|
 
 |
| CASE REPORT |
|
| Year : 2015 | Volume
: 10
| Issue : 4 | Page : 137-139 |
|
Silent traumatic hernia
DS Nirhale, VS Athavale, Mohit Bhatia, Vishal Tomar
Department of General Surgery, Padmashree Dr. D. Y. Patil Hospital and Research Centre, Pune, Maharashtra, India
| Date of Web Publication | 15-Dec-2015 |
Correspondence Address:
Vishal Tomar
Prabhu Apartments, Opposite Union Bank, Near Bus Stop, Ulhasnagar, Thane - 421 001, Maharashtra
India
  | Check |
DOI: 10.4103/1858-5000.171866 
Incidence of abdominal trauma is on an increasing trend but abdominal content herniation due to blunt trauma is rare. Traumatic disruption of the abdominal wall has only about 50 reports worldwide, and only one from India. We report here a case of 65 year old male who underwent blunt trauma due to bull horn injury and presented with a swelling in the left lumbar quadrant of anterior abdominal wall, without as much as an abrasion on the overlying skin. We conclude that a low impact, prolonged presentation, case of traumatic abdominal wall hernia can be managed electively by open anatomical repair.
Keywords: Adult traumatic abdominal wall hernia, bull horn injury, traumatic abdominal wall hernia
How to cite this article:
Nirhale D S, Athavale V S, Bhatia M, Tomar V. Silent traumatic hernia. Sudan Med Monit 2015;10:137-9 |
| Introduction | |  |
The incidence of abdominal trauma is on an increasing trend, but abdominal content herniation due to blunt trauma is rare.[1] Most of the literature consists of handlebar injuries while riding two wheeler vehicles. It is postulated that abdominal wall hernia due to blunt trauma to abdomen accounts for not more than 2% of all traumatic hernia. Moreover, they are seen in the pediatric age group than the adult population.[2] Traumatic disruption of the abdominal wall has only about 50 reports worldwide and only one from India.[3] We report here a case of a 65-year-old male who underwent blunt trauma due to bull horn injury and presented with a swelling in the left lumbar quadrant of the anterior abdominal wall, without as much as an abrasion on the overlying skin.
| Case Report | | |
A 65-year-old male presented to the outpatient department with a chief complaint of pain in the abdomen along with swelling in the left lumbar and inguinal region for 10 days [Figure 1]. He gave a history of being hit by bullhorn after that he developed the swelling. On general examination, his pulse was 88 bpm, blood pressure 118/76 mm of Hg, respiratory rate 20/min, and afebrile. No evidence of clubbing, cyanosis, icterus, generalized edema, and lymphadenopathy. On local examination, the skin over the swelling was normal. No scar marks, pigmetation, ulceration or abrasion were seen. No visible peristalsis and no cough impulse present. Tenderness was present over the swelling. Borborygmi could be appreciated on trying to reduce the swelling, though the swelling was not reducible, only compressible. No local rise of temperature on systemic examination of the patient, there was tenderness around the region of swelling. No guarding or rigidity over the abdomen. No organomegaly. No evidence of an inguinal hernia on either side. We were suspecting bowel herniation into the anterior abdominal wall but were not convinced by the history given by the patient, as there was no scar or abrasion to be seen after a bull horn injury.
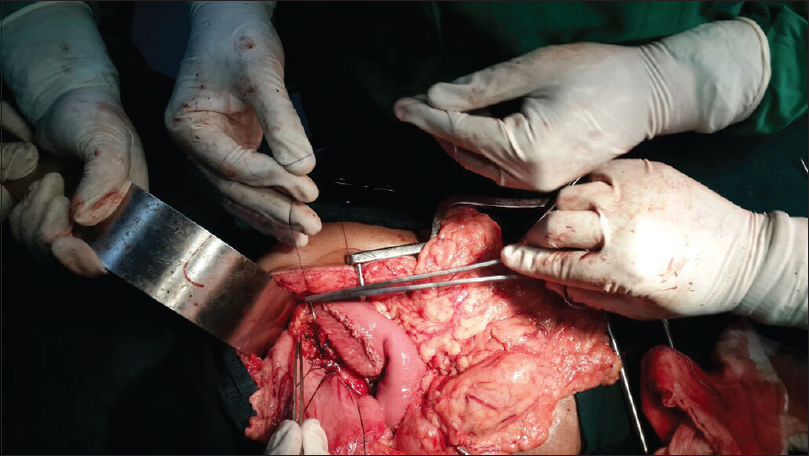
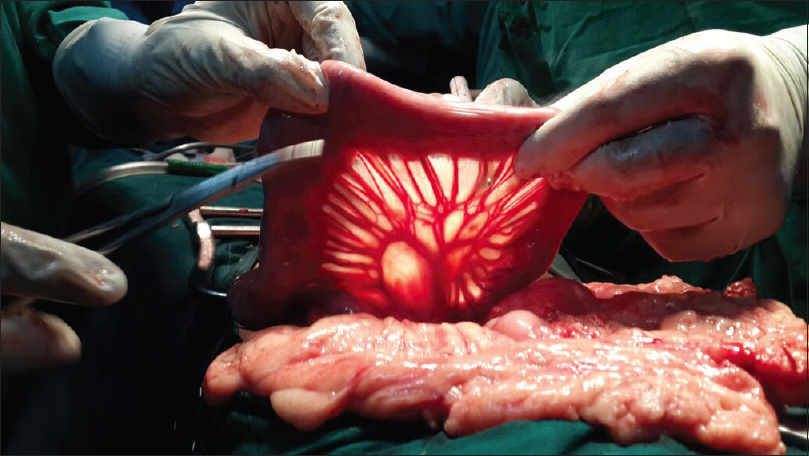
After workup for anesthesia and radiological opinion [Figure 2], the patient was operated on. The incision was taken above the swelling and beneath the subcutaneous layer; we found a small bowel herniating through a rent in the anterior abdominal wall musculature [Figure 3]. There was no evidence of edema or gangrene of the bowel. No evidence of adhesions surrounding the bowel. No perforation of the bowel [Figure 4]. The rent present in the musculature was used to reduce the bowel back into the abdominal cavity, and the abdominal cavity was checked for the presence of hemoperitoneum, blood clots, active bleeding, or other organ injury.
