|
 
 |
| ORIGINAL ARTICLE |
|
| Year : 2016 | Volume
: 11
| Issue : 1 | Page : 7-11 |
|
Blood pressure changes among children living at high altitude in South-Western Saudi Arabia
Humeda Suekit Humeda Mohammed Ahmed1, Mohammed El-Habib Mohammed Khalid1, Mansour Abdelgadir Ballal2, Fahaid Hassan Al-Hashem1
1 Department of Physiology, King Khalid University, College of Medicine, Abha, Saudi Arabia
2 Department of Physiology, College of Medicine, University of Science and Technology, Omdurman, Sudan
| Date of Web Publication | 10-Mar-2016 |
Correspondence Address:
Humeda Suekit Humeda Mohammed Ahmed
Department of Physiology, College of Medicine, King Khalid University, Abha
Saudi Arabia
  | Check |
DOI: 10.4103/1858-5000.178491 
Objective: To determine the effect of high altitude on systemic blood pressure (BP) among children. Subjects and Methods: About 145 school children from high altitude and 155 from low altitude were included in this study. Measurements of normal BP, body weight and height, triceps skin fold, waist circumference, and hematocrit value were made. Body mass index (BMI) was calculated from body weight and height, and the percentage of fat mass (FMP) was calculated from triceps skin fold measurement. Results: There was no difference in the mean age for high altitude and low altitude groups (12.46 ± 1.56 12.41 ± 1.52, respectively). Body weight and height were significantly higher in high altitude children than their counterparts at low altitude. The mean BMI values were not significantly different between the two groups. Children living at high altitude had significant higher systolic blood pressure (SBP) and diastolic blood pressure (DBP), hematocrit value, triceps skin fold, waist circumference, and FMP than those living at low altitude. There were positive significant correlations between SBP and DBP on one hand and body weight and height, BMI, FMP, waist circumference, triceps skinfold, and hematocrit values on the other hand. Conclusion: The significant difference in BP between the two groups was attributed to high body weight and height, body fat, and hematocrit value in the high altitude group. Keywords: Blood pressure, children, high altitude, Saudi Arabia
How to cite this article:
Ahmed HH, Mohammed Khalid ME, Ballal MA, Al-Hashem FH. Blood pressure changes among children living at high altitude in South-Western Saudi Arabia. Sudan Med Monit 2016;11:7-11 |
How to cite this URL:
Ahmed HH, Mohammed Khalid ME, Ballal MA, Al-Hashem FH. Blood pressure changes among children living at high altitude in South-Western Saudi Arabia. Sudan Med Monit [serial online] 2016 [cited 2017 Apr 22];11:7-11. Available from: http://www.sudanmedicalmonitor.org/text.asp?2016/11/1/7/178491 |
| Introduction | |  |
Previous studies of the effect of chronic hypoxia on blood pressure (BP) among children living permanently at high altitude have produced conflicting results. It has been reported that children (6-20 years) living permanently at high altitude areas had lower BPs than comparable individuals living at sea level. [1] However, Arslan et al. found that the mean systolic BP (SBP) and diastolic BP (DBP) were higher among high altitude children than low altitude ones.
In South-Western part of Saudi Arabia, Khalid et al. found that BP was higher among adults living at high altitude compared to those living at low altitude. [2],[3] To the best of our knowledge, no study was performed to determine the effect of high altitude residence on BP in children in this area. This study was aimed to determine the effect of high altitude on BP of children living at high altitude areas in South-Western Saudi Arabia. In addition, to investigate any possible relationship of body weight and height, body mass index (BMI), body fat, and hematocrit value to BP.
| Subjects and Methods | | |
This prospective study was carried out at the high- and low-altitude areas of the Assir Province in the South-Western part of the Kingdom of Saudi Arabia. Two villages - Al Soda and Alsoga located at 3150 m with a barometric pressure of 550 mmHg were selected for the study. These villages are located at the highest point of the kingdom. For comparison, Alraish and Al-Khataresh located at a low altitude of 500 m (barometric pressure 720 mmHg) were selected to represent low altitude residence. Environmental data on these areas are shown in [Table 1]. [4]
Health services to the area involved in the study are provided by primary health care centers run by qualified physicians who used two referral hospitals with good access roads. Meat, chicken, and rice constitute the major dietary items for the people living in the two localities. This study was approved by the Ethical Committee of the College of Medicine at King Khalid University.
