|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2015 | Volume
: 10
| Issue : 2 | Page : 63-67 |
|
Topical phenytoin for managing various ulcers: A meta-analysis
Pugazhenthan Thangaraju1, T Tamilselvan2, Sajitha Venkatesan3, T Eswaran4, Hosanna Singh1, VC Giri5, MK Showkath Ali6
1 Department of Clinical Division, Central Leprosy Teaching and Research Institute, MOHFW, GOI, Chengalpattu, Tamil Nadu, India
2 School Of Information Technology, SRMU, Sikkim, Tamil Nadu, India
3 General Physician, Tamil Nadu, India
4 Research scholar, TCE, Madurai, Tamil Nadu, India
5 Department of Epidemiology, Central Leprosy Teaching and Research Institute, MOHFW, GOI, Chengalpattu, Tamil Nadu, India
6 Director, MOHFW, GOI, Chengalpattu, Tamil Nadu, India
| Date of Web Publication | 16-Jul-2015 |
Correspondence Address:
Dr. Pugazhenthan Thangaraju
Central Leprosy Teaching and Research Institute, Ministry of Health and Family Welfare, Government of India, Chengalpattu - 603 001, Tamil Nadu
India
  | Check |
DOI: 10.4103/1858-5000.160951 
Objective: The aim of this meta-analysis was to evaluate the efficacy of topical phenytoin in the treatment of ulcers of different origin compared with other standard topical treatment. Methods: Randomized controlled trials were identified by searching PubMed, Embase, Medline, and Web of Science. Outcomes were complete wound healing rate and reduction in wound volume or surface area. Results: Thirteen studies with 980 patients were included. Topical phenytoin were associated with a statistically significant improvement of complete wound healing rate compared with other line of management in 11 randomized control trial of 815 patients (odds ratio = 3.03, 95% confidence interval 2.23-4.10, Z = 7.14, P < 0.00001). No publication bias exists in this meta-analysis. Three studies from India also confirmed that the topical phenytoin was associated with a statistically significant percent reduction in wound volume compared with the other dressing (mean difference 23.56, 95% confidence interval 19.48-27.64, Z = 11.32, P < 0.00001). Conclusion: The existent evidence shows that topical phenytoin is more effective for ulcer treatment. Keywords: Randomized control trial, topical phenytoin, ulcer, wound healing
How to cite this article:
Thangaraju P, Tamilselvan T, Venkatesan S, Eswaran T, Singh H, Giri V C, Showkath Ali M K. Topical phenytoin for managing various ulcers: A meta-analysis. Sudan Med Monit 2015;10:63-7 |
How to cite this URL:
Thangaraju P, Tamilselvan T, Venkatesan S, Eswaran T, Singh H, Giri V C, Showkath Ali M K. Topical phenytoin for managing various ulcers: A meta-analysis. Sudan Med Monit [serial online] 2015 [cited 2018 Sep 5];10:63-7. Available from: http://www.sudanmedicalmonitor.org/text.asp?2015/10/2/63/160951 |
| Introduction | |  |
Wounds with nonhealing and chronicity are a significant healthcare problem in today's medical practice. [1] Healing of wound is the process of restoration of the physical integrity of internal or external body structures, and it involves a complex interaction between the cells and various factors like the status of the patient, etc. [2] The healing process consists of: [2]
- An inflammatory response
- Regeneration of the epidermis
- Shrinkage of the wound
- Finally, connective tissue formation, and
- Remodeling.
Rational management of wound and caring accelerates the healing process and prevents mixed infection and chronicity of the wound. [3] Different approaches and methods have been used to achieve shorter complete wound healing times. [1] Various agents that have been tried in wound healing are phenytoin, honey, and amlodipine. Phenytoin was earlier introduced in 1937 as an antiseizure drug. [4] A common side effect with phenytoin is the gingival hypertrophy. [5] The stimulatory effect of phenytoin on the connective tissue by inhibiting collagenase enzyme suggested an exciting possibility for its use in wound healing. [3]
| Methods | | |
A search of PubMed and Web of Science, from their inception to February 28, 2015, included the terms "topical phenytoin," "ulcer," and "wound healing." The search detail in PubMed was (topical [all fields] and ["phenytoin" [MeSH terms] or "phenytoin" [all fields]) and (["wound healing" [MeSH terms] or ["wound" [all fields] and "healing" [all fields] or "wound healing" [all fields] and ["ulcer" [MeSH terms] or "ulcer" [all fields]). In the web of Science Citation Database, the authors selected the Science Citation Index Expanded and Conference Proceedings Citation Index Science databases. The authors supplemented the searches by manually reviewing the references of all relevant studies. Language restrictions were applied on these searches and only the English articles were used.