After being convinced of hemostasis being achieved, closure was done in layers. No colostomy was required. There was no need of prolene mesh being placed to cover the rent. The patient tolerated the procedure well. The patient was discharged on the 8th postoperative day.
| Discussion | | |
No disease of the human body, belonging to the province of the surgeon, requires in its treatment a better combination of accurate anatomical knowledge with surgical skill than hernia in all its varieties.
Sir Astley Paston Cooper (1804)
A hernia is a protrusion of a viscus or part of a viscus through an abnormal opening in the walls of its containing cavity.[4] Traumatic abdominal wall hernia (TAWH) is defined as herniation of viscera through the muscles and fascia of the abdominal wall with the overlying skin intact. Acute TAWHs are rare in occurrence. They result from a difference in elasticity between the skin and the layers of the anterior abdominal wall. The skin is more elastic than anterior abdominal wall structures.[5] TAWH was first described by Shelby in 1906.[6] TAWH is generally classified into three types. A small abdominal wall defect caused by low-energy trauma with small instruments (e.g., bicycle handlebar). A larger abdominal wall defect caused by high-energy transfer such as motor vehicle accident or a fall from a height. Intra-abdominal herniation of bowel with deceleration injuries (rare).[7] Such hernias are typically found in lower quadrants of the abdomen, especially after a high-velocity impact, probably due to the lack of rectus sheath in the lower half of abdomen for providing strength.[8] Most of the patients present shortly after trauma with swelling over the anterior abdominal at the site of injury. However, 26% patients also come with delayed presentation.[3] Our patient also presented 10 days after the day of injury. Computed tomography scan of the abdomen and pelvis after giving intravenous contrast helped in visualizing the herniated bowel contents into the anterior abdominal wall. There was no evidence of visceral organ injury. The management of delayed abdominal wall hernia in a hemodynamically stable patient is many folds and depends on various factors such as surgeon preference, comorbidities, fitness for surgery, and the presence of complications.[3] Despite the trend to use the laparoscopic approach in the treatment of incisional hernias, it infrequently practiced in the cases of TAWH.[9] Open surgery was selected in most of the reported cases in literature. Debates exist on whether to use a midline incision or an incision over the hernia. In the majority, the midline incision was chosen in acute cases to rule out associated intra-abdominal injury, which occurs in about 30–44% of patients in high-energy trauma.[8] While in low energy-induced TAWH, local exploration through an incision over the hernia is preferred.[7] In our patient, we preferred an open approach and performing the anatomical repair. The incision was taken over the swelling, as consistent with literature in cases of low impact blunt abdominal trauma patients.
| Conclusion | | |
A low impact, prolonged presentation case of TAWH can be managed electively by open anatomical repair.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Killeen KL, Girard S, DeMeo JH, Shanmuganathan K, Mirvis SE. Using CT to diagnose traumatic lumbar hernia. AJR Am J Roentgenol 2000;174:1413-5.  |
| 2. | Navaratnam R. Abdominal wall hernia following blunt trauma. Int J Case Rep Images 2012;3:26-8. |
| 3. | Kumar A, Hazrah P, Bal S, Seth A, Parshad R. Traumatic abdominal wall hernia: A reappraisal. Hernia 2004;8:277-80. |
| 4. | Williams S, Bulstrode C, O'Connel P. Bailey and Love's Short Practice of Surgery. 25 th ed. United Kingdom: Edward Arnold Ltd.; 2008. |
| 5. | Esposito TJ, Fedorak I. Traumatic lumbar hernia: Case report and literature review. J Trauma 1994;37:123-6. |
| 6. | Selby CD. Direct abdominal hernia of traumatic origin. JAMA 1906;47:1485. |
| 7. | Wood RJ, Ney AL, Bubrick MP. Traumatic abdominal hernia: A case report and review of the literature. Am Surg 1988;54:648-51. |
| 8. | Singh R, Kaushik R, Attri AK. Traumatic abdominal wall hernia. Yonsei Med J 2004;45:552-4. |
| 9. | Munshi IA, Ravi SP, Earle DB. Laparoscopic repair of blunt traumatic anterior abdominal wall hernia. JSLS 2002;6:385-8. |
[Figure 1], [Figure 2], [Figure 3], [Figure 4]
|











 Search Pubmed for
Search Pubmed for