The data were collected from 145 school children and adolescents aged 10-15 years who were born and living permanently at high altitude and 155 school children of comparable age born and living permanently at low altitude. Each child was first subjected to detailed clinical examination and children with abnormal clinical examination, as well as children who were not born and who did not live permanently in the designated study areas, were excluded from this study. All subjects were Arab and of Saudi nationality. All measurements were taken in the health centers. The body weight was measured with an Avery beam weighing scale and the standing height was measured with a stadiometer SECA 213 portable stadiometer. The weights of the children in minimal clothing were taken to the nearest 0.1 kg, and the heights were taken without shoes to the nearest 0.5 cm. The BMI was calculated from the formula: Weight (kg)/height (m 2 ). The percentage of fat mass (FMP) was calculated from triceps skin fold measurements using the following equation: [5]
FMP = 6.77 + 1.26 TSF
SBP and DBP were measured by attending physicians in the health centers using mercurial sphygmomanometer.
A venous blood sample was then taken for determination of hematocrit value which was performed by lab technicians in the health centers, using microhematocrit centrifuge and packed cell volume reader.
Statistical analysis
The collected data were compiled and fed into IBM computer. SPSS version 20 (IBM company) was used for standard statistical analysis. Descriptive data were presented as means and standard deviations of means or percentages. The Student's t-test was used to compare between two means. Spearman's correlation coefficient was used to test for association between two variables. P < 0.05 was considered significant.
| Results | | |
The total number of subjects involved in this study at high and low altitudes were 145 and 155, respectively, with equal response rate of 95%.
[Table 2] shows the number of children by sex and their mean ages at high and low altitudes. Sixty-nine percent of the sample from high altitude were boys and 31% were girls. The respective percentages in the sample from low altitude were 70.3% and 29.7%. There were significant differences between the percentage of boys and girls at the same altitude (P < 0.001 for both), but there were no significant differences between the percentage of boys and girls at high altitude and their respective sexes at low altitude (P = 0.79 for boys, <0.89 for girls). There were no significant differences in the mean ages between boys and girls at high altitude and their respective groups at low altitude (P < 0.76 for all).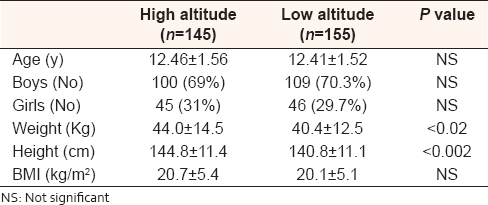 | Table 2: Mean Values of age, gender and anthropometric measurements of children living at high and low altitude
Click here to view |
Body weight and height were significantly greater among highlanders than lowlanders (P < 0. 02 and <0.002, respectively). The average weight and height of the high altitude group were 44.0 kg and 144.8 cm, respectively, while the average weight and height of the low altitude group were 40.4 kg and 140.8 cm, respectively.
Although the BMI was slightly greater at high altitude than at low altitude, the difference was not statistically significant (P < 0.32).