Study selection
The inclusion criteria included the following: Only randomized controlled trials (RCTs) were included, patients had an ulcer of different origin namely leprosy, diabetic, nonmalignant, pressure, burns and venous, topical phenytoin versus other management like Edinburgh University solution of lime, normal saline, silverex, were used in the treatment of ulcers, complete wound healing/appearances of granulation, and reduction in wound volume or surface area was achieved. Case reports, case series, single arm Phase I trials, retrospective case-control studies, and Phase II nonrandomized trials were excluded.
Quality assessment
Jadad scale was used to evaluate the study quality, which offers a score ranging from 1 to 5 based on the following parameters: Randomization (2), double-blinding (2), and withdrawals/dropouts at follow-up (1). A final score of 1-2 is defined as the low quality and 3-5 as high quality. [6] Two reviewers independently assessed the quality of each included study, and disagreements were resolved by discussion.
Data extraction
An initial form was used to extract data on first author, year of publication, country and number of patients, average duration of treatment, complete wound healing/granulation rate, and volume/surface area reduction in wound in two groups, respectively.
Statistical analysis
Statistical heterogeneity was explored by inconsistency (I 2) statistics. The values of 0-30% represented minimal heterogeneity, 31-50% moderate heterogeneity, and >50% substantial heterogeneity. [7] If there was minimal heterogeneity, a fixed effects model was used for meta-analysis, otherwise, a random effect model based on the DerSimonian and Laird estimator was used. [8] Summary odds ratio (OR) was calculated by taking a weighted average of individual study results. Two-sided P < 0.050 was considered statistically significant. Potential publication bias was tested by funnel graph. Analyses were all performed with RevMan 5.2.
| Results | | |
Eligible studies and quality
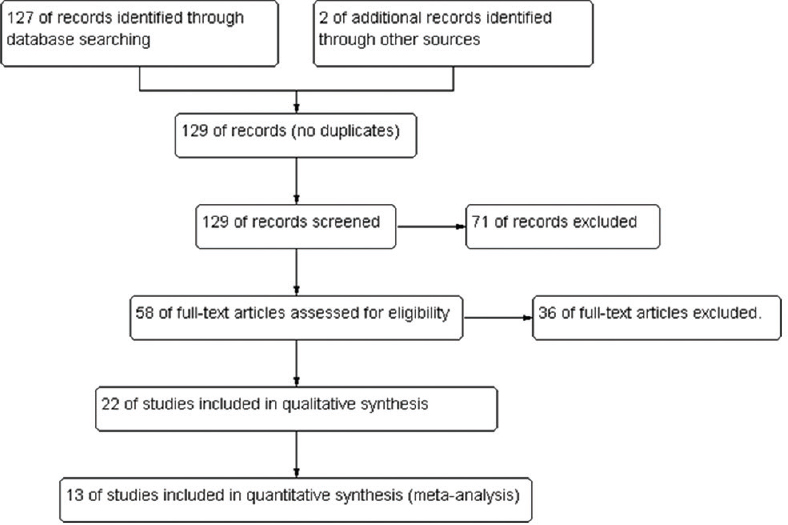
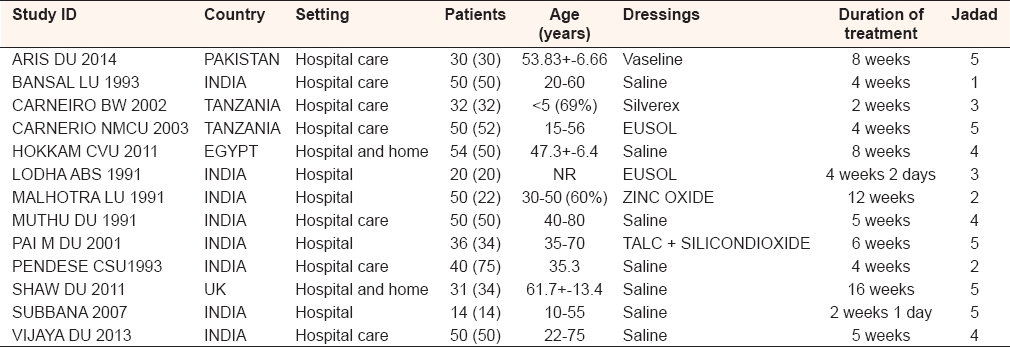
Thirteen RCT studies [9],[10],[11],[12],[13],[14],[15],[16],[17],[18],[19],[20],[21] that met the inclusion criteria for meta-analysis were identified. [Figure 1] shows the stages in identifying studies for inclusion in this analysis. Characteristics of the studies from the 13 articles included in the meta-analysis are shown in [Table 1]. Eight studies were conducted in India while Pakistan, Tanzania, Egypt, and UK contributed rest studies. Of the 13 studies, the sample sizes ranged from 28 to 104, the patients' age ranged from 15 to 80 years and in one study <5 years contributed 69%, the duration of treatment ranged from 2 weeks to 16 weeks. The Jadad scale of 10 included studies scored more than three, which indicated high quality. Eleven studies reported data on hospital care; the other two studies reported data on combined hospital and home care.
