation and relieves tourniquet pain thus satisfying the surgeon and patient.
Supraclavicular brachial plexus block provides anesthesia for surgeries around elbow, forearm and hand. This technique was chosen for upper limb surgeries in our study. Bupivacaine was in clinical use for close to 10 years before serious cardiac toxicity was reported. Several deaths were reported in obstetric patients in the United States in the 1970s. [1] Ropivacaine is a novel alternative to bupivacaine. The well-known cardiovascular system and central nervous system adverse effects of bupivacaine seem to be less with ropivacaine when comparable plasma levels of this drug are reached. [2],[3]
Recent reports pointed out that clonidine, an alpha 2 agonist may have benefited patients when it was injected at peripheral nerve sites. Analgesia with clonidine lasted longer than analgesia obtained with epinephrine. [4],[5] Brachial plexus clonidine 150 μg delays the onset of pain by two-fold, when compared with systemic control, and 0.5 μg/kg prolongs analgesia by 50% compared with placebo. [6],[7]
| Materials and methods | | |
After getting clearance from Institutional Ethics Committee, a comparative, double-blind, prospective, randomized, clinical study was carried out on 60 patients of either sex undergoing various orthopedic surgeries of upper limb under supraclavicular brachial plexus block using a mixture of injection ropivacaine 30 ml (0.75%) with 1 ml normal saline and injection ropivacaine 30 ml (0.75%) with injection clonidine 1 ml (150 μg). The Patients included in the study belonged to American Society of Anaesthesiologist physical status I and II of age group 25-65 years. Patients are having a history of hypertension, diabetes mellitus, coagulation abnormalities, on antiplatlet/anticoagulation therapy, allergy to local anesthetics, obese and pregnant patients were excluded from the study.
After taking written informed consent, patients were randomly allocated to either of the 2 groups of 30 each. Group-R: Injection ropivacaine 30 ml (0.75%) with 1 ml normal saline. Group-ropivacaine clonidine (RC): Injection ropivacaine 30 ml (0.75%) with injection clonidine 1 ml (150 μg).
Prior to injection, pulse, blood pressure, respiratory rate, oxygen saturation and sedation score were recorded. Assessment of sensory blockade was done at 0 min, 1 min, 2 min, 3 min, 4 min, 5 min, 6 min, and 6.5 min till 15 min after completion of drug injection in skin areas innervated by median nerve, radial nerve, ulnar nerve and musculocutaneous nerve.
Motor blockade was determined according to a modified Bromage scale for upper extremities. 0 = able to move normally, 1 = inability to move wrist and/or elbow against resistance, 2 = inability to lift wrist and/or elbow against resistance, 3 = inability to move entire arm. The block was considered incomplete, when any of the segments supplied by median, radial, ulnar and musculocutaneous nerves were not anesthetized even after 30 min of drug injection.
Sedation score was assessed by using the sedation scale described by Culebras et al., (1) awake and alert, (2) sedated, responding to verbal stimulus, (3) sedated, responding to mild physical stimulus, (4) sedated, responds to moderate or severe physical stimulus.
During intraoperative period patients were monitored for pulse rate, blood pressure, respiratory rate, and oxygen saturation. In postoperative period pulse rate, blood pressure, respiratory rate, sedation score were noted. Patients were examined for the duration of analgesia as per visual analog scale (VAS). VAS score is the most commonly used methods of assessing acute pain and its relief. Postoperatively at every 2 h VAS score was noted, and when it is ≥4, rescue analgesia was given in the form of injection diclofenac sodium 1.5 mg/kg intramuscularly and time of rescue analgesia was noted.
All the patients were observed for the incidence of any side-effects and complications such as nausea, vomiting, pneumothorax, hematoma, local anesthetic toxicity and postblock neuropathy.
Statistical analysis
Statistical analysis was performed using Chi-square test for qualitative data and Student t-test. P < 0.05 was considered significant and P < 0.01 was considered as highly significant.
| Results | | |
[Table 1] shows demographic data which was comparable in both groups.
[Table 2] shows time to onset of sensory and the motor blockade, which was delayed in Group-RC and statistically significant (P < 0.05) between two groups.