Children living at high altitude were found to have significant higher SBP and DBP than those living at low altitude (P < 0.001 for both). The hematocrit value was greater among high altitude group than low altitude group (P < 0.001) [Table 3].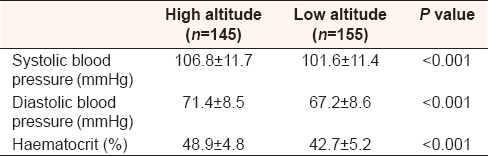 | Table 3: Mean values and standard deviations (SD) of the systolic and diastolic blood pressure and haematocrit value among children living at high and low altitude
Click here to view |
[Table 4] shows that the mean waist circumference was significantly greater at high altitude compared to low altitude (P < 0.005). Children living at high altitude were found to have significantly greater triceps skinfold thickness than their counterparts living at low altitude (P < 0.003). The FMP was significantly greater in the high altitude group than at low altitude one (P < 0.01).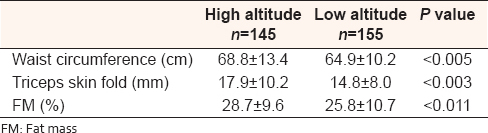 | Table 4: Mean values and standard deviations of waist circumference, triceps skinfold and fat mass percent of children living at high and low altitude
Click here to view |
There were significant positive correlations between both SBP and DBP and hematocrit value [Figure 1].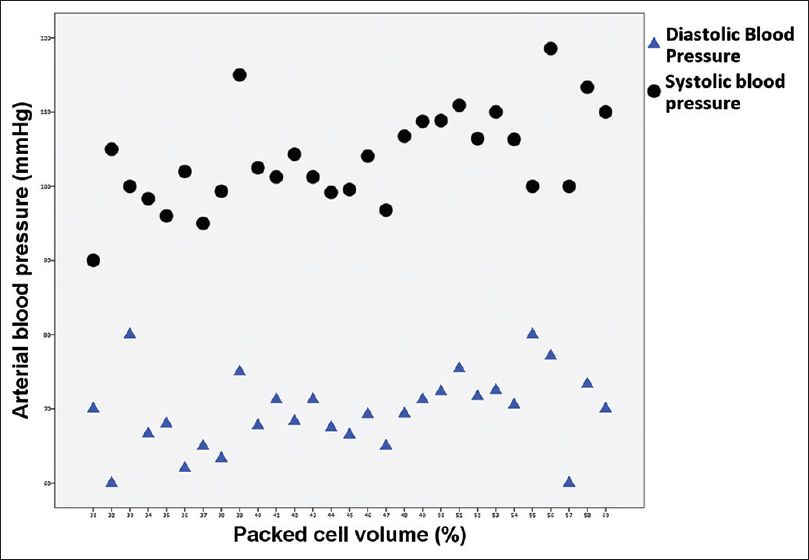 | Figure 1: Correlations between systolic and diastolic blood pressure with haematocrit value
Click here to view |
Both SBP and DBP had significant positive correlations with body weight, body height, and BMI [Figure 2].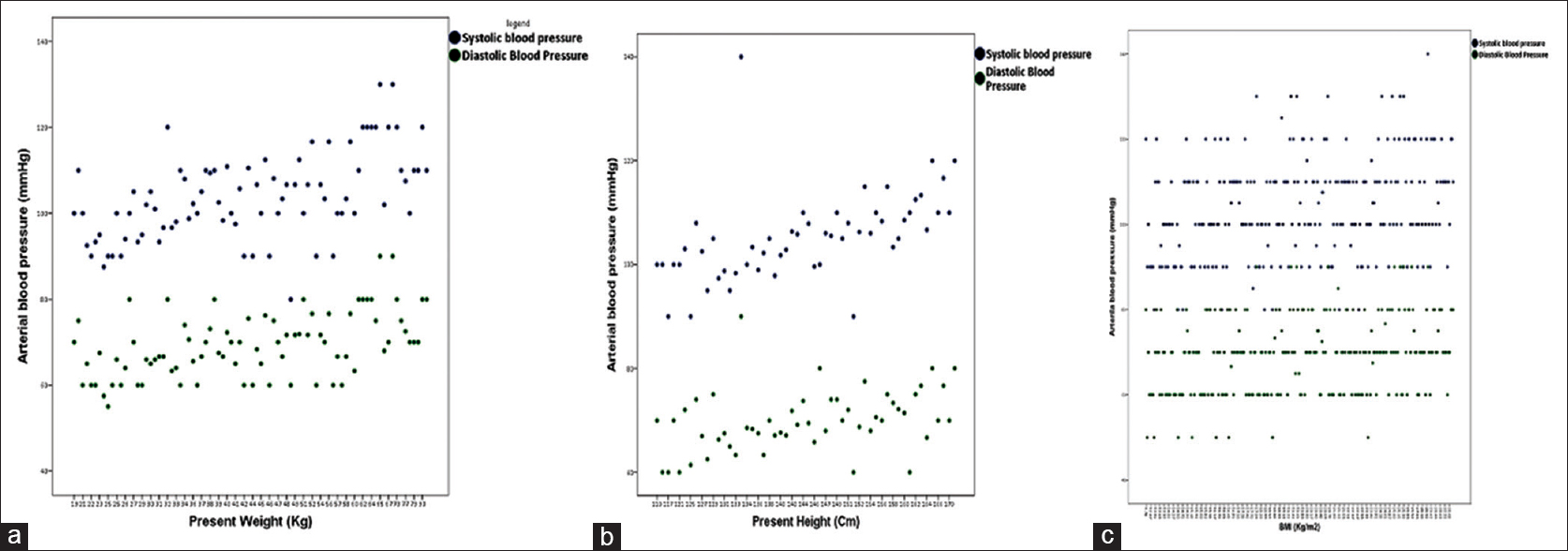 | Figure 2: Correlations between systolic and diastolic blood pressure with body weight (a) body height (b) and BMI (c)