Complete wound healing rate in topical phenytoin versus other line of management
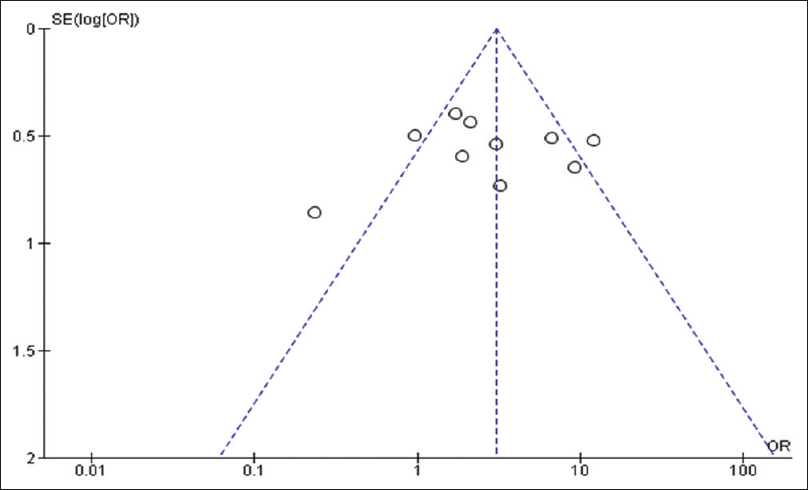
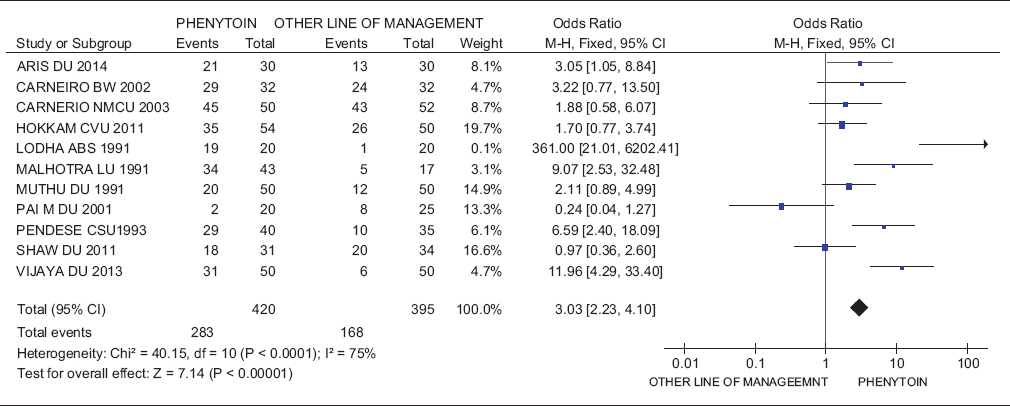
A total of 11 studies [9],[11],[12],[13],[14],[15],[16],[17],[18],[19],[21] provided sufficient data to analyze complete wound healing, which included 815 patients. The summary OR of the complete wound healing rate in patients treated with topical phenytoin compared with patients treated with other dressings was 3.03, 95% confidence interval 2.23-4.10, Z = 7.14, P < 0.00001 [Table 2]. Among those, six studies were done in India. [14],[15],[16],[17],[18],[21] Funnel plot showed the symmetrical distribution of the studies in this meta-analysis with two studies outlier [Figure 2].