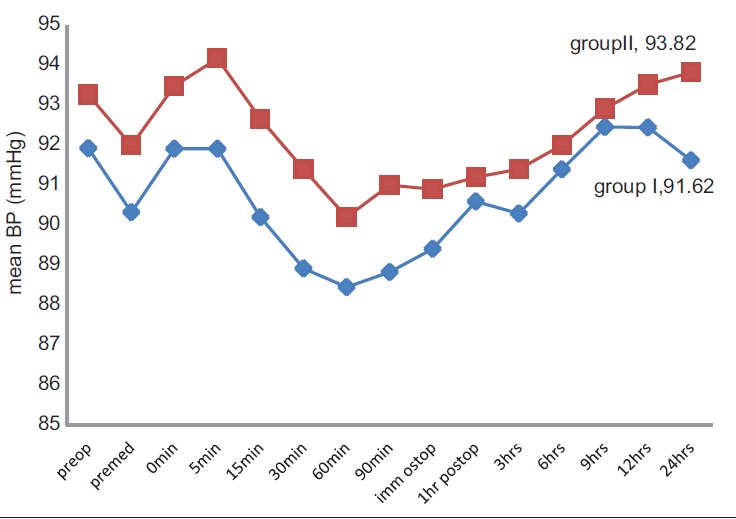
As shown in [Figure 1] mean arterial pressure does not show significant change between the two groups in preoperative, intraoperative and postoperative period, P values remained >0.05 (i.e., Not significant).
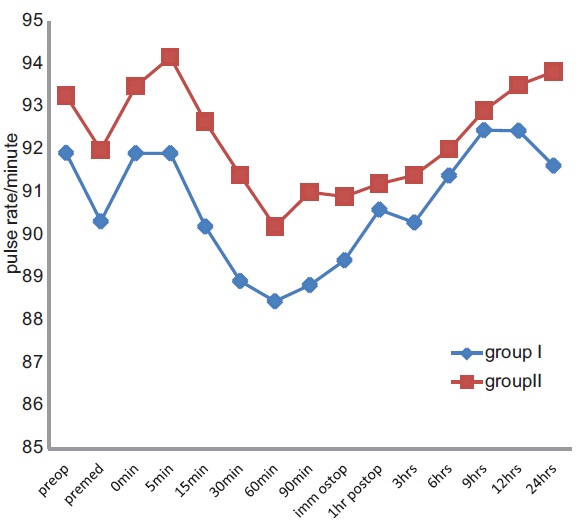
[Figure 2] shows mean pulse rate changes. Both groups did not show significant changes during preoperative, intraoperative and postoperative period. P values remained >0.05 (i.e., Not significant).
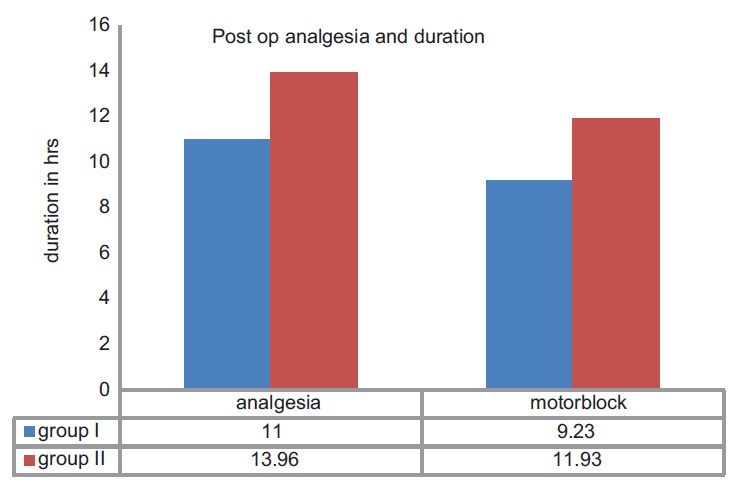
[Table 3] shows the duration of analgesia and motor blockade. Time of rescue analgesia was noted and was considered as duration of analgesia. It was 11.06 ± 2.67 h in Group-R and 13.96 ± 1.90 h in Group-RC. The results are statistically highly significant with P < 0.01. Duration of the motor blockade in Group-R was 9.23 ± 2.48 h and in Group-RC was 11.93 ± 1.94 h. It was statistically highly significant with P < 0.01.