Click here to view |
There were significant positive correlations between both SBP and DBP and triceps skin fold, waist circumference, and FMP [Figure 3].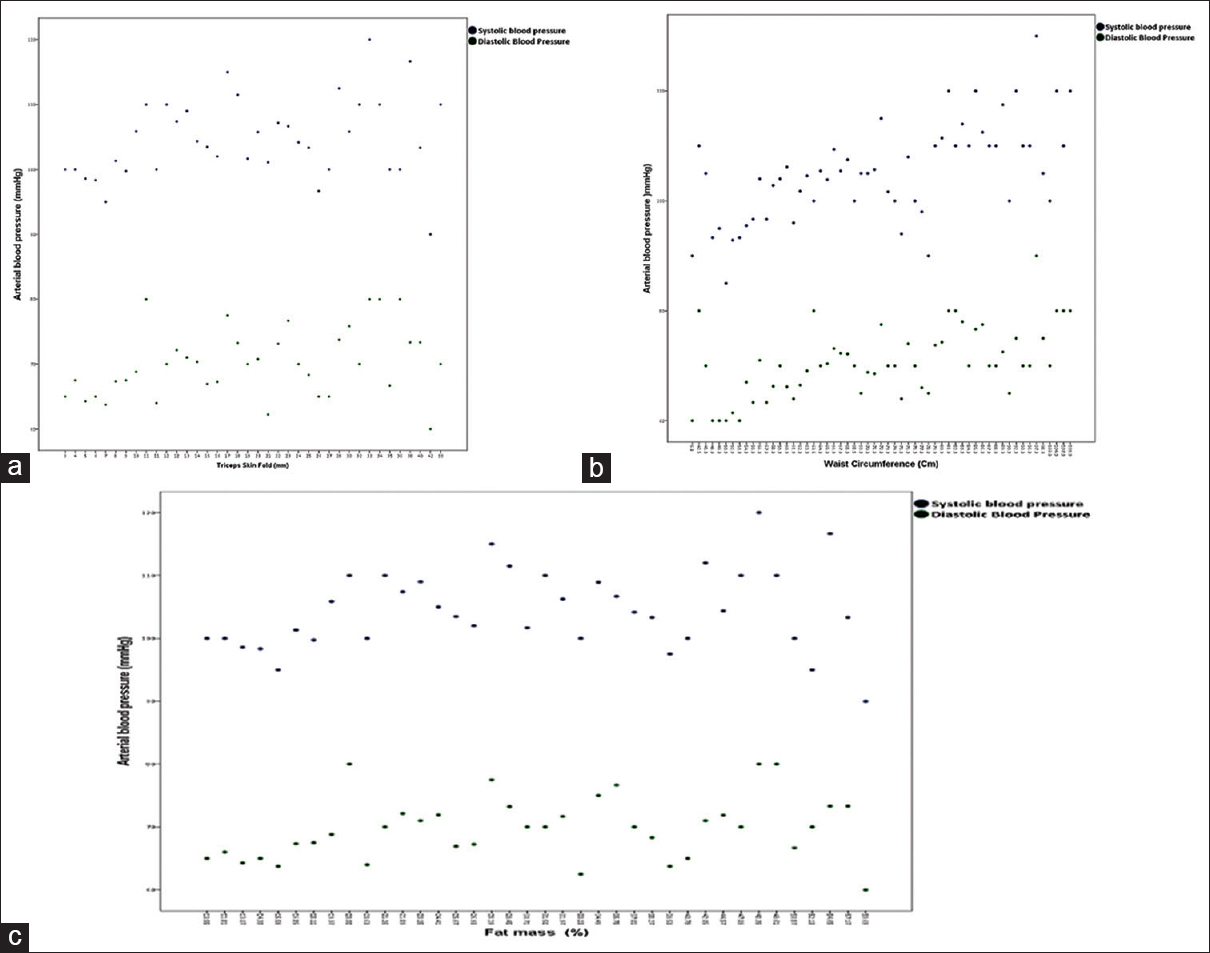 | Figure 3: Correlations between systolic and diastolic blood pressure with triceps skin fold (a) waist circumference (b) and fat mass percent (c)
Click here to view |
| Discussion | | |
Hypobaric hypoxia caused by high altitude is associated with many adaptive mechanisms such as increased hematocrit value, hemoglobin concentration, plasma volume, and cardiac output. However, chronic hypoxia at high altitude can relax systemic peripheral vascular smooth muscles leading to a drop in peripheral resistance and hence lowering of BP. Our present study showed that SBP and DBP were higher among high altitude children than low altitude ones, and there was a significant positive relationship between altitude and BP. These findings are consistent with other investigators who reported increased BP among children living at high altitude. [6] But, at variance with others who reported low BP at high altitude. [7] However, these studies, which reported low BP among children living at high altitude showed that the BP was similar when corrected for body weight and height between high and lowlanders. [7] In addition, in these studies, socioeconomic conditions were different between the two study groups.