Wound volume reduction in topical phenytoin group
Three studies [10],[14],[20] dealt with the percentage reduction of ulcer volume in response to topical phenytoin. Mean difference between the two groups in the three studies was 23.56 with 95% confidence interval of 19.48-27.64, Z = 11.32 with a value of P < 0.00001 [Table 3]. All the three studies were from India.
| Discussion | | |
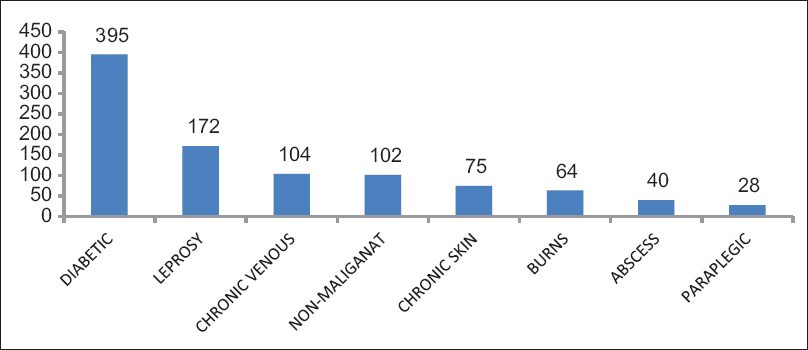
The aim of the meta-analysis was to determine the current evidence to support the use of topical phenytoin in wound healing by assessing the quality of RCTs in India and the rest of world. A systematic review [22] was done in 2007 for the period up to 2005.This meta-analysis includes studies up to 2015, to know any spectral change in the response of topical phenytoin after 2007, in increased sample sizes. The various category of wounds in our study includes diabetic (395), leprosy (172), burns (64), nonmalignant (102), chronic venous (104), abscess (40), chronic skin ulcer (75), and paraplegic ulcer (28) [Figure 3].
In any study, the sample size is crucial for the study to be sufficiently powered for detecting a true treatment effect. [23] In the 13 studies reviewed, sample size ranged from 28 to 104. An independent randomization process and adequate blinding are the important determinants that contribute to the overall strength of the study. The randomization process was adequately described in many studies, with subjects being randomized truly by an independent process. [9],[11],[12],[13],[14],[16],[17],[19],[20],[21] To minimize study bias, the concept of double-blinding has long been regarded as essential. In general in our meta-analysis, proper double-blinding was reported in 10 studies reported as above, in randomization.
Within the group of 13 studies, there was a similarity in the length of the study treatment period of <5 weeks in eight studies followed by 6, 8, 12, and 16 weeks in other studies. Majority of the studies considered an outcome measure involving complete healing and few studies focused on percentage reduction in wound volume over time. Five [8],[14],[15],[18],[21] of the 11 studies reported a statistically significant complete healing rate in the phenytoin-treated group when compared with the control groups in various wound types. Where possible, the calculation of a percentage reduction in ulcer volume in treatment effect also showed that the phenytoin-treated groups had a positive outcome in three studies. [10],[14],[20]
Two randomized controlled studies [24],[25] not included in this meta-analysis also showed some results in two extremes. One of the studies by Bhatia et al., [25] from India showed statistically significant improvement in complete healing and wound volume reduction in 2% and 4% topical phenytoin group which included 30 inpatients. A study [24] showed a negative response toward topical phenytoin when compared with hydrocolloids.
From this meta-analysis, it is seen that topical phenytoin have the property of wound healing in various category of ulcers. Hence, with this meta-analysis, strong evidence is generated in favor of topical phenytoin in different time period and with different population groups.