[Figure 3] shows the duration of analgesia and motor blockade.
| Discussion | | |
Peripheral nerve blocks with local anesthetics provide excellent operating conditions with good muscle relaxation, but the duration of analgesia is rarely maintained for more than 6-8 h even with the longest acting available local anesthetic, that is, bupivacaine, so the search was on for an agent providing longer duration with minimum side effects. Ropivacaine has given some promising results in animal and human studies. [8]
Various studies has shown that several adjuvants like neostigmine, opioids, dexamethasone, hyaluronidase, tramadol with local anesthetic in peripheral nerve blocks prolonged the duration of analgesia, but the results have been inconclusive because of associated side effects or doubtful efficacy. [9],[10] Perineural injection of alpha 2 agonists is reported to influence postoperative analgesia. [11]
We found that the mean onset of sensory blockade was 10.06 min in Group-R and it was 11.86 min in Group-RC, so sensory blockade onset is delayed by adding clonidine, and it matches with the previous study. The mean time for sensory onset in both the previous studies was around 10 min in Group-R which was very much similar to our study. [12],[13],[14] The study showed that sensory onset time was around 10 min in most of the patients with ropivacaine, which was similar to our study but adding clonidine did not change the onset time, which is not in accordance with our study. [15] The duration of motor block was around 11 h with ropivacaine group and duration by adding clonidine was slightly more, which was not statistically significant, but with clonidine it was same as that of our study. [15]
The onset time for motor blockade with ropivacaine alone in our study started around 12 min, which is similar to the previous study. [12] The onset time of motor blockade with clonidine delayed in our study is similar to previous study, [13],[16] time for readiness for surgery was 14.5 min in ropivacaine group, which is also in accordance with our study. [17]
The duration of motor blockade with ropivacaine was 10 h in a previous study which is similar to our study. [13] The study showed that motor block improved from 9 h to 12 h, and analgesia from 10 h to 14 h. This is similar to our study wherein postoperative analgesia improved by 3 h and motor blockade improved by 2.7 h. [16] The mechanism of action for such potentiation of analgesia remains controversial and poorly understood. [12]
In other study, the duration of the motor blockade was 8 h, which is slightly less than our study, but they have used the axillary approach, which may be the reason for the varied results. [17]
The study showed that ropivacaine 0.75% for axillary brachial plexus anesthesia provided a 3 h delay in first analgesic request postoperatively, without clinically relevant effects on the degree of sedation and cardiovascular homeostasis, which is in accordance with our study. [13]
Both groups showed no significant hemodynamic changes intraoperatively or postoperatively, which is consistent with the previous studies. [12],[15] This is similar to the study in which ropivacaine with clonidine did not affect hemodynamic parameters. [16]
The longer duration of the motor blockade and postoperative analgesia in clonidine group could be due to the direct action of clonidine on nerve fiber conduction, specifically C and A delta fibers. However, this would require high local concentrations and would not explain why clonidine alone injected into the nerve sheath failed to produce prolonged analgesia. The action of clonidine would then more likely be via a synergistic mechanism of action in combination with the local anesthetic resulting in the prolonged effect. This is probably the only mechanism that would explain the extended duration of both the sensory and motor blockade. What is certain is that clonidine has mixed alpha1 and alpha 2 agonist effects at both pre and postsynaptic receptors as well as effects on a number of other specific receptors. Its mechanism of action and effects, therefore, are likely to be compound and complex. [18],[19],[20]
Our results showed that sensory block tended to last longer as compared to motor block, which agrees with the observation that large fibers require a higher concentration of local anesthetic than small fibers. The minimal effective concentration of local anesthetic for large (motor) fibers is greater than for small (sensory) fibers. Thus, motor function return before pain perception and duration of the motor block is shorter than the sensory block. [21]
| Conclusions | | |
Thus, we conclude from our study that, the ropivacaine is a novel, long-acting local anesthetic having moderate onset period and longer postoperative analgesia when used in a concentration of 0.75% (30 ml). The addition of clonidine 150 μm delays the onset of sensory and motor blockade while prolongs the duration of postoperative motor blockade and analgesia significantly without producing any clinical significant side-effects in brachial plexus block through supraclavicular approach.