The high BP observed among children living at high altitude may be due to greater effects of high altitude on body weight and height, blood viscosity, and cardiac output than on peripheral vasodilation. Another explanation is insufficient vascular adaptive changes at this age group since high altitude did not result in hypertension in adults. [6]
Our study supported the findings of the previous studies which found that hematocrit value was greater at high altitude than at low altitude, which was attributed to the stimulatory effect of hypoxia on erythropoietin secretion. [8] High hematocrit value can increase peripheral resistance and hence BP. Indeed, our study showed that BP was significantly and positively associated with hematocrit value. Hence, one of the possible mechanisms by which high altitude can increase BP is by increasing the hematocrit value.
Our study showed that children living at high altitude had higher body weight and height than those living at low altitude. This is in agreement with published work in the area [9],[10] and worldwide, [11],[12],[13] but in contrast to other studies that reported the growth retarding the effect of high altitude in children. [14],[15],[16] The differences in body weight and height between the two group were attributed to lower physical activity and lesser risk for tropical infections at high altitude. [17],[18] Our study reconfirmed the significant positive correlations between body weight and height and BP, which were reported by previous studies. [19],[20] In view of such correlations, the high BP among high altitude group observed in this study can be explained by the effect of high altitude on body weight and height.
It is well documented that when BMI increases to obesity levels, hypertension develops. [21] However, as there was no significant difference in the BMI between the two groups, and therefore, BMI cannot be considered as one of the risk factors for high BP observed among high altitude children in this study.
Our study showed that the waist circumference, triceps skinfold, and FMP were greater among high altitude group compared to low altitude group. These findings are in consistent with previous studies which reported high prevalence of central and total obesity among high land children, which was explained by low physical activity at high altitude. [10],[17] Both central and total obesity were found to be significantly associated with cardiovascular diseases and high BP in children. [22],[23],[24] Hence, one of the possible mechanisms by which high altitude can raise BP is by increasing fat deposition centrally and peripherally.
| Conclusion | | |
High altitude is associated with high SBP and DBP in children. This high BP may be explained by the effect of high altitude on blood viscosity, body weight, body height, and body fat.