| Conclusion | | |
The existing evidence shows that topical phenytoin is more effective than other dressings for various ulcer treatments. Cost-wise also it has its own benefits.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Clark RA. Basics of cutaneous wound repair. J Dermatol Surg Oncol 1993;19:693-706.  |
| 2. | Alizadeh A, Mohagheghi M, Khaneki M, Saeed PK. A study of the effect of magnesium hydroxide on the wound healing process in rats. Med J Islam World Acad Sci 2007;16:165-70. |
| 3. | Anstead GM, Hart LM, Sunahara JF, Liter ME. Phenytoin in wound healing. Ann Pharmacother 1996;30:768-75. |
| 4. | Bhatia A, Prakash S. Topical phenytoin for wound healing. Dermatol Online J 2004;10:5. |
| 5. | Tripathi KD, editor. Antiepileptic drugs. Essentials of Medical Pharmacology. 6 th ed. New Delhi: Jaypee Brothers; 2008. p. 382-5. |
| 6. | Clark HD, Wells GA, Huët C, McAlister FA, Salmi LR, Fergusson D, et al. Assessing the quality of randomized trials: Reliability of the Jadad scale. Control Clin Trials 1999;20:448-52. |
| 7. | Higgins JP, Thompson SG. Quantifying heterogeneity in a meta-analysis. Stat Med 2002;21:1539-58. |
| 8. | DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986;7:177-88. [ PUBMED] |
| 9. | Ahmed A, Ahmed MI. A comparison of efficacy of topical use of phenytoin and vaseline gauze dressing with vaseline gauze dressing alone in healing of diabetic foot ulcers. J Postgrad Med Inst 2014;28:297-302. |
| 10. | Bansal NK, Mukul. Comparison of topical phenytoin with normal saline in the treatment of chronic trophic ulcers in leprosy. Int J Dermatol 1993;32:210-3. |
| 11. | Carneiro PM, Rwanyuma LR, Mkony CA. A comparison of topical Phenytoin with Silverex in the treatment of superficial dermal burn wounds. Cent Afr J Med 2002;48:105-8. |
| 12. | Carneiro PM, Nyawawa ET. Topical phenytoin versus EUSOL in the treatment of non-malignant chronic leg ulcers. East Afr Med J 2003;80:124-9. |
| 13. | Hokkam E, El-Labban G, Shams M, Rifaat S, El-Mezaien M. The use of topical phenytoin for healing of chronic venous ulcerations. Int J Surg 2011;9:335-8. |
| 14. | Lodha SC, Lohiya ML, Vyas MC, Bhandari S, Goyal RR, Harsh MK. Role of phenytoin in healing of large abscess cavities. Br J Surg 1991;78:105-8. |
| 15. | Malhotra YK, Amin SS. Role of topical phenytoin in trophic ulcers of leprosy in India. Int J Lepr Other Mycobact Dis 1991;59:337-8. [ PUBMED] |
| 16. | Muthukumarasamy MG, Sivakumar G, Manoharan G. Topical phenytoin in diabetic foot ulcers. Diabetes Care 1991;14:909-11. |
| 17. | Pai MR, Sitaraman N, Kotian MS. Topical phenytoin in diabetic ulcers: A double blind controlled trial. Indian J Med Sci 2001;55:593-9. [ PUBMED]  |
| 18. | Pendse AK, Sharma A, Sodani A, Hada S. Topical phenytoin in wound healing. Int J Dermatol 1993;32:214-7. |
| 19. | Shaw J, Hughes CM, Lagan KM, Stevenson MR, Irwin CR, Bell PM. The effect of topical phenytoin on healing in diabetic foot ulcers: A randomized controlled trial. Diabet Med 2011;28:1154-7. |
| 20. | Subbanna PK, Margaret Shanti FX, George J, Tharion G, Neelakantan N, Durai S, et al. Topical phenytoin solution for treating pressure ulcers: A prospective, randomized, double-blind clinical trial. Spinal Cord 2007;45:739-43. |
| 21. | Patil V, Patil R, Kariholu PL, Patil LS, Shahapur P. Topical phenytoin application in grade I and II diabetic foot ulcers: A prospective study. J Clin Diagn Res 2013;7:2238-40. |
| 22. | Shaw J, Hughes CM, Lagan KM, Bell PM. The clinical effect of topical phenytoin on wound healing: A systematic review. Br J Dermatol 2007;157:997-1004. |
| 23. | Polit DF, Hungler BP. Nursing Research, Principles and Methods. 6 th ed. Philadelphia: Lippincott Williams and Wilkins; 1995. p. 474. |
| 24. | Hollisaz MT, Khedmat H, Yari F. A randomized clinical trial comparing hydrocolloid, phenytoin and simple dressings for the treatment of pressure ulcers [ISRCTN33429693]. BMC Dermatol 2004;4:18. |
| 25. | Bhatia A, Nanda S, Gupta U, Gupta S, Reddy BS. Topical phenytoin suspension and normal saline in the treatment of leprosy trophic ulcers: A randomized, double-blind, comparative study. J Dermatolog Treat 2004;15:321-7. |
[Figure 1], [Figure 2], [Figure 3]
[Table 1], [Table 2], [Table 3]
|









 Search Pubmed for
Search Pubmed for