| References | | |
| 1. | Hawkins JL, Koonin LM, Palmer SK, Gibbs CP. Anesthesia-related deaths during obstetric delivery in the United States. Anesthesiology 1997;86:277-84.  |
| 2. | Akerman B, Hellberg IB, Trossvik C. Primary evaluation of the local anaesthetic properties of the amino amide agent ropivacaine. Acta Anaesthesiol Scand 1988;32:571-87. |
| 3. | Casetti A, Bacierello M. Enantiomeric local anaesthetics, can ropivacaine and levobupivacaine improve our practice. Curr Drug Ther 2006;1:85-9. |
| 4. | Gaumann D. Comparison between clonidine and epinephrine admixture to lidocaine in brachialplexusblock. Anesth Analg 1992;75:69-74. |
| 5. | Stoelting RK, Hillier SC. Pharmacology and Physiology in Anesthetic Practic. 4 th ed. New York: Lippincott-Raven; 2005. p. 340-45. |
| 6. | Brown DL. Brachial plexus anesthesia: An analysis of options. Yale J Biol Med 1993;66:415-31. |
| 7. | Acalovschi I, Bodolea C, Manoiu C. Spinal anesthesia with meperidine. Effects of added alpha-adrenergic agonists: Epinephrine versus clonidine. Anesth Analg 1997;84:1333-9. |
| 8. | Rosemary Hickey, Kenneth D. Candido, Somayaji Ramamurthy. Brachial plexus block with a new local anaesthetic: 0.5 per cent ropivacaine. Can J Anesth. 1990;37:732-8. |
| 9. | Keeler JF, Simpson KH, Ellis FR, Kay SP. Effect of addition of hyaluronidase to bupivacaine during axillary brachial plexus block. Br J Anaesth 1992;68:68-71. |
| 10. | Kapral S, Gollmann G, Waltl B, Likar R, Sladen RN, Weinstabl C, et al. Tramadol added to mepivacaine prolongs the duration of an axillary brachial plexus blockade. Anesth Analg 1999;88:853-6. |
| 11. | Elliott S, Eckersall S, Fligelstone L, Jothilingam S. Does the addition of clonidine affect duration of analgesia of bupivacaine wound infiltration in inguinal hernia surgery? Br J Anaesth 1997;79:446-9. |
| 12. | Vaghadia H, Chan V, Ganapathy S, Lui A, McKenna J, Zimmer K. A multicentre trial of ropivacaine 7.5 mg x ml(-1) vs bupivacaine 5 mg x ml(-1) for supra clavicular brachial plexus anesthesia. Can J Anaesth 1999;46:946-51. |
| 13. | Casati A, Magistris L, Beccaria P, Cappelleri G, Aldegheri G, Fanelli G. Improving postoperative analgesia after axillary brachial plexus anesthesia with 0.75% ropivacaine. A double-blind evaluation of adding clonidine. Minerva Anestesiol 2001;67:407-12. |
| 14. | Casati A, Magistris L, Fanelli G, Beccaria P, Cappelleri G, Aldegheri G, et al. Small-dose clonidine prolongs postoperative analgesia after sciatic-femoral nerve block with 0.75% ropivacaine for foot surgery. Anesth Analg 2000;91:388-92. |
| 15. | Erlacher W, Schuschnig C, Koinig H, Marhofer P, Melischek M, Mayer N, et al. Clonidine as adjuvant for mepivacaine, ropivacaine and bupivacaine in axillary, perivascular brachial plexus block. Can J Anaesth 2001;48:522-5. |
| 16. | El Saied AH, Steyn MP, Ansermino JM. Clonidine prolongs the effect of ropivacaine for axillary brachial plexus blockade. Can J Anaesth 2000;47:962-7. |
| 17. | Bertini L, Tagariello V, Mancini S, Ciaschi A, Posteraro CM, Di Benedetto P, et al. 0.75% and 0.5% ropivacaine for axillary brachial plexus block: A clinical comparison with 0.5% bupivacaine. Reg Anesth Pain Med 1999;24:514-8. |
| 18. | Butterworth JF 5 th , Strichartz GR. The alpha 2-adrenergic agonists clonidine and guanfacine produce tonic and phasic block of conduction in rat sciatic nerve fibers. Anesth Analg 1993;76:295-301. |
| 19. | Gaumann DM, Brunet PC, Jirounek P. Clonidine enhances the effects of lidocaine on C-fiber action potential. Anesth Analg 1992;74:719-25. |
| 20. | Hutschala D, Mascher L, Schmetterer W, Klimscha T, Fleck H, Eichler G. et al. Clonidine added to bupivacaine enhances and prolongs analgesia after brachial plexus block via a local mechanism in healthy volunteers. Eur J Anesthesiol 2004;21:198-204. |
| 21. | Dejong RH, Wagman IH. Physiological mechanisms of peripheral nerve block by local anesthetics. Anesthesiology 1963;24:684-727. |
[Figure 1], [Figure 2], [Figure 3]
[Table 1], [Table 2], [Table 3]
|









 Search Pubmed for
Search Pubmed for