Acknowledgment
The authors would like to thank all the medical and administrative staff in Asoda, Tabab, Alsoga, Alraish, and Al-Khataresh primary health care centers. They thank also to Mr. Mohammed Al-Ahmri for blood samples' analysis.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
| References | | |
| 1. | Wolfe RR, Murphy JR. Chronic high altitude residence and systemic blood pressure in school-aged children. Pediatr Res 1978;12:391.  |
| 2. | Khalid ME, Ali ME, Ahmed EK, Elkarib AO. Pattern of blood pressures among high and low altitude residents of Southern Saudi Arabia. J Hum Hypertens 1994;8:765-9. |
| 3. | Khalid ME, Adzaku FK. The effect of altitude on blood pressure in the Assir Province of Saudi Arabia. Wilderness Environ Med 1995;6:401-6. |
| 4. | Ministry of Agriculture and Water. Water Atlas of Saudi Arabia. Ministry of Agriculture and Water Publication. Riyadh: Saudi Arabia. 1984. p. 1-100. |
| 5. | Bray GA, DeLany JP, Harsha DW, Volaufova J, Champagne CC. Evaluation of body fat in fatter and leaner 10-y-old African American and white children: The Baton Rouge children's study. Am J Clin Nutr 2001;73:687-702. |
| 6. | Arslan S, Arslan N, Soylu A, Akgün C, Tepebasili I, Türkmen M, et al. High altitude and blood pressure in children. Yale J Biol Med 2003;76:145-8. |
| 7. | Jongbloed LS, Hofman A. Altitude and blood pressure in children. J Chronic Dis 1983;36:397-404. [ PUBMED] |
| 8. | Al-Hashem FH. Pattern of haemoglobin among high and low altitude children of Southwestern Saudi Arabia. J Family Community Med 2006;13:35-40. |
| 9. | Khalid ME, Al-Hashem FH. The relationship of body weight to altitude in preschool children of Southwestern Saudi Arabia. J Family Community Med 2007;14:71-6. |
| 10. | Khalid Mel H. Is high-altitude environment a risk factor for childhood overweight and obesity in Saudi Arabia? Wilderness Environ Med 2008;19:157-63. |
| 11. | Clegg EJ, Pawson IG, Ashton EH, Flinn RM. The growth of children at different altitudes in Ethiopia. Philos Trans R Soc Lond B Biol Sci 1972;264:403-37. [ PUBMED] |
| 12. | Kaul S, Kaul HN. Ladakh Through the Ages, Towards a New Identity. 1 st ed. New Delhi: Indus Publishing; 1992. p. 368. |
| 13. | Weitz CA, Garruto RM, Chin CT, Liu JC, Liu RL, He X. Morphological growth of Han boys and girls born and raised near sea level and at high altitude in Western China. Am J Hum Biol 2000;12:665-81. |
| 14. | Frisancho AR. Developmental responses to high altitude hypoxia. Am J Phys Anthropol 1970;32:401-7. [ PUBMED] |
| 15. | Harris NS, Crawford PB, Yangzom Y, Pinzo L, Gyaltsen P, Hudes M. Nutritional and health status of Tibetan children living at high altitudes. N Engl J Med 2001;344:341-7. |
| 16. | Tripathy V, Gupta R. Growth among Tibetans at high and low altitudes in India. Am J Hum Biol 2007;19:789-800. |
| 17. | Mahfouz AA, Shatoor AS, Khan MY, Daffalla AA, Mostafa OA, Hassanein MA. Nutrition, physical activity, and gender risks for adolescent obesity in Southwestern Saudi Arabia. Saudi J Gastroenterol 2011;17:318-22. [ PUBMED]  |
| 18. | Annobil SH, Okeahialam TC, Jamjoom GA, Bassuni WA. Malaria in children - Experience from Asir region, Saudi Arabia. Ann Saudi Med 1994;14:467-70. |
| 19. | Ma J, Wang Z, Dong B, Song Y, Hu P, Zhang B. Quantifying the relationships of blood pressure with weight, height and body mass index in Chinese children and adolescents. J Paediatr Child Health 2012;48:413-8. |
| 20. | Abdulle A, Al-Junaibi A, Nagelkerke N. High blood pressure and its association with body weight among children and adolescents in the United Arab Emirates. PLoS One 2014;9:e85129. |
| 21. | Livshits G, Gerber LM. Familial factors of blood pressure and adiposity covariation. Hypertension 2001;37:928-35. |
| 22. | Freedman DS, Srinivasan SR, Harsha DW, Webber LS, Berenson GS. Relation of body fat patterning to lipid and lipoprotein concentrations in children and adolescents: The Bogalusa heart study. Am J Clin Nutr 1989;50:930-9. |
| 23. | Daniels SR, Morrison JA, Sprecher DL, Khoury P, Kimball TR. Association of body fat distribution and cardiovascular risk factors in children and adolescents. Circulation 1999;99:541-5. |
| 24. | Goran MI, Ball GD, Cruz ML. Obesity and risk of type 2 diabetes and cardiovascular disease in children and adolescents. J Clin Endocrinol Metab 2003;88:1417-27. |
[Figure 1], [Figure 2], [Figure 3]
[Table 1], [Table 2], [Table 3], [Table 4]
|









 Search Pubmed for
Search Pubmed for